Staphylococcus Aureus Treatment and Prevention
MRSA Treatment
Vancomycin, daptomycin, linezolid, and newer agents for resistant staph infections.
Decolonization & Control
Mupirocin nasal decolonization, chlorhexidine baths, and hospital infection control.
MRSA Drug Resistance
The mecA gene, beta-lactam resistance mechanisms, and the VRSA threat.
Table of Contents
- MSSA vs MRSA: Why Susceptibility Results Change Everything
- Oral vs IV Treatment: When Each Is Appropriate
- Incision and Drainage for Abscesses
- Antibiotic Duration by Infection Site
- Source Control: The Often-Overlooked Step
- Preventing Surgical Site Infections
- MRSA Decolonization: Who Needs It and How
- Hand Hygiene and Contact Precautions
- Key Research Papers
- Connections
- Featured Videos
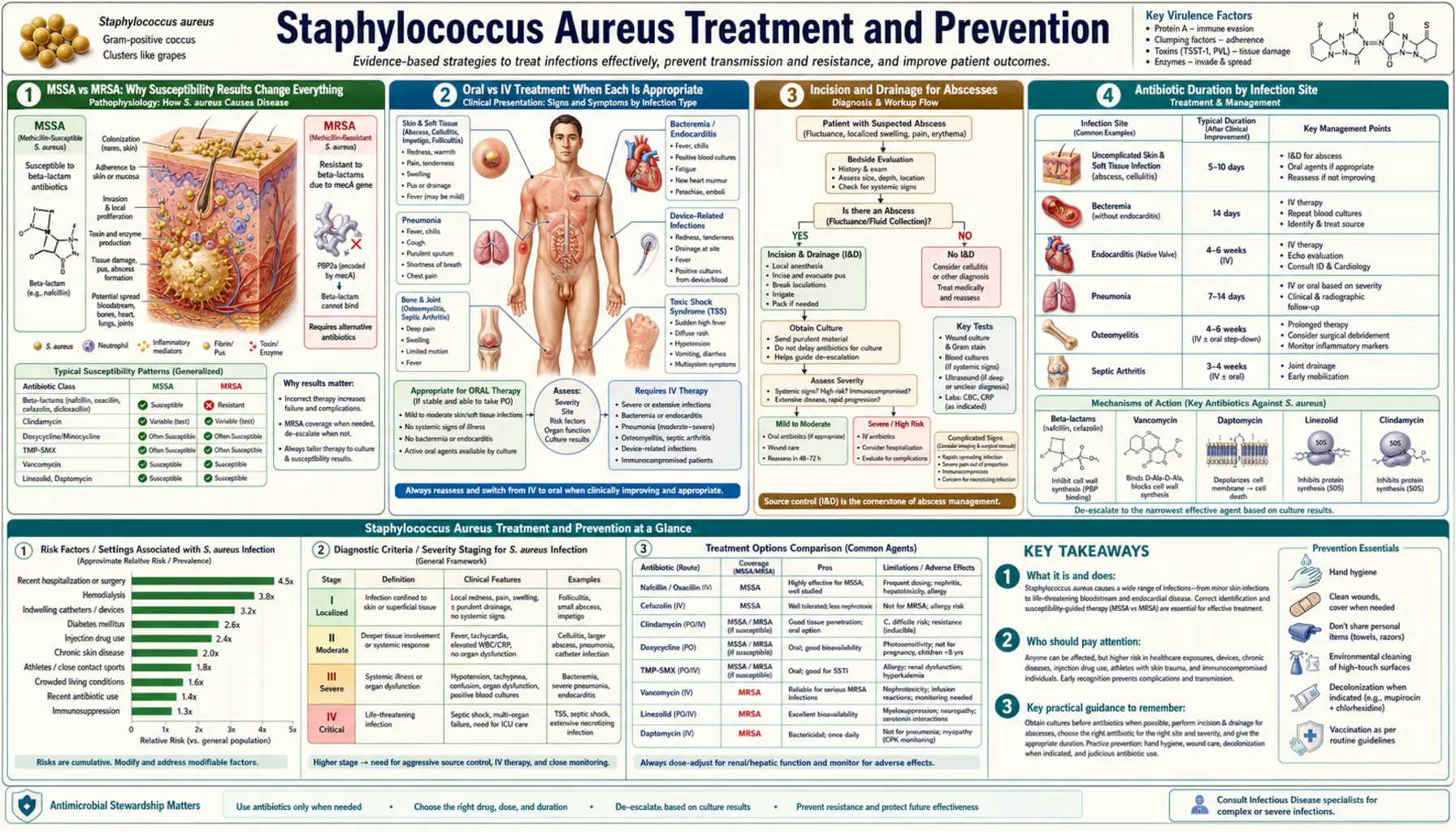
MSSA vs MRSA: Why Susceptibility Results Change Everything
When your doctor says you have a staph infection, the single most important piece of information they are waiting for is the susceptibility result from the lab. That result — usually available 48 to 72 hours after a culture is taken — tells you whether the bacteria is methicillin-susceptible Staphylococcus aureus (MSSA) or methicillin-resistant Staphylococcus aureus (MRSA). The difference determines not just which antibiotic you get, but how well you will do.
For MSSA, the best antibiotics are beta-lactams — specifically anti-staphylococcal penicillins like nafcillin and oxacillin (given intravenously for serious infections), or cephalosporins like cefazolin. These drugs are highly effective, work quickly, and have fewer side effects than the alternatives. For skin infections, oral agents like dicloxacillin or cephalexin work well.
For MRSA, beta-lactams do not work — the mecA gene encodes a modified cell-wall building protein (PBP2a) that beta-lactams cannot bind. The standard IV treatment for serious MRSA infections is vancomycin. Alternatives include daptomycin, linezolid, ceftaroline (a newer cephalosporin that does reach PBP2a), and telavancin.
A critical point that matters for outcomes: you should not use vancomycin to treat MSSA, even though it technically works. Studies consistently show that vancomycin is inferior to anti-staphylococcal penicillins for MSSA bacteremia — it leads to higher rates of treatment failure and slower clearance of bacteria from the blood. If the culture comes back MSSA and you are already on vancomycin empirically, your team should switch you to nafcillin, oxacillin, or cefazolin as soon as possible. This is called "antibiotic de-escalation" and it genuinely saves lives.
For community-acquired MRSA skin and soft tissue infections (the kind you can pick up from gyms, schools, and households), oral antibiotics that usually work include trimethoprim-sulfamethoxazole (TMP-SMX, sold as Bactrim) and doxycycline. Clindamycin also works in areas where inducible resistance rates are low. Your doctor should check local susceptibility data before prescribing clindamycin.
Oral vs IV Treatment: When Each Is Appropriate
One of the most common questions patients have is whether they need to stay in the hospital for IV antibiotics or whether pills at home will be enough. The short answer: it depends entirely on where the infection is and how serious it is.
Infections where oral antibiotics are usually sufficient:
- Small uncomplicated skin abscesses after incision and drainage (see next section)
- Minor skin and soft tissue infections (cellulitis, small impetigo patches) without fever or signs of spreading
- MRSA nasal colonization during decolonization protocols
Infections that require IV antibiotics:
- Bacteremia (staph in the bloodstream) — always IV, no exceptions
- Infective endocarditis (infection of heart valves) — IV for 4 to 6 weeks
- Osteomyelitis (bone infection) — IV for at least the initial phase, sometimes transitioned to oral after weeks
- Septic arthritis (infected joints) — IV initially, sometimes oral step-down
- Pneumonia caused by MRSA — IV initially
- Deep tissue infections, fasciitis, or any infection with signs of systemic illness (high fever, low blood pressure, confusion)
For patients who need long courses of IV antibiotics but are otherwise stable, outpatient parenteral antibiotic therapy (OPAT) is an option. You receive daily or twice-daily IV infusions through a peripherally inserted central catheter (PICC line) at home or at an infusion clinic, avoiding a prolonged hospital stay.
There is growing evidence that in carefully selected patients with uncomplicated MRSA bacteremia, transitioning to oral antibiotics after an initial IV course is feasible. The NEJM 2019 POET trial and smaller staph studies have explored this, though standard of care in the United States still strongly favors completing bacteremia treatment with IV agents. Ask your infectious disease specialist about what is appropriate in your case.
Incision and Drainage for Abscesses
If you have a staph skin abscess — a painful, swollen, pus-filled lump — the single most important treatment step is draining it. This is called incision and drainage (I&D), and in many cases it is the treatment, not just a preliminary step.
The procedure is straightforward: a doctor numbs the skin with local anesthetic, makes a small cut into the abscess, and allows the pus to drain. The cavity is irrigated with saline and sometimes loosely packed with gauze to keep it open for a day or two so it can continue draining. The whole procedure takes about 10 to 20 minutes in an urgent care or emergency setting.
A well-drained abscess often heals without antibiotics, even when caused by MRSA. The 2017 NEJM trial by Talan et al. showed that adding TMP-SMX to I&D for skin abscesses improved cure rates compared to I&D alone, but the cure rate with I&D alone was still around 70%. Current IDSA guidelines recommend adding a 5-day course of TMP-SMX or clindamycin to I&D for most CA-MRSA abscesses because of that improvement in outcomes — but drainage remains the cornerstone.
What you should not do is try to pop or squeeze an abscess at home. Squeezing can push bacteria deeper into surrounding tissue or into the bloodstream. If you see a swollen, red, warm lump that feels like it has fluid in it, go to a clinic or urgent care for proper drainage.
After drainage, watch for signs that the infection is not resolving: increasing redness spreading outward from the wound edge (not just around the incision), fever, red streaks moving up a limb (tracking toward lymph nodes), or feeling generally unwell. These signs mean the infection is spreading beyond the abscess and you need IV antibiotics.
Antibiotic Duration by Infection Site
One of the things that makes staph infections different from many other bacterial infections is that treatment duration is highly variable — and getting the duration right matters. Too short and the infection comes back or seeds distant sites; too long exposes you to drug side effects and resistance risks unnecessarily.
Here are the standard treatment durations by infection type, based on Infectious Diseases Society of America (IDSA) guidelines and published evidence:
- Uncomplicated skin and soft tissue infection (SSTI) after I&D: 5 to 7 days of oral antibiotics. Some guidelines say 5 days is sufficient for most skin abscesses.
- Cellulitis without abscess: 5 to 7 days, extended to 14 days if not improving.
- Uncomplicated bacteremia (staph in blood, source cleared, no evidence of seeding): minimum 14 days of IV antibiotics from the first negative blood culture. "Uncomplicated" means: no implanted hardware, no endocarditis, no persistent positive cultures after 4 days, no fever after 72 hours of treatment.
- Complicated bacteremia: at least 4 to 6 weeks, depending on what is infected.
- Infective endocarditis (native valve): 4 to 6 weeks IV. Right-sided endocarditis in some patients can be treated with 2 weeks of nafcillin or oxacillin if criteria are met.
- Prosthetic valve endocarditis: at least 6 weeks IV. Rifampin is added for its ability to penetrate biofilm on prosthetic material.
- Osteomyelitis (bone infection): typically 6 weeks, sometimes longer. Some cases can transition to oral antibiotics after 1 to 2 weeks of IV therapy.
- Septic arthritis (native joint): 3 to 4 weeks IV, combined with joint drainage.
A note on blood cultures: if you have bacteremia, your doctor will repeat blood cultures every 48 to 72 hours until they are negative. Treatment duration is counted from the day the first negative culture is drawn — not from the day antibiotics started. This is important because the clock resets if cultures remain positive, indicating the infection is not clearing.
Source Control: The Often-Overlooked Step
Source control means physically removing or draining the thing causing the infection. Antibiotics kill bacteria floating in your bloodstream or tissue, but they cannot sterilize a collection of pus, a biofilm on a foreign device, or a necrotic tissue pocket. No antibiotic concentration in tissue is high enough to overcome an undrained abscess or an infected implant.
The most common source control issues in staph infections:
- IV catheters and central lines: If a patient develops bacteremia and has a central venous catheter (CVC), PICC line, or dialysis catheter, that device must be removed unless there is a compelling reason to keep it. Leaving an infected catheter in place is the most common reason staph bacteremia fails to clear. Remove the line, then place a new one at a different site once cultures are negative.
- Abscesses and fluid collections: These must be drained — surgically, by interventional radiology with image-guided drains, or at the bedside for superficial abscesses. Internal abscesses (liver, spleen, psoas muscle, epidural space) often require CT-guided drainage.
- Infected joint prostheses and orthopedic hardware: This is one of the most difficult situations. Biofilm on metal is nearly impossible to eradicate with antibiotics alone. Options include: (1) two-stage exchange (remove the prosthesis, treat with IV antibiotics for 6 weeks, implant a new prosthesis), (2) DAIR (debridement, antibiotics, implant retention) for early infections with stable hardware, or (3) long-term oral suppressive antibiotics when surgery is not possible.
- Infected pacemakers, defibrillators, and valve replacements: These almost always require hardware removal for cure. Suppression without removal fails in the vast majority of cases.
- Empyema (infected fluid around the lung): Requires chest tube drainage.
If you are admitted with staph bacteremia and your cultures are not clearing, the first question your infectious disease doctor should ask is: "Is there an undrainable or unremoved source?"
Preventing Surgical Site Infections
Staphylococcus aureus is the most common cause of surgical site infections (SSIs), responsible for roughly 20 to 30% of all SSIs. The consequences are serious — SSIs prolong hospital stays, can seed the bloodstream, and require re-operation in severe cases. Prevention is both well-studied and highly effective.
Preoperative MRSA screening: Before elective surgery, many hospitals now routinely screen patients for MRSA nasal carriage by swabbing the nose. Patients who test positive undergo decolonization — typically 5 days of mupirocin nasal ointment twice daily plus daily chlorhexidine baths before surgery. Multiple randomized trials have shown this reduces SSI rates substantially, particularly for cardiac, orthopedic, and abdominal surgeries.
Perioperative antibiotic prophylaxis: The standard prophylactic antibiotic for most surgeries in MSSA-colonized or unscreened patients is cefazolin (a first-generation cephalosporin), given within 60 minutes before the first incision and repeated if surgery extends beyond 4 hours. For patients known to carry MRSA, vancomycin should be given instead of or in addition to cefazolin. For patients with a documented beta-lactam allergy, vancomycin or clindamycin are alternatives.
Intraoperative technique matters: Maintaining normothermia (normal body temperature) during surgery, avoiding unnecessary tissue trauma, and using good sterile technique all reduce SSI rates. Hyperglycemia during and after surgery impairs immune function — tight glucose control in the perioperative period reduces infections, particularly in diabetic patients.
Postoperative wound care: Keep the surgical wound covered with a sterile dressing for at least 48 hours. After that, clean, dry wounds can be left open to air. Showering is generally safe after 48 to 72 hours if the wound is closed. Report increasing redness, warmth, swelling, drainage of pus, or fever to your surgeon promptly.
MRSA Decolonization: Who Needs It and How
MRSA decolonization means using antibiotics and antiseptics to reduce or eliminate MRSA from the body surfaces where it likes to live — primarily the nasal passages, but also the skin, groin, and axilla. "Decolonization" does not mean "curing an infection." It means treating the silent carriage state so you are less likely to infect yourself or spread MRSA to others.
Who benefits from decolonization:
- Patients scheduled for high-risk elective surgery (cardiac, orthopedic, abdominal) who screen positive for nasal MRSA carriage
- Patients with recurrent MRSA skin and soft tissue infections (3 or more episodes in 12 months)
- Hemodialysis patients, who have very high rates of MRSA colonization and infection
- Close household contacts of patients with active MRSA infections, when household transmission is suspected as the source of recurrent infections
- ICU patients in some hospitals as part of universal decolonization programs (see the REDUCE MRSA trial)
The standard decolonization protocol:
- Mupirocin nasal ointment: Applied to both nostrils twice daily for 5 days. The nose is the primary reservoir — about 30% of people carry S. aureus nasally at any time.
- Chlorhexidine skin washes: Daily full-body washes with 4% chlorhexidine gluconate solution for 5 days. Pay particular attention to skin folds, the groin, and the axillae. Use a chlorhexidine-soaked cloth or wash with the solution like soap, leaving it on the skin for at least 1 minute before rinsing.
- Duration: The standard decolonization course is 5 days. For recurrent SSTI, some protocols repeat monthly for several months.
- Environmental decolonization: Simultaneously wash all clothing, bed linens, and towels in hot water. Do not share personal items (towels, razors, soap bars). Clean frequently touched surfaces in the home with a dilute bleach solution.
Mupirocin resistance is a real concern — resistance rates are rising in some areas. If decolonization fails, a provider may culture for mupirocin-resistant strains and substitute povidone-iodine nasal rinses or other agents.
Hand Hygiene and Contact Precautions
Hand hygiene is the single most effective intervention for preventing the spread of MRSA in hospitals and in households. MRSA spreads primarily through direct contact — touching a contaminated surface or person and then touching a mucous membrane or an open wound. It can survive on dry surfaces for days to weeks.
Soap and water vs alcohol gel: Alcohol-based hand sanitizers (ABHS) are effective against S. aureus and are the preferred agent in most healthcare situations because they are faster and less damaging to skin with repeated use. However, if hands are visibly soiled — with blood, pus, or wound drainage — you must wash with soap and water first. Both are effective against MRSA; the key is doing it correctly and frequently.
How to actually do it properly: For alcohol gel — apply enough to cover all surfaces, rub vigorously for at least 20 seconds until dry. For soap and water — wet hands, apply soap, scrub all surfaces for 20 seconds minimum, rinse thoroughly, dry with a clean towel. The back of the hands, between fingers, and under nails are consistently undertreated areas.
Contact precautions in hospitals: Hospitalized patients known to carry or be infected with MRSA are placed on contact precautions. This means:
- A private room, or cohorting with other MRSA-positive patients
- All healthcare workers entering the room must wear gloves and a gown
- Dedicated patient-care equipment (blood pressure cuff, stethoscope, thermometer) stays in the room and is cleaned or discarded when the patient is discharged
- The room is terminally cleaned with EPA-registered disinfectants effective against MRSA after discharge
Compliance is the real problem: Studies consistently show hand hygiene compliance rates in hospitals hover around 40% to 60%, even with active monitoring programs. The evidence is unambiguous that compliance above 80% substantially reduces MRSA transmission rates. As a patient or family member, you have the right to ask anyone entering your room whether they have cleaned their hands. Studies show that when patients ask, healthcare workers comply at higher rates.
At home: If you or a family member has active MRSA infection or is a known carrier, wash your hands before and after wound care, do not share towels or personal hygiene items, and cover all wound sites with clean bandages.
Key Research Papers
These peer-reviewed studies form the evidence base for current treatment and prevention guidelines:
- Liu C, et al. Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of Methicillin-Resistant Staphylococcus aureus Infections in Adults and Children. Clinical Infectious Diseases. 2011. PMID: 21208910
- Fowler VG, et al. Staphylococcus aureus Endocarditis: A Consequence of Medical Progress. JAMA. 2005. — Search PubMed
- Chambers HF, Deleo FR. Waves of Resistance: Staphylococcus aureus in the Antibiotic Era. Nature Reviews Microbiology. 2009. — Search PubMed
- Talan DA, et al. Trimethoprim-Sulfamethoxazole versus Placebo for Uncomplicated Skin Abscess. NEJM. 2016. — Search PubMed
- Robicsek A, et al. Universal surveillance for methicillin-resistant Staphylococcus aureus in 3 affiliated hospitals. Annals of Internal Medicine. 2008. — Search PubMed
- Bode LG, et al. Preventing Surgical-Site Infections in Nasal Carriers of Staphylococcus aureus. NEJM. 2010. — Search PubMed
- Klevens RM, et al. Invasive Methicillin-Resistant Staphylococcus aureus Infections in the United States. JAMA. 2007. — Search PubMed
- Huang SS, et al. Targeted versus Universal Decolonization to Prevent ICU Infection. NEJM. 2013. — Search PubMed
- Cosgrove SE, et al. Comparison of Mortality Associated with Methicillin-Resistant and Methicillin-Susceptible Staphylococcus aureus Bacteremia: A Meta-analysis. Clinical Infectious Diseases. 2003. — Search PubMed
- Moran GJ, et al. Methicillin-Resistant S. aureus Infections among Patients in the Emergency Department. NEJM. 2006. — Search PubMed
- van Hal SJ, et al. Predictors of Mortality in Staphylococcus aureus Bacteremia. Clinical Infectious Diseases. 2012. — Search PubMed
- Nathwani D, et al. Guidelines for UK practice for the diagnosis and management of methicillin-resistant Staphylococcus aureus (MRSA) infections presenting in the community. Journal of Antimicrobial Chemotherapy. 2008. — Search PubMed
Connections
- All Bacteria
- Staphylococcus Aureus
- Symptoms & Infections
- MRSA Treatment
- Decolonization & Infection Control
- Drug Resistance
- Garlic
- Oregano
- Tea Tree
- Manuka Honey
- Immune Boosting