Campylobacter jejuni: The Most Common Bacterial Cause of Food Poisoning
Symptoms & Diagnosis
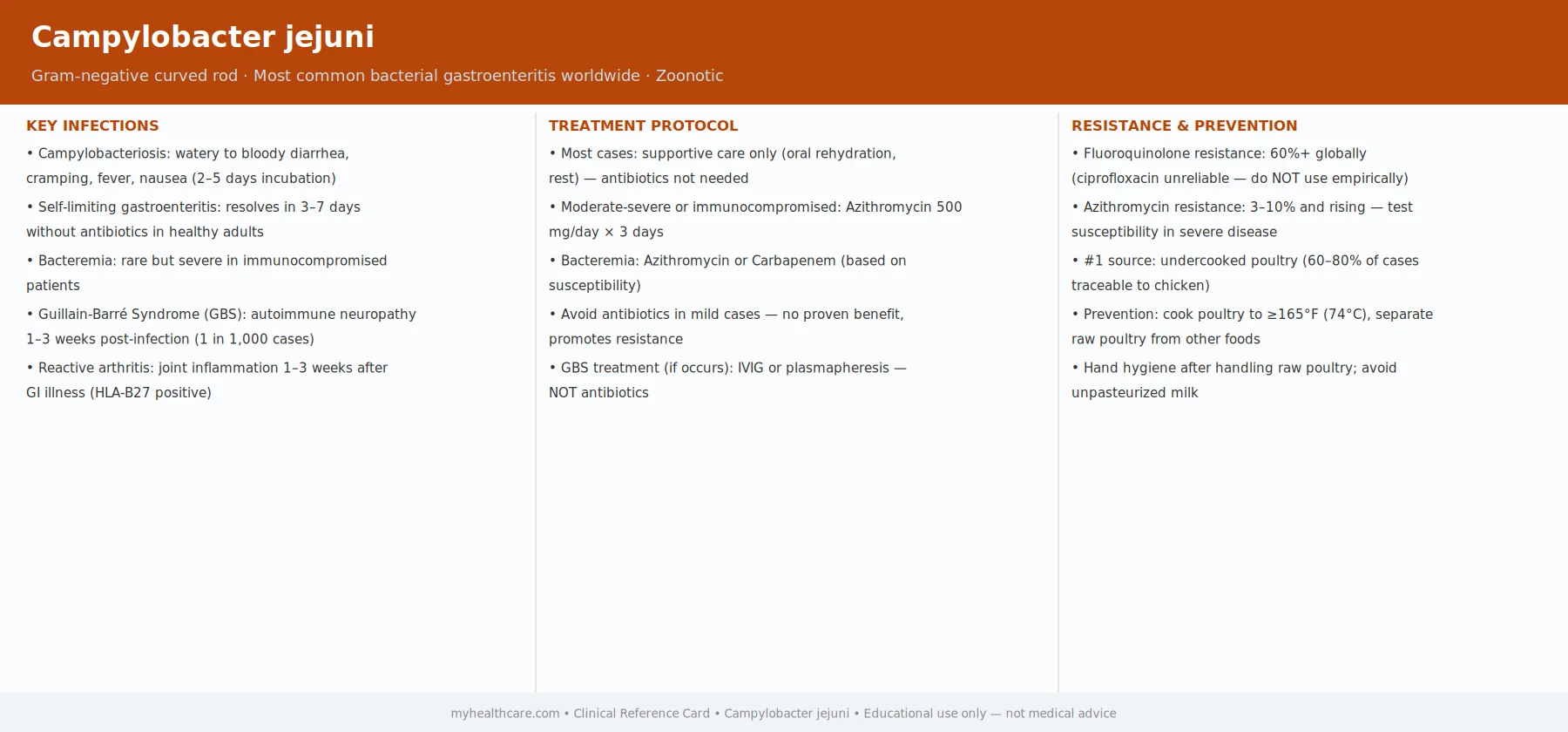
The most common bacterial cause of food poisoning — and the rare but serious Guillain-Barré link.
Diarrhea & GI Symptoms
The typical course: fever, cramps, watery or bloody diarrhea lasting 3-7 days.
Guillain-Barré Syndrome
How a gut infection can cause paralysis — the post-infectious nerve damage mechanism.
Diagnosis Tests
Stool culture requirements, PCR multiplex panels, and blood cultures for bacteremia.
Treatment & Prevention
Most cases resolve without antibiotics — when treatment is actually needed.
Antibiotic Treatment
Azithromycin as first-line, why ciprofloxacin often fails, and invasive disease treatment.
Food Safety
Poultry — the main reservoir — and how to handle it safely at home.
Antibiotic Resistance
Fluoroquinolone resistance driven by veterinary use in poultry — why ciprofloxacin now often fails.
Campylobacter jejuni causes more cases of bacterial food poisoning than Salmonella in many developed countries, yet it receives far less public attention. The bacteria live harmlessly in the gut of poultry, and most human infections come from handling or eating undercooked chicken, drinking unpasteurized milk, or consuming contaminated water. For most people the illness is a miserable but self-limiting few days of diarrhea, cramping, and fever. For a small number, however, an immune reaction triggered by the infection can cause Guillain-Barré syndrome — an ascending paralysis that can require weeks of hospitalization and intensive care. Understanding how Campylobacter spreads and how to prevent it is the key message of this page.
Table of Contents
- What Campylobacter Is
- How People Get Infected
- Symptoms
- Guillain-Barré Syndrome Complication
- Diagnosis
- Treatment
- Prevention
- Research Papers
- Connections
- Featured Videos
What Campylobacter Is
Campylobacter jejuni is a Gram-negative, spiral-shaped, microaerophilic bacterium — meaning it needs a low-oxygen environment to grow and does not thrive exposed to normal air. It was first recognized as a human pathogen in 1977 and is now the leading bacterial cause of gastroenteritis (stomach and intestinal inflammation) in the United States, Europe, and Australia.
The bacterium is extraordinarily common in poultry: studies consistently find Campylobacter in 50–80% of raw retail chicken carcasses in high-income countries. The birds are not made ill by it — their body temperature is high enough that the bacteria colonize without causing disease. But when those bacteria transfer to a human — through undercooking, kitchen cross-contamination, or direct handling — the result is a significant infection. The CDC estimates roughly 1.5 million human infections per year in the United States alone, causing about 120 deaths.
Unlike Salmonella, Campylobacter does not multiply in food sitting on a counter — it is fragile outside a living host. The infectious dose is, however, very low: as few as 500 bacteria can cause illness. A single drop of raw chicken juice can contain enough organisms to infect someone if it reaches food that will be eaten without further cooking.
How People Get Infected
The vast majority of human Campylobacter infections come from a small number of well-understood routes:
- Undercooked poultry. Chicken is by far the most important source. The bacteria are killed reliably when poultry reaches an internal temperature of 165°F (74°C) throughout. Pink or rare chicken is a meaningful risk.
- Cross-contamination in the kitchen. Raw chicken juice on a cutting board, knife, or hand can contaminate salad vegetables, bread, or other ready-to-eat foods. This is a common route even when the chicken itself is cooked thoroughly.
- Unpasteurized (raw) milk. Cattle can also carry Campylobacter. Outbreaks linked to raw milk consumption are well documented and tend to affect multiple family members at once.
- Contaminated water. Untreated surface water (streams, wells, camping water sources) can carry the organism. Waterborne outbreaks have occurred after heavy rains that overwhelm municipal water treatment.
- Contact with pets. Young dogs and cats, particularly those with diarrhea, can be a source of infection, especially for young children.
- Travel. Visiting countries with less stringent food safety infrastructure is a significant risk factor. Campylobacter is a common cause of traveler's diarrhea.
Person-to-person spread is uncommon because the organism does not persist well outside a warm host, but it can occur in households with young children in diapers who have active infection.
Symptoms
After exposure, symptoms typically begin 2 to 5 days later (the incubation period can range from 1 to 10 days). The illness usually lasts 3 to 7 days and then resolves on its own without treatment.
The hallmark features of campylobacteriosis are:
- Diarrhea — often profuse, and frequently bloody. Bloody diarrhea is more characteristic of Campylobacter than of many other foodborne pathogens and reflects the bacterium's ability to invade the intestinal wall and trigger significant inflammation.
- Abdominal cramping — often severe, sometimes mistaken for appendicitis, particularly in children and young adults where the cramping can precede diarrhea and mimic a surgical emergency.
- Fever — typically 38–40°C (100–104°F), accompanying the diarrhea.
- Nausea and vomiting — present in a minority of cases; the illness is more consistently diarrheal than emetic.
- Malaise and headache — a flu-like feeling often precedes the gastrointestinal symptoms by a day or two.
Most healthy adults recover fully without any lasting effects. Severe dehydration requiring IV fluids is the main risk, particularly in infants, the elderly, and immunocompromised individuals. These groups should be watched closely and may need hospitalization.
When to seek care promptly: High fever, bloody diarrhea lasting more than three days, signs of significant dehydration (dizziness, no urination, sunken eyes in children), or any neurological symptoms (weakness, numbness, difficulty walking) after a diarrheal illness all warrant prompt medical evaluation.
Guillain-Barré Syndrome Complication
The most feared complication of Campylobacter infection is Guillain-Barré syndrome (GBS) — an autoimmune attack on the peripheral nervous system that can cause ascending paralysis from the legs upward, sometimes reaching the muscles of breathing and requiring mechanical ventilation.
The mechanism is molecular mimicry. Certain strains of C. jejuni carry surface carbohydrates on their outer membrane called lipo-oligosaccharides that closely resemble the molecular structure of gangliosides — fats found on the surface of human nerve cells. When the immune system mounts an antibody response to clear the bacterial infection, some of those antibodies mistakenly cross-react with the patient's own nerve tissue, causing demyelination (stripping of the nerve insulation) and nerve damage.
Key facts about GBS after Campylobacter:
- Campylobacter infection is the single most common identifiable trigger of GBS globally, preceding about 30% of all GBS cases.
- GBS itself is rare: only about 1 in 1,000 to 1 in 2,000 Campylobacter infections leads to GBS. But because Campylobacter is so common, this accounts for a significant absolute number of GBS cases each year.
- Symptoms of GBS typically begin 1 to 3 weeks after the gastrointestinal illness, often after the diarrhea has resolved — which can make the connection easy to miss.
- Early symptoms include tingling or weakness in the legs that ascends upward. Most patients reach their weakest point within 2 to 4 weeks, then begin a slow recovery that may take months to over a year.
- About 15–20% of GBS patients are left with lasting disability; 3–5% die even with intensive care.
Any new weakness, numbness, or difficulty walking in the days to weeks after a diarrheal illness should be treated as a medical emergency until GBS is ruled out. The treatment — intravenous immunoglobulin (IVIg) or plasma exchange (plasmapheresis) — is most effective when started early.
Diagnosis
In most cases of routine food poisoning, a doctor will not send specific tests — the illness is self-limiting and testing would not change management. However, testing is indicated when:
- Diarrhea is severe, bloody, or lasting more than a week.
- The patient is immunocompromised, elderly, or very young.
- There is an outbreak situation (multiple people at the same event or household affected).
- GBS is suspected and a triggering infection needs to be identified.
The standard diagnostic approach:
- Stool culture. Traditional culture on selective media can grow Campylobacter from a stool sample, but requires specific microaerophilic conditions and incubation at 42°C. Results typically take 48–72 hours.
- PCR-based stool panels. Multiplex PCR panels that test simultaneously for many pathogens (including Campylobacter, Salmonella, norovirus, and others) have become widely available and give results within hours.
- Stool antigen tests. Rapid immunoassays for Campylobacter antigens are available but less sensitive than culture or PCR.
- Serology (antibody testing). Used mainly in GBS workup to confirm prior Campylobacter infection when the patient no longer has active diarrhea.
Treatment
Most Campylobacter infections in otherwise healthy adults and older children do not require antibiotics. The illness is self-limiting, and by the time culture results are back, most patients are already improving. The mainstay of treatment is:
- Fluid and electrolyte replacement. Oral rehydration solution (ORS) — water with the right balance of salt and sugar — is the cornerstone of treatment. Commercially available ORS sachets or sports drinks diluted with water are practical options. Severe dehydration may require intravenous fluids.
- Rest and symptom management. Avoiding dehydrating beverages (alcohol, excess caffeine), eating bland low-fiber foods when appetite returns, and resting are the practical advice given to most patients.
Antibiotics are used in specific circumstances:
- Severe illness with high fever and profuse bloody diarrhea where the patient is not improving.
- Immunocompromised patients, in whom the infection can become bacteremic (spread to the blood) and life-threatening.
- Azithromycin is the preferred first-line antibiotic. Fluoroquinolones such as ciprofloxacin, historically a standard choice, now face significant resistance — Campylobacter is one of the top pathogens on the WHO's antibiotic-resistance watch list, and ciprofloxacin resistance exceeds 50% in many countries.
Antidiarrheal drugs such as loperamide (Imodium) are generally avoided in bloody diarrhea or suspected invasive infection, as slowing gut transit can worsen the illness.
Prevention
Because Campylobacter is so widespread in commercial poultry, complete elimination from the food supply is not realistic. Prevention focuses on breaking the chain of transmission between raw poultry and the mouth:
- Cook poultry thoroughly to an internal temperature of at least 165°F (74°C), measured with a food thermometer in the thickest part of the meat.
- Separate raw poultry from all other foods in shopping bags, in the refrigerator (use the bottom shelf with a tray to catch drips), and on kitchen work surfaces.
- Wash hands thoroughly with soap and water after handling raw poultry and before touching other foods or surfaces. Alcohol hand gels are less effective than soap against Campylobacter.
- Sanitize surfaces and utensils that have contacted raw chicken before using them for other foods. A dilute bleach solution or a food-safe disinfectant spray is effective.
- Avoid unpasteurized milk and dairy products. Pasteurization reliably kills Campylobacter.
- Drink safe water. Use treated or boiled water when camping or traveling to areas with uncertain water quality.
- Handle pets carefully. Wash hands after contact with dogs or cats that have diarrhea, and have sick pets evaluated by a veterinarian.
There is currently no licensed human vaccine against Campylobacter, though several candidates are in clinical development, driven partly by the military's need to protect personnel deploying to high-risk areas.
Research Papers
- Kaakoush NO, Casédine N, Mitchell HM, Man SM. Global epidemiology of Campylobacter infection. Clin Microbiol Rev. 2015;28(3):687–720. — Search PubMed — Comprehensive review of worldwide Campylobacter burden, transmission routes, and trends in antibiotic resistance.
- Nachamkin I, Allos BM, Ho T. Campylobacter species and Guillain-Barré syndrome. Clin Microbiol Rev. 1998;11(3):555–567. — Search PubMed — Seminal review establishing the molecular mimicry mechanism linking C. jejuni lipo-oligosaccharides to GBS pathogenesis.
- Young KT, Davis LM, DiRita VJ. Campylobacter jejuni: molecular biology and pathogenesis. Nat Rev Microbiol. 2007;5(9):665–679. — Search PubMed — Detailed review of how C. jejuni invades the intestinal epithelium and evades host immunity.
- Tack DM, Ray L, Griffin PM, et al. Preliminary incidence and trends of infections with pathogens transmitted commonly through food — Foodborne Diseases Active Surveillance Network, 10 U.S. sites, 2016–2019. MMWR Morb Mortal Wkly Rep. 2020;69(17):509–514. — Search PubMed — CDC surveillance data establishing Campylobacter as the leading bacterial cause of foodborne illness in the United States.
- Wieczorek K, Osek J. Antimicrobial resistance mechanisms among Campylobacter. Biomed Res Int. 2013;2013:340605. — Search PubMed — Review of fluoroquinolone and macrolide resistance mechanisms, explaining why ciprofloxacin is no longer reliably effective.
Connections
- Gastroenterology Conditions
- Infectious Disease
- Helicobacter pylori
- Salmonella
- Guillain-Barré Syndrome
- Inflammatory Bowel Disease
- All Conditions