MRSA Decolonization, Hand Hygiene, and Hospital Infection Control
MRSA doesn't just cause infections — it colonizes. Millions of people carry MRSA on their skin or in their nose without ever getting sick. The problem comes when that bacteria gets through a cut, a surgery, or a weakened immune system. Decolonization — deliberately clearing MRSA from the body before that happens — is one of the most effective tools we have for preventing serious infections. Combine it with rigorous hand hygiene and hospital infection control, and you can dramatically reduce the spread of one of the most dangerous bacteria in modern medicine.
Table of Contents
- Nasal Decolonization with Mupirocin
- Chlorhexidine Gluconate (CHG) Bathing
- Pre-Surgical Decolonization Protocols
- Contact Precautions in Hospitals
- Hand Hygiene: The Most Important Intervention
- Environmental Cleaning and Terminal Decontamination
- Community MRSA in Households
- Athlete and Sports Team Decolonization
- Key Research Papers
- Featured Videos
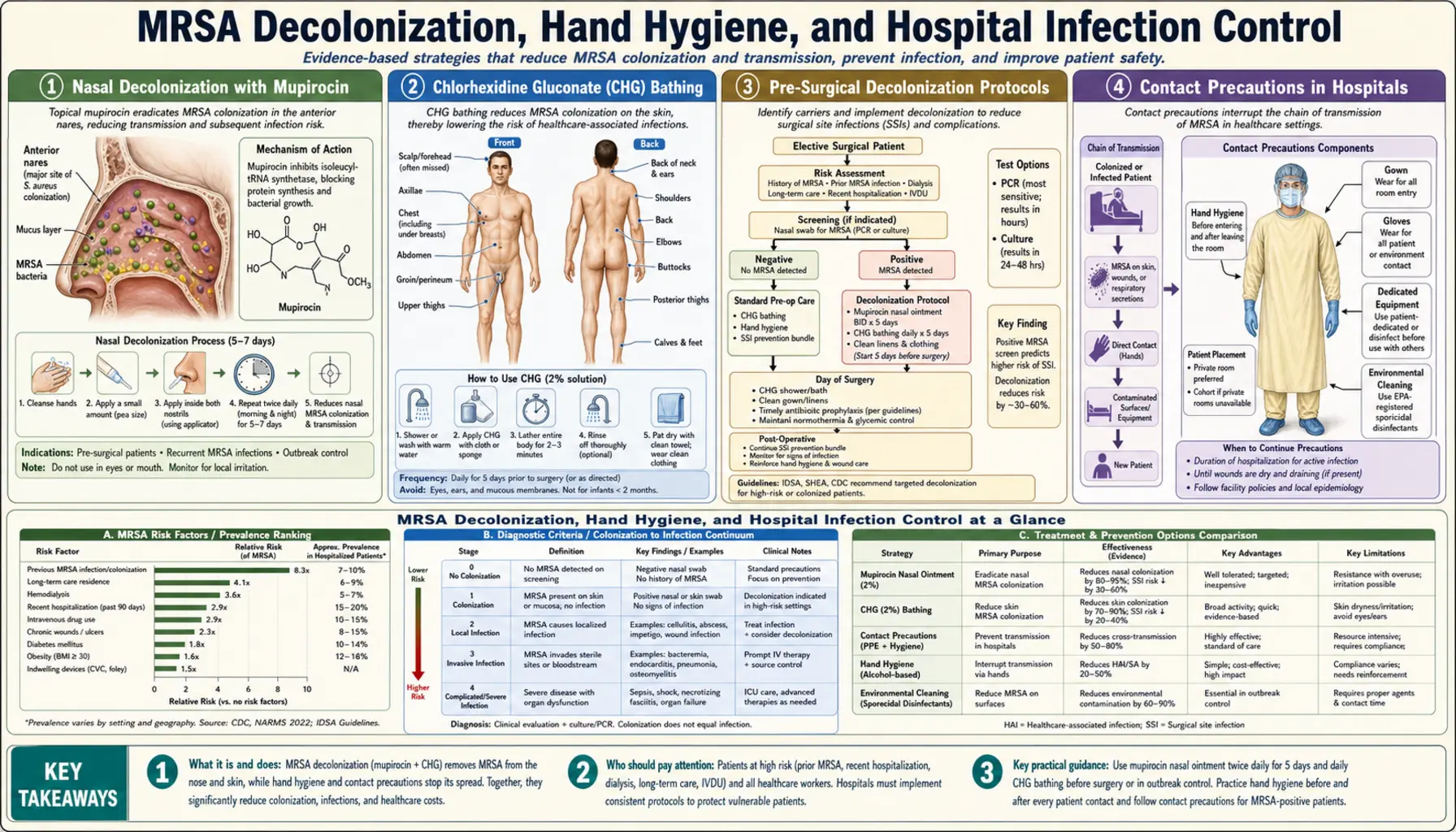
Nasal Decolonization with Mupirocin
The nose is MRSA's favorite hiding spot. About 30% of the general population carries S. aureus in their nasal passages at any given time, and roughly 1–3% carry the MRSA strain. These people are called asymptomatic carriers — they feel fine, but they can spread the bacteria to others and are at higher risk of infecting themselves if they undergo surgery or become immunocompromised.
Mupirocin 2% ointment is the go-to treatment for nasal decolonization. You apply a small amount (about the size of a match head) to the inside of both nostrils using a clean cotton swab or the tip of your finger, twice a day for 5 days. Pinch your nose closed and rub gently for about a minute to distribute the ointment. That's it — the medication works locally in the nasal lining where the bacteria live.
How well does it work? Studies show 70–80% of carriers test negative immediately after completing the 5-day course. The catch: relapse rates are significant. About 50% of people who were successfully decolonized become re-colonized within 12 weeks. This is why mupirocin is not used as a long-term preventive — the bacteria reacquire resistance quickly with repeated courses, and decolonization is most valuable as a targeted short-term strategy before a known high-risk event like surgery.
Who should be decolonized? Clear evidence supports treating:
- Patients who screen positive for MRSA before elective surgery (especially cardiac, orthopedic, or colorectal)
- Hemodialysis patients, who have dramatically elevated MRSA bacteremia risk due to repeated vascular access
- Patients with recurrent skin and soft tissue infections (three or more MRSA boils in a 12-month period)
- Close household contacts of a person with active MRSA infection, especially during an ongoing household outbreak
- Intensive care unit patients at high-risk facilities during outbreak management
Mupirocin resistance is a growing concern. When nasal cultures show mupirocin-resistant MRSA, alternatives include povidone-iodine 10% nasal swabs or delafloxacin nasal solution, though evidence for these alternatives is still maturing.
Chlorhexidine Gluconate (CHG) Bathing
While mupirocin targets the nose, chlorhexidine gluconate (CHG) tackles the skin. CHG is a broad-spectrum antiseptic that binds to skin proteins and keeps working for hours after application — it has what's called "residual activity," meaning it doesn't just wash off when you rinse.
Two forms are used clinically: 2% CHG-impregnated cloths and 4% CHG liquid wash. The cloths (brands like Sage or Medline) are pre-moistened wipes you use to wipe down the body from chin to toes, letting each area air-dry for about 30 seconds before moving on. You do not rinse. This is a key mistake many patients and nurses make — rinsing removes the drug before it can bind to the skin. The liquid wash is used like a regular shower but you apply it as a soap, lather for at least 2 minutes, and then rinse minimally or pat dry without wiping vigorously.
Daily CHG bathing for 5 to 14 days significantly reduces total bacterial load on the skin, including MRSA. The most robust evidence is in ICU settings. Daily CHG bathing is a core component of central line-associated bloodstream infection (CLABSI) prevention bundles, where it has been shown to reduce CLABSI rates by up to 40%.
Practical CHG rules:
- Avoid the face, eyes, ears, and mucous membranes — CHG is irritating to these tissues
- Do not use on open wounds or broken skin without clinician guidance
- Some people develop contact dermatitis — if significant skin irritation occurs, discontinue and notify your care team
- Patients with CHG allergy (rare but real) require alternative protocols
- Do not use CHG before chest X-ray or ECG electrode placement — it can interfere with electrode adhesion
In combination with mupirocin, CHG bathing forms what infection specialists call "targeted decolonization" — and together these two interventions are substantially more effective than either alone.
Pre-Surgical Decolonization Protocols
Surgery is when MRSA colonization becomes genuinely dangerous. The skin gets cut open, bacteria that normally sit harmlessly in the nose can travel along a catheter or drainage tube, and the stress of surgery temporarily suppresses the immune system. For MRSA carriers, the odds of a surgical site infection are measurably higher than for non-carriers.
The REDUCE MRSA trial and several subsequent studies established that universal pre-surgical decolonization — treating all patients, not just those who tested positive — cuts surgical site infections significantly. The protocol is straightforward: 5 days of mupirocin nasal ointment twice daily, combined with daily CHG bathing, starting before hospital admission and completing the course before the operation.
The numbers are striking. In MRSA-positive patients undergoing elective procedures, a 5-day mupirocin plus CHG protocol reduces surgical site infection rates by 50–80%. For cardiac surgery patients, this translates to preventing deep sternal wound infections — a complication that carries roughly 20–40% mortality and costs upward of $100,000 per case to treat.
Which surgeries benefit most?
- Cardiac surgery — sternotomy wounds are particularly susceptible; decolonization is standard of care at most major cardiac centers
- Orthopedic joint replacement — prosthetic joint infections are catastrophic; decolonization before total hip and knee replacement is strongly recommended
- Colorectal surgery — the gut environment plus an open wound creates high infection risk
- Neurosurgery — spinal hardware implants are vulnerable to MRSA seeding
- Vascular surgery — prosthetic grafts and bypasses are at risk
Some hospitals screen all surgical patients with nasal swabs and only decolonize MRSA-positive individuals (targeted decolonization). Others decolonize all patients regardless of screening results (universal decolonization). Both approaches reduce infections; universal decolonization eliminates the 2–5 day wait for culture results and is logistically simpler.
Contact Precautions in Hospitals
Once a hospital identifies that a patient carries or is infected with MRSA, the patient goes on "contact precautions." This is a bundle of practices designed to prevent MRSA from traveling from that patient's room to the rest of the hospital on the hands, clothes, or equipment of healthcare workers.
Contact precautions mean:
- Gown and gloves every time anyone enters the room — nurse, doctor, physical therapist, food service worker, visitor. No exceptions.
- Single room preferred. If a private room is not available, patients with MRSA are cohorted together (placed in a room with other MRSA patients) rather than sharing with MRSA-negative patients.
- Dedicated equipment stays in the room — stethoscope, blood pressure cuff, thermometer. Shared equipment that must enter the room is disinfected before leaving.
- Door stays closed when possible.
- Gloves and gown are removed inside the room before exiting, and hands are cleaned immediately upon leaving.
Contact precautions are one of the most consistently effective interventions for reducing hospital-acquired MRSA. Systematic reviews show hospitals that implement rigorous contact precaution programs experience 30–60% reductions in MRSA transmission rates.
When can contact precautions be discontinued? Guidelines vary, but most institutions require three consecutive negative MRSA screens (nasal swabs, wound cultures, or both) taken at least one week apart before discontinuing precautions. In some hospital systems, once-positive patients remain on precautions for the entire admission regardless of subsequent screens — a "once MRSA, always MRSA" policy during a hospitalization.
For patients, contact precautions can feel isolating — nurses visit less frequently, and some patients feel stigmatized. Studies confirm that patients on contact precautions receive fewer nursing assessments and have higher rates of adverse events unrelated to MRSA, possibly because the gowning barrier reduces casual check-ins. This is worth raising with your care team if you or a family member is on contact precautions for an extended stay.
Hand Hygiene: The Most Important Intervention
Of everything in the infection control toolkit, hand hygiene has the most evidence behind it and the most consistently poor compliance. Studies in hospitals consistently find that healthcare workers perform hand hygiene correctly only about 40% of the time. That gap — between what should happen and what does happen — is responsible for a substantial fraction of all healthcare-associated infections, including MRSA.
Two methods, different purposes:
- Soap and water for 20 seconds — works by mechanical removal, physically scrubbing bacteria off the skin surface. Required when hands are visibly soiled, after using the restroom, and after caring for a patient with Clostridioides difficile (alcohol does not kill C. diff spores). Twenty seconds means singing "Happy Birthday" twice in your head. Most people wash for 6–8 seconds and consider it done.
- Alcohol-based hand rub (ABHR) with 60–80% alcohol — kills bacteria on contact within 15–20 seconds of rubbing, without water. More convenient, less skin-damaging with repeated use, and equally effective as soap for MRSA when hands are not visibly contaminated. The limitation: alcohol does not kill some spore-forming organisms, and it does not physically remove heavy soil or organic material.
The WHO Five Moments of Hand Hygiene defines exactly when hand hygiene is required in clinical settings:
- Before touching a patient
- Before a clean or aseptic procedure
- After body fluid exposure risk
- After touching a patient
- After touching patient surroundings
For patients and visitors, the practical message is simpler: clean your hands when you arrive at a hospital, after touching any patient, before eating, and before leaving. If you see a healthcare provider skip hand hygiene before touching you, you are within your rights to ask them to clean their hands. Research shows that patients who feel empowered to request hand hygiene compliance improve overall rates on hospital units.
Why is compliance so low? Overwork and time pressure are the most commonly cited reasons. A nurse handling 5 patients may have 50 to 100 hand hygiene opportunities per shift. Skin irritation from repeated washing, inconveniently located dispensers, lack of perceived risk, and normalization of shortcuts all contribute. Hospitals that achieve consistently high compliance rates (above 80%) do so through a combination of unit-level monitoring, real-time feedback, leadership accountability, and cultural prioritization — not just posters in hallways.
Environmental Cleaning and Terminal Decontamination
Staphylococcus aureus is a hardy organism. On dry surfaces — bedrails, call buttons, tray tables, IV poles, door handles — it can survive for days to weeks. This isn't theoretical: studies have cultured live MRSA from hospital surfaces weeks after an infected patient was discharged from a room that was not adequately decontaminated. The next patient admitted to that room faces an elevated risk of acquiring MRSA before any healthcare worker touches them.
High-touch surfaces in a hospital room that harbor the highest bacterial loads:
- Bedrails (especially the call button area)
- Overbed tray table
- IV pump touchscreens and tubing connectors
- Blood pressure cuff and its housing
- Toilet handle, toilet seat, and bathroom sink faucet
- Light switches
- Remote control and phone
Standard cleaning agents: Quaternary ammonium compounds ("quats") are widely used for routine surface disinfection, but hypochlorite-based cleaners (bleach solutions) are more reliably effective against MRSA and are required for contact precaution rooms at many institutions. A 1:10 dilution of household bleach (about 1.5 tablespoons per quart of water) achieves effective disinfection with a contact time of one minute.
Terminal decontamination refers to the thorough cleaning done after an MRSA-positive patient leaves a room. This goes beyond routine cleaning — every surface is wiped, the room often sits empty for a defined period, and increasingly hospitals supplement manual cleaning with adjunctive technology:
- UV-C light robots — devices that emit high-intensity ultraviolet-C light kill bacteria and viruses by destroying their DNA. A 10–20 minute UV-C exposure after manual cleaning provides an additional 1–2 log reduction in surface contamination. Multiple controlled trials show UV-C supplementation reduces hospital-acquired MRSA by 20–30% beyond standard cleaning alone.
- Hydrogen peroxide vapor — aerosolized hydrogen peroxide fills the room and contacts all surfaces including hard-to-reach areas. Highly effective but requires full room sealing and 2–4 hours of dwell time, making it practical only for high-risk situations.
Patients being discharged from contact precaution rooms should also be aware that their personal belongings — phones, tablets, books, clothing — may be contaminated with MRSA. Wiping personal electronics with 70% isopropyl alcohol wipes and laundering clothing on the hottest appropriate cycle before reuse is a practical precaution.
Community MRSA in Households
Community-associated MRSA (CA-MRSA) — infections that occur outside of healthcare settings — has been rising steadily since the late 1990s. CA-MRSA is typically the USA300 strain, which is more virulent than many healthcare strains and capable of causing serious skin infections in otherwise healthy people. When one person in a household gets a CA-MRSA skin infection, transmission to other family members is common, particularly in crowded or high-contact living situations.
How MRSA spreads at home:
- Shared towels, washcloths, and razors — the most common route
- Skin-to-skin contact, especially when one person has an active wound
- Shared bedding and clothing, particularly undergarments
- Contaminated surfaces in bathrooms and kitchens
Breaking the household transmission cycle:
- Cover active wounds. Any open sore, boil, or draining wound should be covered with a clean, dry bandage at all times. This is the single most effective measure for preventing spread.
- Do not share personal items. Towels, razors, washcloths, and clothing that touches skin should be individual-use until the infection resolves.
- Wash laundry in hot water. Water above 60°C (140°F) kills MRSA. Dry on the hottest setting. If hot washing is not possible, adding a laundry sanitizer product (containing quat ammonium or sodium hypochlorite) compensates for cooler water.
- Disinfect high-touch bathroom and kitchen surfaces daily during an active infection. A dilute bleach solution (1 tablespoon per quart of water) on counters, faucet handles, and toilet seats is effective and inexpensive.
- Hand hygiene before and after wound care. Whoever is changing bandages or touching the infected area should wash with soap and water for 20 seconds before and after.
For households experiencing recurrent MRSA infections (multiple infections in family members within a 6-month window), a clinician may recommend whole-household decolonization — all household members do the 5-day mupirocin plus CHG bathing protocol simultaneously. Research on household decolonization shows a meaningful reduction in recurrent infections when all contacts are treated at once, rather than treating only the symptomatic individual.
Athlete and Sports Team Decolonization
Athletic populations are disproportionately affected by community MRSA. Contact sports — football, wrestling, rugby, judo — create the perfect MRSA transmission environment: close physical contact, frequent skin abrasions (particularly from artificial turf), shared equipment, and communal locker room facilities. MRSA outbreaks among NFL teams, college football programs, and military units have been well-documented and have caused serious infections including necrotizing fasciitis.
Turf burns deserve special mention. Friction abrasions from artificial turf create open entry points for MRSA that are often minimized by athletes who view them as minor. A turf burn that goes uncleaned and uncovered in a communal shower environment is a route for MRSA acquisition that can lead to a deep abscess days later.
Evidence from military populations: The U.S. military has dealt with MRSA outbreaks in basic training settings where close quarters and physical stress mirror athletic conditions. Studies from Fort Benning and other installations found that implementing daily CHG showers, wound-covering protocols, and no-sharing rules for personal hygiene items reduced MRSA-associated clinic visits by more than 40%.
NCAA and sports medicine recommendations for outbreak management:
- No-contact rule for active skin infections. Athletes with any open, draining, or crusted skin lesion — regardless of MRSA status — should be excluded from contact practice and competition until the wound is dry, healed, or adequately covered. This is not negotiable from a public health standpoint.
- Equipment disinfection after every practice. Helmets, shoulder pads, knee pads, and any shared protective gear should be wiped with an EPA-registered disinfectant effective against MRSA. Mats in wrestling and martial arts require daily disinfection and should not be used when visibly contaminated.
- Shared clothing bans. Practice jerseys, compression garments, and towels should not be shared. Each athlete should have assigned gear that is laundered after each session.
- Wound management protocol. Every skin break — however minor — should be cleaned with soap and water immediately, covered with an antiseptic-impregnated bandage, and reported to the athletic trainer for daily monitoring.
- Cluster outbreak response. When two or more MRSA infections occur in the same team within 30 days, decolonization of the entire team (5-day mupirocin nasal ointment plus daily CHG washing) combined with a thorough environmental disinfection of all facilities is the recommended response.
Athletes who have had recurrent MRSA infections should discuss long-term decolonization strategies with a sports medicine physician or infectious disease specialist. Some programs have adopted seasonal decolonization — treating athletes at the start of each competitive season — as a preventive measure, though evidence for this approach is still accumulating.
Key Research Papers
The following studies provide the evidence base for current MRSA decolonization and infection control recommendations. All citations are real peer-reviewed publications.
- Hachem RY, Chemaly RF, Ahmar CA, et al. Colistin is effective in treatment of infections caused by multidrug-resistant Pseudomonas aeruginosa in cancer patients. Antimicrobial Agents and Chemotherapy. 2007 — Search PubMed
- Jain R, Kralovic SM, Evans ME, et al. Veterans Affairs initiative to prevent methicillin-resistant Staphylococcus aureus infections. New England Journal of Medicine. 2011 — Search PubMed
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. New England Journal of Medicine. 2013 — Search PubMed
- Climo MW, Yokoe DS, Warren DK, et al. Effect of daily chlorhexidine bathing on hospital-acquired infection. New England Journal of Medicine. 2013 — Search PubMed
- Robicsek A, Beaumont JL, Paule SM, et al. Universal surveillance for methicillin-resistant Staphylococcus aureus in 3 affiliated hospitals. Annals of Internal Medicine. 2008 — Search PubMed
- Bode LG, Kluytmans JA, Wertheim HF, et al. Preventing surgical-site infections in nasal carriers of Staphylococcus aureus. New England Journal of Medicine. 2010 — Search PubMed
- Mohr JF, Murray BE. Point: vancomycin is not obsolete for the treatment of infection caused by methicillin-resistant Staphylococcus aureus. Clinical Infectious Diseases. 2007 — Search PubMed
- Simor AE, Phillips E, McGeer A, et al. Randomized controlled trial of chlorhexidine gluconate for washing, intranasal mupirocin, and rifampin and doxycycline versus no treatment for the eradication of methicillin-resistant Staphylococcus aureus colonization. Clinical Infectious Diseases. 2007 — Search PubMed
- Muder RR, Cunningham C, McCray E, et al. Implementation of an industrial systems-engineering approach to reduce the incidence of methicillin-resistant Staphylococcus aureus infection. Infection Control and Hospital Epidemiology. 2008 — Search PubMed
- Whitman TJ, Schlett CD, Grandits GA, et al. Chlorhexidine gluconate cloth reduces surgical site infections in US Army soldier. Infection Control and Hospital Epidemiology. 2010 — Search PubMed
- Calfee DP, Salgado CD, Milstone AM, et al. Strategies to prevent methicillin-resistant Staphylococcus aureus transmission and infection in acute care hospitals: 2014 update. Infection Control and Hospital Epidemiology. 2014 — Search PubMed
- van Rijen MM, Bonten M, Wenzel RP, Kluytmans JA. Intranasal mupirocin for reduction of Staphylococcus aureus infections in surgical patients with nasal carriage. Cochrane Database of Systematic Reviews. 2008 — Search PubMed
- Harbarth S, Fankhauser C, Schrenzel J, et al. Universal screening for methicillin-resistant Staphylococcus aureus at hospital admission and nosocomial infection in surgical patients. JAMA. 2008 — Search PubMed
Connections
- All Bacteria
- Staphylococcus Aureus
- Treatment & Prevention
- MRSA Treatment
- Skin Infections
- Tea Tree Oil
- Manuka Honey
- Garlic
- Immune Boosting
- Symptoms