Bacteria — Pathogens, Infections, and Antimicrobial Resistance
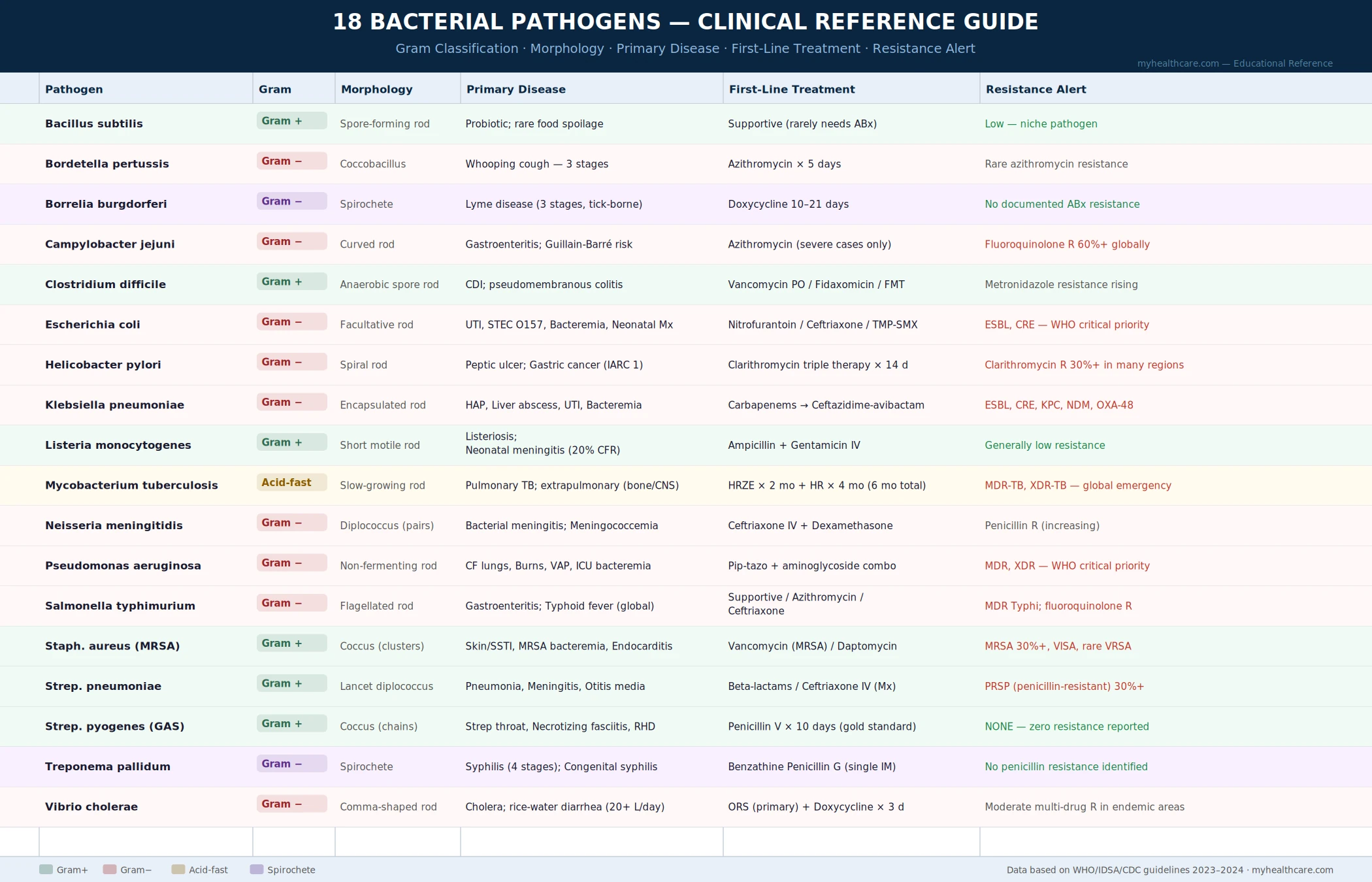
Bacteria are single-celled prokaryotes that live in every environment on Earth — and a small but medically critical subset cause disease in humans. The 18 bacteria profiled here range from the foodborne killers responsible for millions of annual hospitalizations to the sexually transmitted spirochete behind syphilis; from the harmless soil resident that produces life-saving enzymes to the lung-destroying pathogen driving the global antibiotic resistance crisis. Understanding how each bacterium behaves — how it enters the body, what it damages, and how treatment works (or is failing) — is essential for informed health decisions.
Bacillus subtilis
A common soil and gut bacterium widely used as a probiotic and in industrial enzyme production; rarely pathogenic but important in biofilm research.
Bordetella pertussis
The cause of whooping cough (pertussis) — a highly contagious respiratory infection whose 100-day cough is dangerous for infants.
Borrelia burgdorferi
The spirochete transmitted by deer ticks that causes Lyme disease — the most common vector-borne disease in the United States.
Campylobacter jejuni
The leading bacterial cause of foodborne diarrhea worldwide, most often from undercooked poultry; can trigger Guillain-Barré syndrome.
Clostridium difficile
C. diff — the antibiotic-associated colitis pathogen responsible for 500,000 US infections and 15,000 deaths annually.
Escherichia coli
Most strains are harmless gut residents, but pathogenic types cause urinary tract infections, traveler's diarrhea, and life-threatening hemolytic uremic syndrome.
Helicobacter pylori
The stomach-dwelling bacterium behind most peptic ulcers and the leading infectious cause of gastric cancer; infects half the world's population.
Klebsiella pneumoniae
A hospital-acquired pathogen causing pneumonia and bloodstream infections, now among the most dangerous antibiotic-resistant "superbug" threats.
Listeria monocytogenes
A foodborne pathogen that grows in refrigerators and is uniquely dangerous to pregnant women, newborns, and immunocompromised individuals.
Mycobacterium tuberculosis
The cause of tuberculosis — an airborne infection that kills over a million people annually and has infected one quarter of the world's population.
Neisseria meningitidis
The bacterium behind bacterial meningitis and septicemia — a medical emergency with a fatality rate of 10–15% even with treatment.
Pseudomonas aeruginosa
An opportunistic pathogen that devastates cystic fibrosis lungs and is a leading cause of hospital-acquired infections, with rising multidrug resistance.
Salmonella Typhimurium
A major cause of salmonellosis from contaminated eggs, poultry, and produce; also the model organism for understanding bacterial invasion of gut cells.
Staphylococcus aureus
A versatile pathogen causing skin infections, pneumonia, and bloodstream infections; MRSA strains are a critical antibiotic resistance problem worldwide.
Streptococcus pneumoniae
The leading cause of bacterial pneumonia, meningitis, and ear infections globally; vaccines have dramatically reduced disease but resistant strains are emerging.
Streptococcus pyogenes
Group A Strep — the cause of strep throat, scarlet fever, and the life-threatening necrotizing fasciitis (flesh-eating disease).
Treponema pallidum
The spirochete behind syphilis — a four-stage STI resurging to multi-decade highs with devastating congenital outcomes if untreated in pregnancy.
Vibrio cholerae
The cause of cholera — a waterborne disease producing the most severe diarrhea known to medicine, capable of killing within hours from dehydration.
Table of Contents
- What Are Bacteria?
- How Bacteria Cause Disease
- Routes of Transmission
- The Antibiotic Resistance Crisis
- Diagnosis and Identification
- Prevention Principles
- Key Research Papers
- Featured Videos
1. What Are Bacteria?
Bacteria are single-celled organisms belonging to the domain Prokaryota — they lack a membrane-bound nucleus and the complex internal organelles found in the human cells they infect. Despite this apparent simplicity, bacteria are extraordinarily successful: they reproduce rapidly (some doubling every 20 minutes), adapt quickly through mutation and horizontal gene transfer, and have colonized every environment on Earth, from deep-sea hydrothermal vents to the skin and gut of every human alive.
The human body hosts trillions of bacteria, the vast majority of which are beneficial or neutral. The gut microbiome alone comprises over a thousand species performing essential functions — synthesizing vitamins, training the immune system, fermenting fibers, and outcompeting pathogens for space and nutrients. Only a small fraction of the roughly 30,000 known bacterial species are capable of causing human disease, and even among those, illness depends on a complex interplay between the virulence of the bacterium, the route of exposure, and the state of the host's immune defenses.
Bacteria are classified by multiple characteristics: their shape (spheres called cocci, rods called bacilli, spirals called spirochetes or spirilla), their response to the Gram stain (Gram-positive organisms retain purple dye because of their thick peptidoglycan wall; Gram-negative organisms have a thinner peptidoglycan layer but an outer membrane, giving them distinct antibiotic susceptibility profiles), their oxygen requirements (aerobic, anaerobic, or facultative), and their growth requirements in culture.
2. How Bacteria Cause Disease
Pathogenic bacteria have evolved diverse mechanisms to breach the body's defenses and establish infection. Understanding these mechanisms explains why different bacteria cause disease in different organs, why some are more dangerous than others, and why certain treatments work while others fail.
Toxin production is one of the most powerful bacterial weapons. Some bacteria cause disease primarily by secreting toxins rather than by invading tissue directly. Clostridioides difficile releases toxins A and B that destroy the colon lining; Vibrio cholerae produces a toxin that causes the gut to pour out water; Bacillus anthracis secretes a lethal toxin that disrupts immune signaling. Even bacteria killed by the immune system can release toxins from their damaged cell walls (endotoxins) that trigger the overwhelming inflammatory cascade of septic shock.
Adhesion and invasion allow bacteria to attach to and penetrate host cells, evading the physical barrier that normally excludes them. Helicobacter pylori burrows through the stomach's mucus layer to reach and damage the epithelium underneath. Listeria monocytogenes triggers its own phagocytosis, then escapes the phagosome and hijacks the host cell's actin cytoskeleton to propel itself from cell to cell.
Immune evasion is a hallmark of the most dangerous pathogens. Treponema pallidum coats itself in host proteins to avoid antibody recognition. Mycobacterium tuberculosis survives inside macrophages — the immune cells designed to kill bacteria — by blocking the fusion of the phagosome with the lysosome. Staphylococcus aureus secretes protein A, which binds immunoglobulin and blocks opsonization.
Biofilm formation enables bacteria to attach to surfaces (prosthetic heart valves, urinary catheters, hospital equipment) and build organized communities encased in a protective polysaccharide matrix. Biofilm bacteria are up to a thousand times more resistant to antibiotics than their free-floating counterparts and can persistently shed bacteria into the bloodstream.
3. Routes of Transmission
How a bacterium reaches a new host defines its epidemiology, its risk groups, and how it can be prevented. The major routes are:
- Foodborne and waterborne: Ingestion of contaminated food or water is the route for Salmonella, Campylobacter, Listeria, E. coli O157:H7, and Vibrio cholerae. Contamination occurs at any point from farm to table, and the risk is highest with raw or undercooked animal products, unpasteurized dairy, and fresh produce irrigated with contaminated water.
- Airborne and respiratory droplets: Mycobacterium tuberculosis, Bordetella pertussis, Streptococcus pneumoniae, and Neisseria meningitidis spread through the air when infected people cough, sneeze, or speak. Enclosed spaces and crowded living conditions amplify transmission.
- Direct contact and sexual transmission: Treponema pallidum (syphilis) and Neisseria gonorrhoeae spread through sexual contact with infectious lesions or mucous membranes. Staphylococcus aureus spreads through direct skin-to-skin contact and contaminated surfaces.
- Vector-borne: Borrelia burgdorferi (Lyme disease) is transmitted through the bite of infected Ixodes ticks. The bacterium lives in the tick's midgut and must be transferred during a blood meal lasting at least 36–48 hours.
- Healthcare-associated: Clostridioides difficile, Pseudomonas aeruginosa, and Klebsiella pneumoniae thrive in hospital environments. Disruption of the normal microbiome by antibiotics, invasive devices (catheters, ventilators), and immunosuppression create the conditions for these opportunistic pathogens.
4. The Antibiotic Resistance Crisis
Antibiotic resistance is one of the most urgent public health threats of the 21st century. When bacteria are exposed to antibiotics, susceptible organisms die while naturally resistant mutants survive and reproduce — a straightforward application of natural selection. Horizontal gene transfer, in which bacteria share resistance genes with each other through plasmids and other mobile genetic elements, accelerates this process dramatically: a resistance gene that arose in one species can spread to entirely unrelated bacteria within hours.
The consequences are already severe. The WHO's "ESKAPE" pathogens — Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species — collectively represent the bacteria most likely to be multidrug-resistant and to cause treatment failures in hospitals worldwide. Several of the 18 bacteria profiled on this site feature prominently in this crisis. MRSA (methicillin-resistant Staphylococcus aureus) became one of the first widely recognized superbugs; carbapenem-resistant Klebsiella pneumoniae and Pseudomonas aeruginosa now present near-untreatable scenarios in intensive care units.
Antibiotic overuse in human medicine and massive use in agriculture (where antibiotics have historically been given to promote livestock growth, not just treat infections) have both contributed to the resistance crisis. The pipeline of new antibiotics has also slowed dramatically because developing antibiotics is commercially unattractive: a successful antibiotic is used for a short course and then reserved to minimize resistance, which is the opposite of the business model that drives drug development.
5. Diagnosis and Identification
Identifying the specific bacterium causing an infection is essential for selecting the right treatment and for controlling spread. Several methods are used:
- Culture: Growing bacteria from a blood, urine, sputum, wound, or stool sample on nutrient agar remains the gold standard. It identifies the organism and, crucially, allows antibiotic sensitivity testing (determining which antibiotics actually kill this specific isolate). The drawback is time: most cultures take 24–72 hours, and some organisms (like Mycobacterium tuberculosis) grow so slowly that cultures may take weeks.
- Gram stain and microscopy: A rapid, inexpensive technique that categorizes bacteria by cell wall structure (Gram-positive vs. Gram-negative) and shape. This can guide empiric antibiotic choice while culture results are pending. Treponema pallidum is a notable exception: it is too thin to stain and requires darkfield microscopy.
- Molecular diagnostics (PCR): Polymerase chain reaction tests detect bacterial DNA directly in a sample, often returning results within hours. PCR is particularly valuable for organisms difficult or slow to culture (tuberculosis, Lyme disease) and in identifying antibiotic resistance genes.
- Serologic testing: Blood tests that detect antibodies the immune system has made against bacterial antigens. Useful for diagnosing past or chronic infection (syphilis, Lyme disease, typhoid) but often unreliable in the very early stages when antibody levels are still low.
- Antigen tests: Detect bacterial proteins directly, rather than the antibody response. Rapid antigen tests for Streptococcus pneumoniae urinary antigen and Clostridioides difficile toxins are available as point-of-care tests.
6. Prevention Principles
Prevention strategies depend on the route of transmission but share common themes:
- Vaccination is the most powerful tool against several of the bacteria covered here. Vaccines against Bordetella pertussis (DTaP/Tdap), Streptococcus pneumoniae (PCV15, PCV20, PPSV23), and Neisseria meningitidis (MenACWY, MenB) have dramatically reduced disease and death. No vaccines exist yet for Staphylococcus aureus, Clostridioides difficile, or Treponema pallidum, despite decades of research.
- Food safety: Cooking meat to safe temperatures, avoiding cross-contamination in kitchens, practicing proper handwashing, and avoiding raw milk and other unpasteurized products are the front-line defenses against foodborne bacteria.
- Water and sanitation: Safe water supply, sewage treatment, and handwashing facilities are the most cost-effective public health interventions in history, eliminating cholera and typhoid from countries that implement them.
- Antibiotic stewardship: Using antibiotics only when necessary, completing prescribed courses, and avoiding using antibiotics for viral infections all slow the development and spread of resistance. Healthcare systems that implement formal stewardship programs measurably reduce resistance rates.
- Sexual health practices: Consistent condom use, regular STI screening, and partner notification are the primary tools against sexually transmitted bacteria including Treponema pallidum.
- Hospital infection control: Hand hygiene, contact precautions for colonized patients, environmental cleaning, and prudent use of invasive devices dramatically reduce healthcare-associated infections from C. difficile, MRSA, Pseudomonas, and Klebsiella.
Key Research Papers
Foundational and recent research on bacterial pathogenesis, antibiotic resistance, and public health impact of the organisms covered in this section.
- Murray CJL, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. PMID 35065702 — Estimated 1.27 million deaths attributable directly to AMR in 2019, establishing the global scope of the resistance crisis.
- Tacconelli E, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318–327. PMID 29276051 — WHO framework identifying the bacteria for which new antibiotics are most urgently needed.
- Laxminarayan R, et al. Antibiotic resistance — the need for global solutions. Lancet. 2013;382(9912):1057–1098. PMID 24252483 — Landmark review on the global dimensions of antibiotic resistance and the policy frameworks required to address them.
- Collaborators GBDLRI. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016. Lancet Infect Dis. 2018;18(11):1191–1210. PMID 30243584 — Defines the enormous burden of bacterial lower respiratory infections globally, including S. pneumoniae and H. influenzae.
- Kaper JB, Nataro JP, Mobley HLT. Pathogenic Escherichia coli. Nat Rev Microbiol. 2004;2(2):123–140. PMID 15040260 — Comprehensive review of how pathogenic E. coli strains cause disease through diverse virulence mechanisms.
- Blaser MJ. Who are we? Indigenous microbes and the ecology of human diseases. EMBO Rep. 2006;7(10):956–960. PMID 17016449 — Influential piece on the dual nature of bacteria as both residents and pathogens, and the consequences of disrupting the microbiome.
- Fischbach MA, Walsh CT. Antibiotics for emerging pathogens. Science. 2009;325(5944):1089–1093. PMID 19713519 — Reviews the mechanisms of antibiotic action and the challenges of developing new drugs for resistant organisms.
- Davies J, Davies D. Origins and evolution of antibiotic resistance. Microbiol Mol Biol Rev. 2010;74(3):417–433. PMID 20805405 — Traces the evolutionary origins of resistance genes and how horizontal gene transfer propagates resistance across bacterial species.
- Mandell GL, Bennett JE, Dolin R, eds. Chapter: Principles of antimicrobial therapy. In: Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 8th ed. Elsevier; 2015. — Standard reference text covering mechanisms, spectrum, and clinical use of all major antibiotic classes.
- World Health Organization. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report 2022. Geneva: WHO; 2022. PMID 37027254 — WHO's most comprehensive global surveillance dataset on resistance trends across pathogens and countries.
Live PubMed Searches
Each link opens a live PubMed query returning current research.
- Antibiotic resistance global burden
- Bacterial pathogenesis virulence mechanisms
- ESKAPE pathogens treatment
- Foodborne bacterial infection epidemiology
- Hospital-acquired infection prevention
- Gut microbiome bacterial pathogen colonization
Connections
- Bacillus subtilis
- Bordetella pertussis (Whooping Cough)
- Borrelia burgdorferi (Lyme Disease)
- Campylobacter jejuni
- Clostridium difficile (C. diff)
- Escherichia coli (E. coli)
- Helicobacter pylori
- Klebsiella pneumoniae
- Listeria monocytogenes
- Mycobacterium tuberculosis (TB)
- Neisseria meningitidis (Meningococcus)
- Pseudomonas aeruginosa
- Salmonella Typhimurium
- Staphylococcus aureus (MRSA)
- Streptococcus pneumoniae
- Streptococcus pyogenes (Group A Strep)
- Treponema pallidum (Syphilis)
- Vibrio cholerae (Cholera)
- Parasites
- Infectious Disease
- All Conditions
- Lab Tests