Atrial Flutter
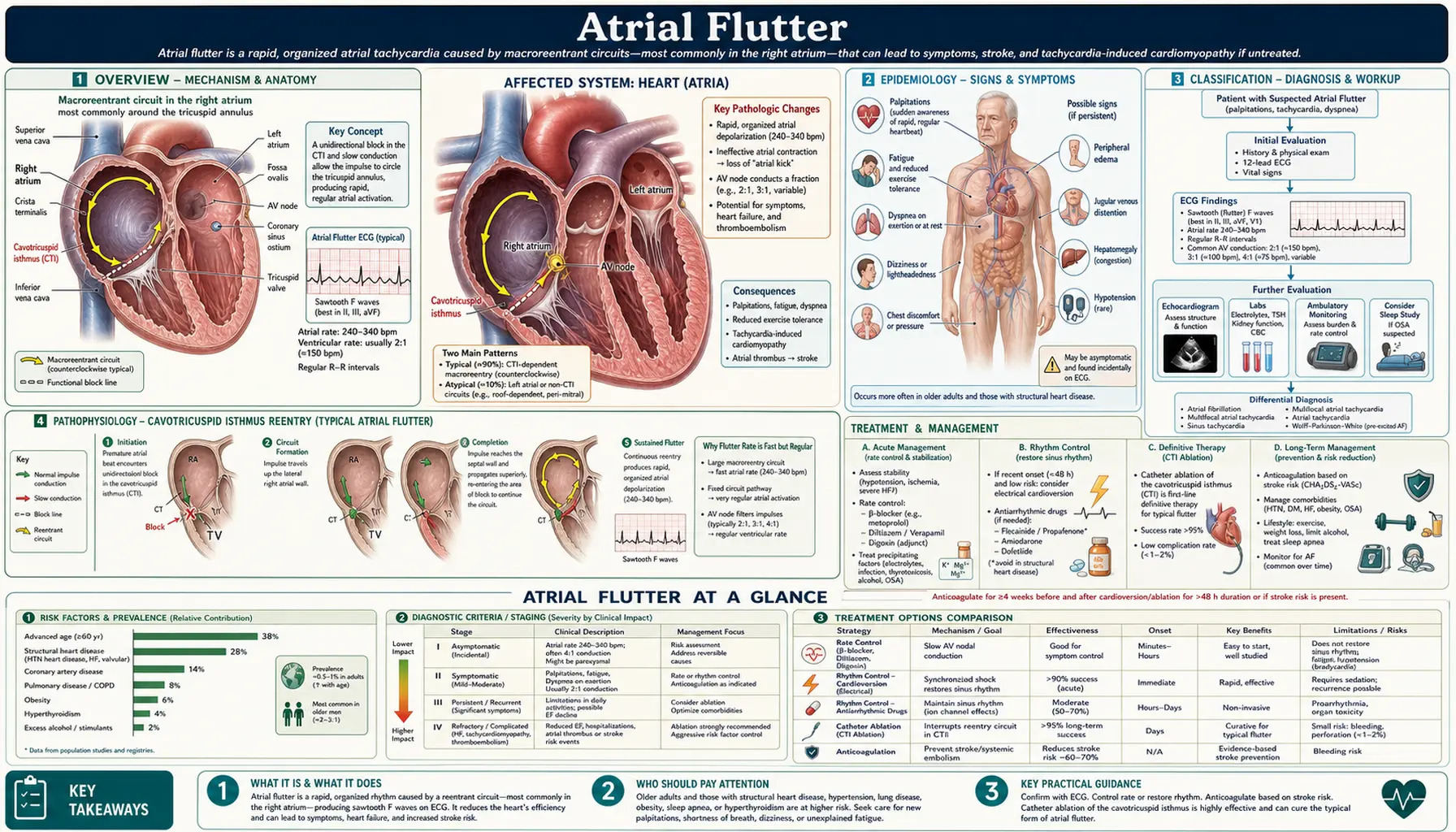
Table of Contents
- Overview
- Epidemiology
- Classification (Typical vs Atypical Flutter)
- Pathophysiology (Cavotricuspid Isthmus Reentry)
- Clinical Presentation
- Diagnosis and ECG Features
- Rate Control
- Cardioversion and Anticoagulation
- Catheter Ablation (CTI Ablation)
- Thromboembolic Risk and Prevention
- Research Papers
- Connections
- Featured Videos
1. Overview
Atrial flutter (AFL) is a macro-reentrant atrial arrhythmia characterized by rapid, organized atrial electrical activity at approximately 250–350 beats per minute, most commonly around 300 bpm. Unlike atrial fibrillation with its chaotic, disorganized activity, atrial flutter maintains a regular, organized circuit — producing the distinctive "sawtooth" flutter wave pattern on ECG.
Typical atrial flutter (type I, common flutter) is the most prevalent form, driven by a counterclockwise reentrant circuit in the right atrium dependent on the cavotricuspid isthmus (CTI) — a narrow corridor of myocardium between the inferior vena cava and the tricuspid annulus. This CTI-dependent nature makes typical flutter exquisitely amenable to catheter ablation, with cure rates exceeding 95%.
AFL occupies a distinct but interrelated position with atrial fibrillation on the arrhythmia spectrum: the two conditions frequently coexist, share common risk factors, and carry similar thromboembolic risk. Approximately 50–80% of atrial flutter patients will develop AF over time.
2. Epidemiology
Atrial flutter has an estimated prevalence of 200,000 in the United States, with an annual incidence of approximately 88 per 100,000 person-years. Incidence increases sharply with age: the annual incidence in those over 80 approaches 587 per 100,000. Men are affected 2.5 times more frequently than women.
Risk factors parallel those of AF: age, hypertension, coronary artery disease, heart failure, obesity, diabetes, chronic obstructive pulmonary disease, obstructive sleep apnea, and excessive alcohol consumption. AFL is particularly prevalent post-cardiac surgery (25–35% of patients) and after pulmonary vein isolation procedures for AF, where scar tissue can create new reentrant circuits (incisional flutter).
3. Classification
Typical AFL (Type I, CTI-dependent, counterclockwise): The dominant form (>90% of AFL). The circuit rotates counterclockwise in the right atrium (as viewed in left anterior oblique fluoroscopic projection): ascending the right atrial septum (interatrial septum), across the roof, descending the right atrial free wall (crista terminalis acts as a functional posterior barrier), and pivoting around the tricuspid annulus isthmus (CTI). ECG shows negative sawtooth F waves in inferior leads (II, III, aVF) and positive F waves in V1.
Clockwise (reverse typical) AFL: Same CTI-dependent circuit but rotating clockwise — producing positive flutter waves in inferior leads and negative in V1. Less common (~10% of typical AFL).
Atypical AFL (Type II, non-CTI-dependent): Reentrant circuits not dependent on the CTI. Includes: perimitral flutter (circuit around mitral annulus), roof-dependent flutter, left atrial flutter, incisional flutter (scar-dependent after cardiac surgery or ablation). Typically requires advanced electroanatomical mapping for characterization.
4. Pathophysiology (Cavotricuspid Isthmus Reentry)
The cavotricuspid isthmus forms the critical bridge in typical AFL. It is bounded anteriorly by the tricuspid annulus (electrically inexcitable) and posteriorly by the inferior vena cava (inexcitable). The isthmus is typically 20–40 mm wide and 30–50 mm long, with slow and non-homogeneous conduction properties that allow the reentrant circuit to sustain.
The crista terminalis serves as a line of functional block along the posterior right atrial wall, preventing short-circuiting of the circuit and forcing the wavefront to travel the full path around the tricuspid annulus.
At 300 bpm atrial rate, the AV node typically conducts every other flutter wave — producing 2:1 AV block and a ventricular rate of approximately 150 bpm. This ventricular rate of 150 bpm is a highly specific clinical finding for flutter and should trigger immediate suspicion. 4:1 block (ventricular rate ~75 bpm) occurs spontaneously or after rate-control drugs. Variable AV block can produce an irregular ventricular response.
AFL-AFib continuum: Both arrhythmias share pathophysiologic substrates (atrial fibrosis, stretch, inflammation). Pulmonary vein triggers can initiate AF; the organized CTI circuit sustains flutter. AFL can degenerate into AF and vice versa, particularly after pharmacologic cardioversion where flutter may slow sufficiently to permit AFib triggers.
5. Clinical Presentation
Clinical features are similar to AFib but with important distinctions:
- Palpitations — often described as a rapid, regular "fluttering"
- Dyspnea and reduced exercise tolerance
- Fatigue and lightheadedness
- Chest discomfort
- Ventricular rate of ~150 bpm is a classic presenting heart rate suggesting 2:1 AFL until proven otherwise
AFL may present asymptomatically (discovered incidentally) or with hemodynamic instability (particularly in patients with structural heart disease or when ventricular rates are very rapid: 1:1 conduction with rates of 300 bpm can occur with class IC drugs like flecainide that slow atrial rate but paradoxically enable 1:1 conduction — medical emergency).
Carotid sinus massage or adenosine can transiently increase AV block (2:1 → 4:1 → 8:1), dramatically slowing the ventricular rate and unmasking the sawtooth flutter waves — an important diagnostic maneuver.
6. Diagnosis and ECG Features
The 12-lead ECG is diagnostic:
- Sawtooth flutter waves (F waves): Regular, organized atrial activity at ~300 bpm (range 250–350 bpm). Negative, saw-toothed appearance in inferior leads (II, III, aVF) in typical counterclockwise AFL. F waves are continuous without isoelectric baseline between deflections — distinguishing from P waves with intervening isoelectric periods.
- 2:1 AV block: Most common; ventricular rate ~150 bpm. F waves may be partially hidden within QRS or T waves, making diagnosis difficult. Long rhythm strip (V1) helps identify hidden F waves.
- Regular ventricular response (unless variable block or aberrant conduction is present)
- QRS narrow unless bundle branch block or pre-excitation
Carotid massage/adenosine transiently blocks AV conduction, increasing block ratio and making F waves clearly visible.
Differential Diagnosis
- Atrial fibrillation: irregular ventricular response, no organized F waves
- AVNRT/AVRT at ~150 bpm: narrow complex, P waves in or after QRS
- Sinus tachycardia: upright P waves in inferior leads, rate increases/decreases gradually
- Atrial tachycardia: distinct P waves with isoelectric intervals
7. Rate Control
Rate control in AFL is often more difficult to achieve than in AFib because the regular organized flutter circuit is less susceptible to drug-induced disruption of conduction. Medications that slow AV nodal conduction may be needed in high doses:
- Beta-blockers: Metoprolol, atenolol — preferred for long-term rate control
- Non-dihydropyridine CCBs: Diltiazem IV or verapamil IV for acute rate control; oral forms for chronic management
- Digoxin: Less effective for AFL than AFib; may help in heart failure
Warning — Class IC drugs (flecainide, propafenone) alone: These drugs slow the flutter rate from ~300 to ~200 bpm without blocking the AV node — potentially enabling 1:1 AV conduction at 200 bpm, causing extreme tachycardia and hemodynamic collapse. Always co-administer AV nodal blocking drugs if Class IC agents are used.
8. Cardioversion and Anticoagulation
Electrical cardioversion: Atrial flutter is highly responsive to DC cardioversion. Low energy shocks (50–100 J biphasic) achieve cardioversion in >95% of cases — AFL requires less energy than AF. Synchronized mode is essential.
Pharmacologic cardioversion: Ibutilide (class III, 1 mg IV over 10 minutes, repeat once) converts flutter in ~60% of cases; risk of torsades de pointes requires monitored setting with QTc correction pre-treatment. Dofetilide is an alternative. Amiodarone has limited efficacy for acute AFL termination.
Anticoagulation per AFib guidelines: The thromboembolic risk of AFL is equivalent to AF. The same anticoagulation strategy applies:
- AFL duration >48 hours (or unknown): anticoagulate for ≥3 weeks before elective cardioversion, then ≥4 weeks post-cardioversion regardless of CHA₂DS₂-VASc score
- OR TEE to exclude left atrial appendage thrombus before cardioversion
- Long-term anticoagulation guided by CHA₂DS₂-VASc score, identical to AF management
- DOACs preferred over warfarin in non-valvular AFL; same dosing regimens as AF
9. Catheter Ablation (CTI Ablation)
CTI ablation is the preferred long-term therapy for typical AFL, with success rates exceeding 95% and very low recurrence rates (~5–10%):
- A line of radiofrequency (RF) lesions is deployed from the tricuspid annulus to the inferior vena cava, creating bidirectional conduction block across the CTI
- CTI block is confirmed by demonstrating "differential pacing" — pacing from coronary sinus ostium and observing the activation sequence change from counterclockwise to clockwise (or vice versa)
- Procedure duration: typically 1–2 hours; performed under conscious sedation
- Success: >95% acute termination and long-term freedom from typical AFL
- Complications: rare — AV block (<1%), right coronary artery injury (<0.1%), pericardial effusion (<1%)
- After CTI ablation: ~50% of patients develop AFib within 5 years, as the underlying atrial substrate persists; these patients may require rhythm control therapy for AF
10. Thromboembolic Risk and Prevention
AFL carries thromboembolic risk equivalent to AF despite the organized atrial activity. Pathophysiologic explanation: although atrial contractile function appears to be maintained in AFL, atrial mechanical dysfunction can persist (atrial "stunning") after cardioversion, and left atrial appendage (LAA) flow is frequently impaired during AFL.
Embolic risk from AFL is substantial:
- AFL patients not anticoagulated have similar stroke rates to AF patients
- TEE studies demonstrate LAA thrombus in 0–5% of AFL patients cardioverted after <48 hours, comparable to AF
- Long-term anticoagulation recommendations identical to AF — CHA₂DS₂-VASc score guides therapy
- DOACs equally appropriate in AFL as in AF
Anticoagulation should be initiated and maintained even after successful CTI ablation if the patient's CHA₂DS₂-VASc score warrants it, due to high AF conversion risk.
Research Papers
The following PubMed topic searches return current peer-reviewed literature relevant to this condition. Each link opens a live PubMed query.
- Atrial flutter epidemiology incidence
- Cavotricuspid isthmus atrial flutter mechanism
- CTI ablation atrial flutter outcomes
- Atrial flutter anticoagulation thromboembolic risk
- Atrial flutter atrial fibrillation continuum
- Typical atrial flutter ECG diagnosis
- Ibutilide atrial flutter cardioversion
- Atrial flutter DC cardioversion
- Atrial flutter stroke risk
- Left atrial appendage thrombus flutter
- Atrial flutter radiofrequency ablation
- Post-ablation atrial flutter AF recurrence
Connections
- Cardiology
- Arrhythmia
- Atrial Fibrillation
- Supraventricular Tachycardia
- Heart Block
- Stroke
- Heart Failure
- Hypertension
- Heart Palpitations
- Lightheadedness
- Magnesium
- Deep Vein Thrombosis
- Long QT Syndrome
- Cryosurgery and Cryoablation (cardiac cryoablation)