Cryosurgery and Cryoablation: Freezing as a Medical Treatment
When most people hear "cryotherapy" they picture a wellness spa and an icy plunge tub. But the oldest and by far the most medically established use of extreme cold is not about recovery or mood — it is about deliberately destroying unwanted tissue. Doctors freeze warts off skin, freeze pre-cancerous spots before they turn into cancer, freeze tumors deep inside a kidney or prostate, and freeze tiny misfiring patches of heart muscle to stop a dangerous rhythm. This is therapeutic tissue destruction by controlled freezing, and it is genuinely well-established medicine with decades of use behind it. This page explains how freezing kills tissue, walks through what actually happens in the dermatology clinic and the operating room, and sets honest expectations — including where freezing is an excellent choice and where surgery or other methods are still better.
Table of Contents
- Cryosurgery vs. Cryoablation: The Words
- How Freezing Kills Tissue
- Liquid Nitrogen in the Skin Clinic
- The Freeze, the Blister & Healing
- Cryoablation for Tumors
- Cardiac Cryoablation for Arrhythmias
- When Freezing Is Chosen Over Cutting
- Setting Honest Expectations
- A Myth Worth Correcting
- Key Research
- Connections
- Featured Videos
Cryosurgery vs. Cryoablation: The Words
The two terms describe the same basic idea — killing tissue with cold — but the setting differs, and it helps to keep them straight.
- Cryosurgery (also called cryotherapy in a dermatology context) usually means freezing something on or near the surface of the body, most often with liquid nitrogen sprayed or dabbed onto the skin. Freezing a wart or a rough sun spot is cryosurgery. It is typically quick, done in a clinic, and needs no anesthesia.
- Cryoablation usually means freezing a target inside the body through a thin needle-like probe, guided by imaging such as ultrasound, CT, or MRI. Freezing a small kidney tumor, or freezing a patch of heart tissue, is cryoablation. It is an image-guided or catheter-based procedure done by a radiologist, urologist, or cardiologist.
Both rely on the same physics. The difference is mostly how the cold is delivered and how deep the target sits. Everything on this page — the skin clinic, the tumor probe, the heart catheter — is the same freeze-kill mechanism aimed at different tissue. That mechanism is also exactly what happens accidentally in frostbite; you can watch the shared cold-injury cascade in the companion cold-response animation, where the "frostbite" scenario is simply this treatment turned on purpose.
How Freezing Kills Tissue
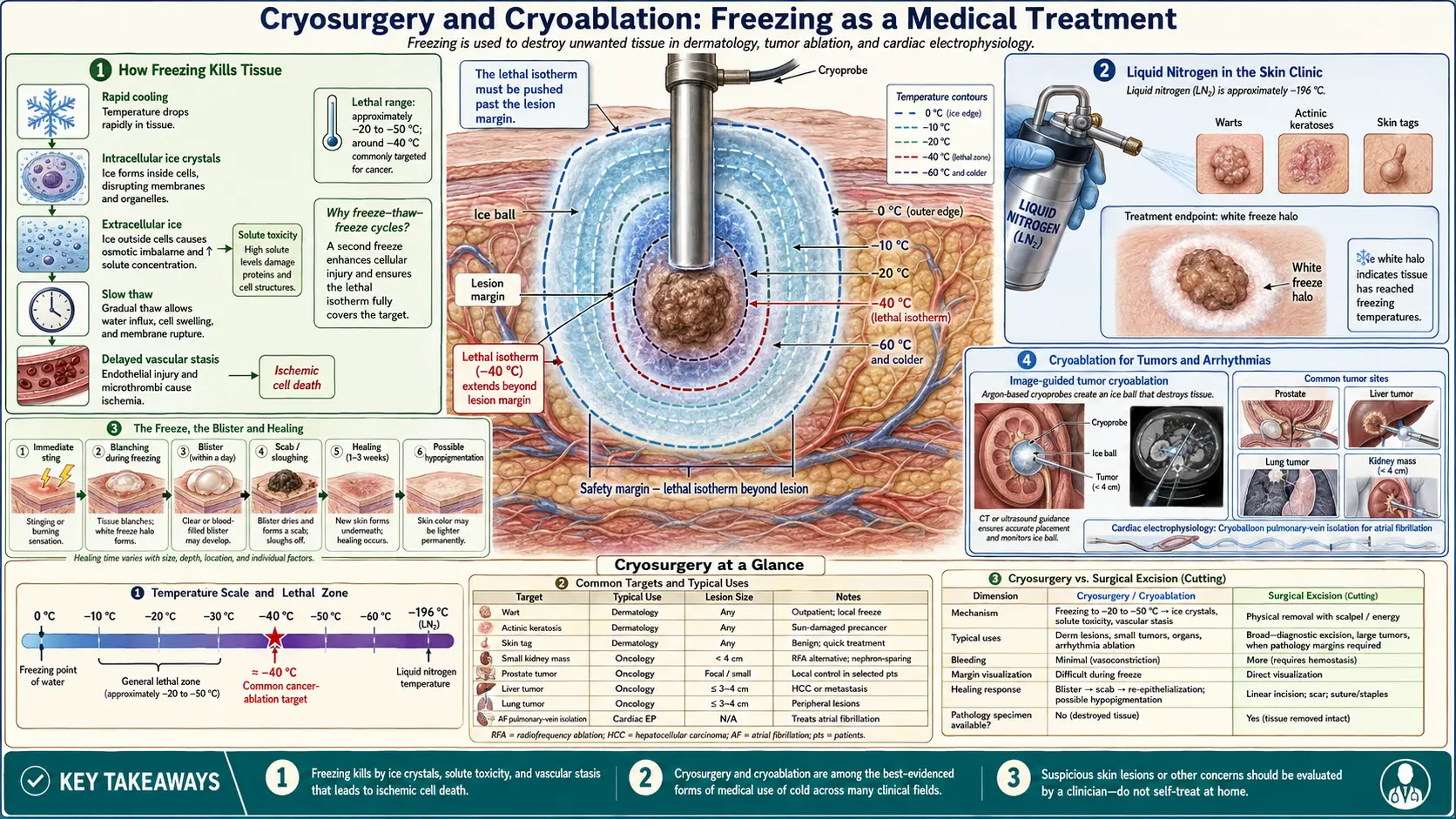
Cold does not kill cells by magic; it destroys them through a specific, well-understood sequence. Understanding it explains why doctors freeze, thaw, and then freeze again, and why a light chill is useless but a deep freeze is lethal.
Ice crystals rupture the cells
As tissue is cooled, water freezes — first in the fluid outside the cells, then, if cooling is fast and deep enough, inside them. Ice crystals forming inside a cell physically tear apart its internal machinery and puncture its membranes. The freezing also pulls water out of cells and concentrates the salts left behind, which is chemically toxic on its own. Fast cooling makes more of the deadly intracellular ice, which is why probes and sprays chill hard and quickly rather than gently.
The slow thaw does more damage
Counterintuitively, the thawing phase is where a lot of the killing happens. A slow, passive thaw lets small ice crystals fuse into larger, more destructive ones and prolongs the toxic, salt-concentrated state inside the cell. This is the reasoning behind the standard freeze–thaw–freeze cycle: the second freeze hits tissue already weakened by the first, and each slow thaw grinds it down further. Two cycles reliably kill more tissue than one.
Vascular stasis finishes the job
The final blow comes hours later. Freezing injures the lining of the small blood vessels feeding the treated area. As the tissue thaws, those vessels leak, clot, and shut down — a process called vascular stasis. The result is that even cells that survived the ice itself are cut off from their blood supply and die over the following hours to days. This delayed vascular death is why a frozen spot keeps declaring itself long after the probe is gone.
How cold is cold enough
Not every temperature that feels freezing actually kills. Reliable cell death generally requires cooling tissue to roughly −20 to −50 °C, and for cancer the target is usually the colder end, around −40 °C or below, to be confident malignant cells are destroyed. The freezing agents easily reach these depths and then some: liquid nitrogen boils at about −196 °C (−320 °F), and modern gas-driven cryoprobes reach comparably brutal temperatures. The catch is that the killing zone shrinks as you move outward from the probe or spray — the surface may be far colder than lethal while the edge of the visible ice is barely at freezing (0 °C) and not cold enough to kill. Doctors therefore aim to push the lethal isotherm past the edge of the lesion, deliberately freezing a margin of healthy-looking tissue.
Liquid Nitrogen in the Skin Clinic
The version of this you are most likely to meet is the dermatologist's or family doctor's liquid-nitrogen treatment. A small flask of liquid nitrogen feeds either a spray gun (a fine, cold jet aimed at the lesion) or a cotton-tipped applicator dipped in nitrogen and pressed onto it. There is a brief, sharp burning or stinging sensation for a few seconds, sometimes described as feeling like a hot pinch rather than a cold one. Most lesions need no numbing.
Common targets and rough approaches:
- Warts — caused by human papillomavirus (HPV), these are frozen with one or two freeze–thaw cycles, often needing repeat visits every 2–3 weeks until they clear. Thick warts on the hands or feet are stubborn and may take several sessions. See Warts for the fuller treatment picture.
- Actinic keratoses — rough, scaly sun-damage spots that are considered pre-cancerous because a fraction can progress to squamous cell skin cancer. Freezing them is a mainstay of preventing that progression. A brief single freeze often suffices per spot. See Actinic Keratosis.
- Molluscum contagiosum — small, dome-shaped viral bumps, common in children, that can be touched off with a quick freeze.
- Skin tags — harmless soft flaps, easily frozen at the base, though snipping or cautery is often quicker for these. See Skin Tags.
- Selected superficial skin cancers — certain thin, low-risk basal cell or squamous cell cancers, and the very early in-place form, can be treated with cryosurgery by an experienced clinician, though surgery is preferred for anything higher-risk (see When Freezing Is Chosen and Skin Cancer).
The freeze time varies with the target — a delicate wart on a child versus a thick plantar wart are very different — but the clinician is watching for a specific sign: a white "ice ball" or freeze halo that spreads a millimeter or two beyond the lesion, then times the hold from there. That visible margin is the practical stand-in for "the lethal cold reached the whole target."
The Freeze, the Blister & Healing
Knowing what the days afterward look like prevents a lot of needless worry, because a well-treated spot is supposed to look worse before it looks better.
- Immediately: the spot stings, turns white during the freeze, then reddens and may swell as it thaws.
- Within hours to a day: a blister often forms — sometimes clear, sometimes blood-filled (a dark or purple blister), which looks alarming but is a normal, expected result of the tissue separating as it dies. This is the treatment working, not a complication.
- Over the next 1–2 weeks: the blister dries, a scab forms, and the dead tissue sloughs off, leaving fresh skin underneath. Most simple lesions heal in roughly one to three weeks depending on size and location; areas like the lower legs heal more slowly.
Aftercare is simple: keep it clean, do not deliberately pop a blister (if it bursts on its own, keep it clean and covered), and let the scab fall off naturally. Honest side effects to expect: a possible pale (hypopigmented) mark where the freeze destroyed pigment cells, which can be permanent and is more noticeable on darker skin; occasionally a small scar; temporary numbness or tingling if a nerve near the skin was chilled; and rarely, infection. Because pigment cells are especially sensitive to cold, cryosurgery is used cautiously on the faces of people with darker skin tones.
Cryoablation for Tumors
The same freeze-kill mechanism is aimed at tumors deep inside the body using a thin, insulated cryoprobe — a needle only a few millimeters wide — passed through the skin and steered to the target under CT, ultrasound, or MRI guidance. Modern probes work by rapidly expanding pressurized gas (typically argon to freeze, helium to thaw) at the probe tip. As the tip plunges to lethal temperatures, a roughly egg-shaped "ice ball" grows outward around it, visible in real time on the scan. The doctor watches the advancing ice edge and keeps freezing until the ice ball engulfs the tumor plus a safe margin, usually running two freeze–thaw cycles for the reasons described above. Larger tumors are covered by placing several probes at once to merge their ice balls.
Cryoablation is an established or emerging option for several tumors:
- Kidney tumors — small renal masses (generally under about 4 cm) are among the best-established targets, especially for older patients or those who are poor candidates for surgery, or who have only one working kidney and cannot afford to lose tissue. It spares far more of the kidney than removing it.
- Prostate — cryoablation of the prostate is an accepted treatment for selected localized prostate cancer, and increasingly for focal therapy that freezes only the cancerous zone rather than the whole gland, aiming to preserve urinary and sexual function.
- Liver and lung tumors — freezing is used for certain primary or secondary (metastatic) tumors in patients who are not surgical candidates, as one of several "ablation" options.
- Breast fibroadenomas — benign breast lumps can be frozen in an office setting as an alternative to surgical removal, letting the body reabsorb the treated tissue over months.
- Painful bone metastases — when cancer has spread to bone and is causing severe pain, cryoablation of the lesion is a valued palliative tool that can meaningfully reduce pain even when cure is not the goal.
An interesting practical advantage of freezing over heat-based ablation is that the ice ball is clearly visible on imaging, so the doctor can literally see how much tissue is being treated. Freezing also tends to be less immediately painful than heat, which can allow lighter sedation for some procedures.
Cardiac Cryoablation for Arrhythmias
One of the most elegant uses of medical freezing is inside the heart. Many abnormal heart rhythms (arrhythmias) are caused by tiny patches of heart muscle or extra electrical pathways that fire or conduct when they should not. Ablation treats these by scarring the culprit tissue so it can no longer carry the rogue signal. This can be done with heat (radiofrequency ablation) or with cold (cryoablation), both delivered through a catheter threaded up a vein into the heart — no chest incision.
Cardiac cryoablation shines in a few situations:
- Atrial fibrillation (AFib) — a specialized cryoballoon is inflated where the pulmonary veins meet the left atrium and frozen to isolate the veins that trigger the chaotic rhythm. Balloon cryoablation is now a standard, well-studied approach for AFib. See Atrial Fibrillation.
- AVNRT and atrial flutter — for fast rhythms arising near the heart's critical wiring (the AV node), cryoablation is often preferred precisely because freezing is gentler on nearby delicate structures. See Atrial Flutter.
Two features make cold especially attractive near fragile parts of the heart's conduction system. First is cryo-mapping: the tip can be cooled to a mild, reversible temperature (around −30 °C) that temporarily stuns the tissue without destroying it. If freezing the spot briefly stops the arrhythmia and does not harm normal conduction, the doctor commits to a colder, permanent lesion; if it accidentally disturbs the AV node, they simply stop and the tissue recovers. Radiofrequency heat offers no such "test drive" — damage is immediate and permanent. Second, cryoablation tends to keep the treated tissue's structure more intact and carries a lower risk of certain complications like blood-clot formation on the catheter and injury to adjacent structures. The trade-off is that cryo lesions can sometimes be less durable than heat, so the choice between cold and heat depends on the specific arrhythmia and the electrophysiologist's judgment.
When Freezing Is Chosen Over Cutting
Freezing is not automatically better than surgery — it is a tool with a niche. It tends to be favored when:
- The patient is a poor surgical candidate — older, frail, or with other illnesses that make anesthesia and a big operation risky. A probe through the skin is far less taxing than open surgery.
- Preserving surrounding tissue matters — sparing kidney tissue, or freezing only part of a prostate to protect nearby nerves.
- The lesion is small, accessible, and well-defined — freezing works best when the target is modest in size and the ice ball can reliably cover it with a margin.
- Delicacy near vital structures is needed — as with the reversible "test" freeze in the heart.
- The goal is comfort, not cure — palliating painful bone metastases.
Surgery (or heat ablation, or other therapy) is usually still preferred for larger tumors, higher-risk or deeply invasive cancers, and lesions where a pathologist needs to examine removed tissue to confirm clean edges — something freezing, which destroys tissue in place, cannot provide.
Setting Honest Expectations
Here is where an evidence-honest site has to be careful, because "cryotherapy" covers wildly different levels of proof:
- Well-established (strong evidence): dermatologic cryosurgery for warts, actinic keratoses, molluscum, and skin tags is decades-proven and routine. Cardiac cryoballoon ablation for atrial fibrillation and cryoablation for AVNRT are supported by solid trials and guidelines. Renal cryoablation for small kidney tumors is a well-accepted option in the right patients. These are real medicine, not wellness claims.
- Established but with caveats: prostate, liver, lung, and bone cryoablation are legitimate, in-use options whose exact place versus surgery, radiation, or other ablation is still being refined by ongoing research and depends heavily on the individual case.
- The catch across all of it — recurrence: freezing does not guarantee a one-and-done cure. Warts frequently need multiple sessions and can still come back. A frozen tumor can leave microscopic survivors at the margin and recur, which is why cryoablation patients get follow-up imaging and some need repeat treatment. Honest framing: freezing is often highly effective, but "effective" is not the same as "permanent in every case."
None of this is the same thing as the whole-body cryotherapy chambers marketed for recovery and wellness, whose evidence is far weaker. Destroying a defined lesion with a targeted, monitored, lethal freeze is a completely different proposition from standing in a cold-mist booth for three minutes.
A Myth Worth Correcting
Myth: "Freezing a wart kills the virus." It does not, at least not directly. Cryosurgery destroys the infected skin cells where the wart is growing; it does not seek out and neutralize human papillomavirus scattered in the surrounding skin. That is precisely why warts are so prone to returning after treatment and often need several rounds — freeze the visible wart, and the virus lurking in nearby skin can seed a new one. The freeze works by removing the affected tissue and, some researchers think, by provoking a local immune response that may help clear the virus, but the notion that a single zap sterilizes the area is wrong. Set expectations accordingly: cryosurgery for warts is effective but often a course of treatment, not a single cure.
A related over-reach worth flagging: cryosurgery is not an all-purpose skin-cancer cure. It has a real but limited role for select thin, low-risk lesions in experienced hands. For most skin cancers — anything thick, aggressive, poorly defined, in a high-risk location, or where confirming clean margins matters — surgical removal remains the standard. Freezing a suspicious spot without a proper diagnosis can also mask a cancer while leaving it behind. Anything unusual, changing, or bleeding on the skin deserves evaluation and often a biopsy first, not a do-it-yourself freeze.
Key Research
Because this is a fast-moving clinical field, the safest way to reach the current evidence is a live PubMed topic search rather than a single frozen citation. These searches open the peer-reviewed literature on each use discussed above.
- PubMed: mechanisms of cryosurgical tissue injury (ice crystals, freeze–thaw, vascular stasis)
- PubMed: cryotherapy for cutaneous warts — clinical trials
- PubMed: cryosurgery for actinic keratosis
- PubMed: renal cryoablation for small renal masses — outcomes
- PubMed: cryoballoon ablation for atrial fibrillation
- PubMed: cryoablation vs. radiofrequency for AVNRT and AV-nodal arrhythmias
- PubMed: cryoablation for painful bone metastases (palliation)
Connections
- All Remedies
- Cryotherapy Hub
- Cryotherapy for Pain & Inflammation
- Safety, Risks & Contraindications
- Warts
- Actinic Keratosis
- Skin Tags
- Skin Cancer
- Atrial Fibrillation
- Arrhythmia