N-acetyl-cysteine (NAC) as a Glutathione Precursor — the Master Mechanism
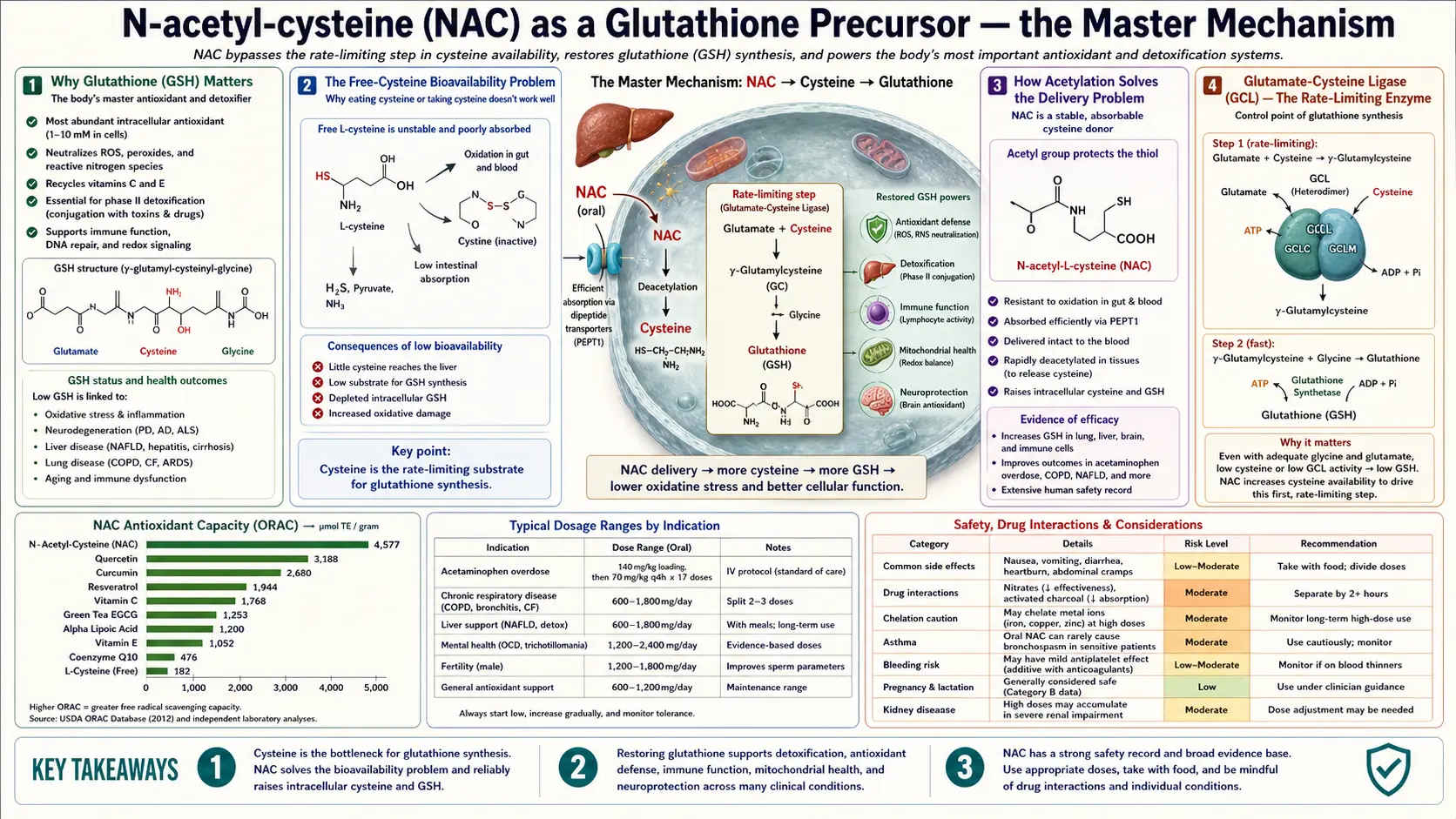
The single most important fact about N-acetylcysteine is that it is a vehicle for delivering cysteine to hepatocytes, lymphocytes, neurons, and every other cell with active glutathione synthesis. Free oral cysteine fails as a clinical strategy: gut bacteria degrade most of it, what survives is rapidly oxidized in the bloodstream to cystine, and cystine is poorly transported into many cell types. The acetyl group on NAC protects the thiol all the way through gastric acid, gut wall, and portal circulation to the hepatocyte, where intracellular deacetylation releases free cysteine inside the cell where it is needed. From there, glutamate-cysteine ligase (GCL) catalyzes the rate-limiting step of glutathione synthesis. This deep-dive explains the bioavailability paradox (NAC's plasma bioavailability is only 4–10% but the clinical effect is robust), the 1-to-4-week intracellular glutathione restoration kinetics, the GlyNAC combination work that pairs NAC with glycine for full effect, and why oral NAC outperforms direct oral glutathione despite the apparent shortcut.
Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- Why Glutathione Matters
- The Free-Cysteine Bioavailability Problem
- How Acetylation Solves the Delivery Problem
- Glutamate-Cysteine Ligase — the Rate-Limiting Enzyme
- Intracellular GSH Restoration Kinetics
- The Bioavailability Paradox
- Why Glycine Matters: GlyNAC
- The Sekhar GlyNAC Aging Trials
- NAC vs Direct Oral Glutathione
- Alternatives: Whey, Liposomal GSH, Sulforaphane, Selenium
- Measuring Glutathione Status
- Dosing for Glutathione Restoration
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Why Glutathione Matters
Glutathione (GSH) is a tripeptide of glutamate, cysteine, and glycine. It is the most abundant intracellular antioxidant by orders of magnitude — concentrations of 1–10 millimolar inside most cells, compared to micromolar concentrations for vitamin C, vitamin E, CoQ10, and the other small-molecule antioxidants. The reduced (GSH) to oxidized (GSSG) ratio is the most sensitive measure of cellular redox state in clinical chemistry. Maintaining a GSH:GSSG ratio above about 10:1 is critical for normal cellular function.
The functional roles of glutathione include:
- Direct radical scavenger — particularly hydroxyl radical, peroxynitrite, and lipid peroxyl radicals
- Substrate for glutathione peroxidase — the selenium-dependent enzyme that reduces hydrogen peroxide and lipid peroxides
- Substrate for glutathione S-transferases — Phase II detoxification enzymes that conjugate xenobiotics and electrophilic metabolites (including NAPQI from acetaminophen)
- Reductant for vitamin C and vitamin E — recycles them from oxidized to active forms, maintaining the antioxidant network
- Protein disulfide-bond homeostasis — protects cysteine residues in enzymes, transcription factors, and structural proteins
- S-glutathionylation signaling — reversible covalent modification of protein cysteines as a regulatory mechanism
Glutathione depletion is a unifying feature of most chronic disease processes. Aging, diabetes, cardiovascular disease, neurodegeneration, COPD, HIV, kidney disease, and the entire family of toxic-exposure syndromes all involve some component of intracellular GSH depletion. Restoring glutathione is therefore therapeutic across an unusually broad range — which is exactly the breadth of NAC's clinical applications.
The Free-Cysteine Bioavailability Problem
The obvious therapeutic strategy — if cysteine is the rate-limiting substrate for glutathione synthesis — would be to supplement free cysteine orally. This does not work for three reasons:
- Gut bacterial degradation. Free cysteine is an attractive sulfur substrate for many gut bacteria. A significant fraction is consumed by colonic flora before it reaches the systemic circulation, producing hydrogen sulfide and methanethiol as the breakdown products. The clinical consequence is malodorous flatus along with reduced delivery.
- Plasma oxidation to cystine. Free cysteine is highly reactive. The thiol -SH group rapidly oxidizes in oxygen-rich plasma to form the disulfide-bonded dimer cystine (Cys-S-S-Cys). Within minutes of an oral cysteine dose, most circulating cysteine in plasma is present as cystine, not the reduced thiol.
- Limited cellular uptake of cystine. Hepatocytes take up cystine through the ASC and L systems, but with substantially lower efficiency than free cysteine. Many other cell types take up cystine only through the cystine-glutamate antiporter (system xc−), which is downregulated in many disease states and which requires intracellular glutamate as the counter-ion (not always available). Free cysteine, by contrast, is taken up rapidly through the ubiquitous ASC system.
The net effect: oral free cysteine raises plasma cystine somewhat, raises intracellular cysteine only modestly, and is an unreliable strategy for glutathione restoration. Oral cysteine is also expensive because of the difficulty in preserving the reduced form during manufacturing and storage.
How Acetylation Solves the Delivery Problem
N-acetylcysteine is cysteine with an acetyl group (-CO-CH3) attached to the amino group. The structural change has three pharmacological consequences:
- Protection from gut bacterial metabolism. The acetyl group prevents the amino-acid transporter systems that gut bacteria use for free cysteine uptake. NAC passes through the gut largely intact.
- Resistance to plasma oxidation. The acetyl group sterically hinders thiol-thiol oxidation. NAC's plasma half-life as the intact molecule is longer than free cysteine's; a useful fraction reaches hepatocytes in the active reduced form.
- Intracellular deacetylation releases free cysteine where it is needed. Hepatocytes (and other cell types) express deacetylase enzymes that hydrolyze NAC to release free cysteine inside the cell — on the correct side of the plasma membrane for incorporation into glutathione synthesis. The deacetylation is essentially complete within hours.
The acetyl group is therefore a clever delivery prodrug strategy: it protects the cysteine thiol through gastric acid, gut wall, portal blood, and into the hepatocyte, then is cleaved off precisely where the free cysteine is needed. This is why NAC works clinically and free cysteine does not.
A subset of NAC also acts directly without deacetylation — the acetylated thiol can react with NAPQI (the acetaminophen toxic intermediate), with hydroxyl radicals, and with disulfide bonds in mucus. But the dominant therapeutic effect of oral NAC is via intracellular cysteine release, not via the intact NAC molecule.
Glutamate-Cysteine Ligase — the Rate-Limiting Enzyme
Glutathione synthesis is a two-step ATP-dependent process catalyzed by two enzymes in sequence:
- Glutamate-cysteine ligase (GCL, also called γ-glutamylcysteine synthetase) — joins glutamate and cysteine via a peptide bond between glutamate's gamma-carboxyl group (not the alpha-carboxyl), forming γ-glutamylcysteine. This is the rate-limiting step.
- Glutathione synthetase — adds glycine to γ-glutamylcysteine to form the complete tripeptide glutathione (γ-Glu-Cys-Gly).
GCL is the rate-limiting enzyme because (a) it is feedback-inhibited by glutathione itself (so as GSH levels rise the synthesis rate falls, providing self-regulation), and (b) its Vmax is substantially lower than glutathione synthetase's. Under most physiological conditions, the kinetic bottleneck is GCL's catalytic rate combined with cysteine availability.
Cysteine is the rate-limiting substrate for GCL because (a) glutamate is abundant intracellularly (5–10 mM in most cells), (b) glycine is abundant intracellularly (in millimolar range in liver, lower in brain and aging cells), but (c) cysteine is the rarest of the three amino acids and the most tightly regulated. The cellular cysteine pool turns over quickly because cysteine is consumed by multiple metabolic pathways (glutathione synthesis, taurine synthesis, sulfate generation, coenzyme A synthesis, hydrogen sulfide signaling).
Increasing intracellular cysteine availability — the precise effect of NAC — drives GCL activity upward toward its Vmax, accelerating glutathione synthesis. The synthesis rate is also regulated transcriptionally through Nrf2-mediated upregulation of GCL gene expression, but the acute clinical effect of NAC is the substrate-driven increase in GCL flux.
Intracellular GSH Restoration Kinetics
Starting NAC dosing in a glutathione-depleted patient produces measurable intracellular glutathione restoration over a 1-to-4-week timeline:
- Day 1–3: Plasma cysteine and cystine concentrations rise modestly. Hepatic GSH begins increasing within hours; the change is detectable by 24 hours of consistent dosing.
- Week 1: Erythrocyte GSH (a common clinical biomarker because red cells are accessible and have active GSH synthesis) is typically up 20–40% from baseline in depleted patients.
- Week 2–3: Lymphocyte and neutrophil GSH approach normal ranges. Functional measures of immune oxidative burst improve.
- Week 4: Most cellular compartments have restored their GSH pools to near-baseline. Tissue-specific compartments with slow GSH turnover (e.g., neurons) take somewhat longer.
- Discontinuation: Once NAC is stopped, intracellular GSH returns toward the patient's baseline (which may be subnormal due to underlying disease or aging) over a similar 1-to-4-week timeline.
This timeline explains why NAC clinical trials in chronic disease typically need 8–24 weeks to assess full effect — the upstream biochemical restoration (1–4 weeks) is followed by downstream functional improvement (additional weeks-to-months as cells repair, inflammation subsides, and tissue function normalizes).
The Bioavailability Paradox
A classic objection to oral NAC is its low oral bioavailability of the intact molecule — only 4–10% reaches systemic circulation as NAC itself. Critics argue this means oral NAC cannot work.
The objection misunderstands NAC's mechanism. The clinically active species is intracellular free cysteine, not the intact NAC molecule. The intact NAC has already done much of its work by the time it reaches systemic plasma:
- A large fraction is taken up first-pass by hepatocytes (the highest-priority target tissue for glutathione restoration)
- Inside hepatocytes, NAC is deacetylated to free cysteine and incorporated into hepatic glutathione — this is exactly the desired effect
- Some NAC is converted in the gut and portal blood to free cysteine, which then enters the cysteine pool
- The intact NAC that does reach systemic plasma is taken up by peripheral tissues (lymphocytes, neurons, kidney, lung) and deacetylated locally
The "low bioavailability" is therefore a misleading metric — it tells us that NAC is efficiently extracted and used, not that NAC is failing. The clinical proof is the well-documented rise in intracellular glutathione, the established efficacy in acetaminophen overdose, the PANTHEON COPD result, and the psychiatric trial outcomes.
Newer NAC analogs — NACET (N-acetylcysteine ethyl ester) and NACA (N-acetylcysteine amide) — have higher cell-penetration kinetics and may show advantages for certain indications (particularly brain penetration). NACA in particular has shown promise in preclinical models of neurodegeneration. These analogs are not yet widely available commercially.
Why Glycine Matters: GlyNAC
Cysteine is the most-discussed rate-limiting substrate for glutathione synthesis, but glycine is the second potentially limiting factor — particularly in aging cells, where intracellular glycine concentrations decline measurably.
The glycine concentration in liver and other tissues is typically high enough to support glutathione synthesis when cysteine is plentiful. But the GSH synthetase reaction (the second step, adding glycine to γ-glutamylcysteine) has its own kinetics, and in glycine-depleted cells the reaction can become co-limiting. Older adults, vegetarians with limited collagen-protein intake, and patients with chronic catabolic states often have reduced intracellular glycine.
The clinical implication: pairing NAC with glycine supplementation produces greater glutathione restoration than NAC alone. This is the basis for the "GlyNAC" protocol developed by Rajagopal Sekhar at Baylor College of Medicine.
The typical GlyNAC ratio is approximately 1.3 g cysteine equivalent (1 g NAC, since NAC is ~80% cysteine by weight) plus 1.3 g glycine, daily. Both amino acids are inexpensive and well-tolerated.
For the broader story of glycine, see the Glycine page. For the Sekhar aging trials, the deep-dive at Antioxidants/Glutathione/Benefits/Aging-and-GlyNAC.html (when added) will provide the full clinical detail.
The Sekhar GlyNAC Aging Trials
Rajagopal Sekhar's group at Baylor College of Medicine has produced the most influential modern work on glutathione restoration in aging. The conceptual framing: older adults have measurably reduced intracellular glutathione, with the deficit driven by both reduced cysteine availability and reduced glycine availability. Sekhar's hypothesis is that restoring both substrates simultaneously could reverse not just the glutathione deficit but the downstream consequences (mitochondrial dysfunction, insulin resistance, inflammation, oxidative stress, cognitive decline).
The Sekhar 2021 trial (Clinical and Translational Medicine) randomized older adults (mean age 71) to GlyNAC supplementation versus placebo for 16 weeks. Substrates: 100 mg/kg/day each of glycine and N-acetylcysteine (roughly 7 g of each per day for a 70 kg adult). Results:
- Red blood cell glutathione restored to levels seen in young adults (versus persistent deficit in placebo)
- Mitochondrial dysfunction biomarkers improved — including PGC-1α expression and fatty acid oxidation
- Insulin resistance reduced (HOMA-IR improvement)
- Inflammatory cytokines decreased (TNF-α, IL-6, C-reactive protein)
- Cognitive function improved on multiple measures
- Body composition changed favorably — reduced waist circumference, improved lean-mass-to-fat-mass ratio
- Gait speed and grip strength improved — both validated frailty markers
The trial was small (24 participants) but the effect size across multiple outcomes was striking. A larger replication trial is in progress. If the findings hold up at scale, GlyNAC could become a foundational longevity-medicine intervention — cheap, well-tolerated, and addressing a fundamental aging mechanism (glutathione depletion) rather than a downstream symptom.
Earlier Sekhar work (2011, 2014) in HIV patients showed similar restoration of glutathione status and improvement in mitochondrial markers using a similar GlyNAC protocol, establishing that the glutathione-precursor strategy works in clinically depleted populations beyond just normal aging.
NAC vs Direct Oral Glutathione
An apparently obvious alternative to NAC is to supplement glutathione directly. The reasoning seems straightforward: if glutathione is what we want, why go through the cysteine intermediate?
The answer is bioavailability. Free oral glutathione faces the same problems as free oral cysteine, plus additional ones:
- Gut peptidase degradation — glutathione is a tripeptide. Brush-border peptidases (γ-glutamyl transferase) cleave it into its constituent amino acids before absorption.
- Limited intact uptake — some intact glutathione is absorbed in the small intestine, but the fraction is small.
- Limited cellular uptake of intact glutathione from plasma — most cells re-synthesize glutathione intracellularly rather than importing it from plasma. Hepatocytes do export glutathione to plasma, but reverse uptake is inefficient.
A direct comparison of oral glutathione vs NAC for raising intracellular glutathione has consistently shown NAC at least as effective — often more so — at much lower cost. The Allen 2011 trial of oral GSH (500 mg twice daily) for 4 weeks failed to raise blood glutathione markers, while NAC trials at similar molar doses reliably do.
Liposomal glutathione preparations (glutathione encapsulated in phospholipid vesicles) have improved bioavailability compared to free glutathione, but the clinical evidence for superiority over NAC is thin. Liposomal GSH is also substantially more expensive than NAC. The Sinha 2018 trial of liposomal glutathione showed modest improvements in oxidative stress markers, but no head-to-head comparison with NAC has shown clear superiority.
The clinical take: oral NAC is the most cost-effective, evidence-supported glutathione-restoration strategy for most patients. Liposomal glutathione is a reasonable second-line for patients who do not tolerate NAC or who want additional glutathione delivery.
Alternatives: Whey, Liposomal GSH, Sulforaphane, Selenium
- Whey protein — particularly the α-lactalbumin fraction — is unusually high in cysteine bound within the intact protein structure. Cysteine residues delivered as protein-bound are protected from gut bacterial degradation. Several trials have shown whey protein supplementation raises intracellular glutathione. Practical use: 20–30 g/day of high-quality whey protein concentrate or isolate.
- Sulforaphane — the isothiocyanate from cruciferous vegetables (broccoli sprouts contain the highest concentrations) activates Nrf2, which transcriptionally upregulates GCL and many other antioxidant genes. Sulforaphane increases glutathione synthesis capacity rather than directly providing substrate. Pairs well with NAC. See the relevant pages on sulforaphane and Nrf2 activation.
- Selenium — essential cofactor for glutathione peroxidase (the selenium-dependent enzyme that uses GSH to reduce hydrogen peroxide and lipid peroxides). Selenium deficiency limits GSH function even when GSH itself is adequate. Selenium and glutathione/NAC are complementary; ensure adequate selenium intake (~200 mcg/day from food or supplement) for full glutathione system function.
- Alpha lipoic acid — recycles oxidized glutathione back to the reduced active form. ALA + NAC is a synergistic combination for oxidative stress reduction. See Alpha Lipoic Acid.
- Vitamin C — protects the cysteine thiol from oxidation and supports the cellular redox cycle that maintains GSH:GSSG ratio. Adequate vitamin C (500–1,000 mg/day) supports any glutathione-restoration strategy.
The most efficient glutathione-restoration protocol for a typical patient combines NAC 600 mg twice daily, glycine 1–3 g/day (for the GlyNAC effect), selenium 200 mcg/day, and adequate dietary protein (especially cysteine-rich proteins like whey and eggs). For aggressive restoration in severely depleted patients, add alpha lipoic acid 300–600 mg/day.
Measuring Glutathione Status
Clinical labs offer several glutathione-related measurements with varying utility:
- Whole blood / erythrocyte glutathione — the most practical and reproducible measurement. Reflects body-wide GSH status. Normal range varies by lab but is approximately 800–1,300 μmol/L in whole blood.
- Plasma GSH — lower concentrations, less stable, not typically clinically useful.
- GSH:GSSG ratio — the most informative single measurement of oxidative stress. A ratio above 10:1 is normal; below 5:1 indicates significant oxidative stress.
- Urinary 8-OHdG (8-hydroxy-2'-deoxyguanosine) — an indirect marker of oxidative DNA damage that correlates with low GSH status.
- F2-isoprostanes — lipid peroxidation marker, also an indirect indicator of glutathione system function.
For most patients, measuring glutathione status is not necessary before starting NAC — the safety profile is favorable, the cost is low, and the indications (any condition with significant oxidative stress contribution) are common enough that empiric use is reasonable. Measurement becomes more useful for research applications, for monitoring response in patients with severe depletion (HIV, chronic kidney disease), and for documenting effect in longevity-medicine contexts.
Dosing for Glutathione Restoration
- General antioxidant / longevity support: NAC 600 mg twice daily (1,200 mg total). Add glycine 1–2 g once daily.
- Aggressive restoration in documented depletion: NAC 900 mg three times daily (2,700 mg total) plus glycine 3 g/day, for 8–12 weeks, then taper to maintenance.
- Sekhar GlyNAC aging protocol: 100 mg/kg/day each of NAC and glycine for 16 weeks. For a 70 kg adult: 7 g NAC + 7 g glycine daily, divided into 2–3 doses.
- Maintenance after restoration: 600 mg NAC twice daily plus 1–2 g glycine daily, indefinitely. The glutathione pool will return toward the patient's baseline within weeks of discontinuation.
- Take with or without food. NAC absorption is not significantly affected by food. Take with adequate water (8 oz) and consider taking with breakfast and dinner for simple compliance.
- Effervescent or solution forms are often better tolerated than capsules. The capsule preparations carry a sulfurous odor when opened; the effervescent tablets dissolved in juice or water mask this.
Cautions
- Sulfur breath and odor — common and harmless but socially noticeable. Effervescent forms with juice masking are better tolerated.
- GI upset — nausea, indigestion, diarrhea are common at higher doses. Start at half the target dose for a week and titrate up.
- Drug interactions — the nitroglycerin interaction (potentiated vasodilation, possible hypotension) is the most clinically significant. See Cardiovascular Health.
- Activated charcoal — adsorbs NAC in the gut. If both are being given (rare scenario), separate doses by at least 2 hours.
- Pregnancy: Category B. The acetaminophen-overdose literature has established NAC's safety in pregnancy at very high IV doses. Standard oral supplementation in pregnancy is reasonable when clinically indicated.
- Caution in active asthma — only relevant for inhaled/nebulized NAC, not for oral. Oral NAC is safe in asthma at standard doses.
- Glutathione is not always good in excess. Some cancers (notably platinum-resistant ovarian, drug-resistant melanoma) maintain high intracellular glutathione as a chemoresistance mechanism. NAC supplementation in active cancer treatment should be discussed with the oncologist.
Key Research Papers
- Kumar P et al. (2021). Supplementing glycine and N-acetylcysteine (GlyNAC) in older adults improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, physical function, and aging hallmarks. Clinical and Translational Medicine. — PubMed
- Nguyen D et al. (2014). Effect of increasing glutathione with cysteine and glycine supplementation on mitochondrial fuel oxidation, insulin sensitivity, and body composition in older HIV-infected patients. Journal of Clinical Endocrinology & Metabolism. — PubMed
- Atkuri KR et al. (2007). N-acetylcysteine — a safe antidote for cysteine/glutathione deficiency. Current Opinion in Pharmacology. — PubMed
- Herzenberg LA et al. (1997). Glutathione deficiency is associated with impaired survival in HIV disease. PNAS. — PubMed
- Lu SC (2013). Glutathione synthesis. Biochimica et Biophysica Acta. — PubMed
- Dilger RN, Baker DH (2007). Oral N-acetylcysteine raises whole-blood glutathione in adults. American Journal of Clinical Nutrition. — PubMed
- Allen J, Bradley RD (2011). Effects of oral glutathione supplementation on systemic oxidative stress biomarkers in human volunteers. Journal of Alternative and Complementary Medicine. — PubMed
- Sinha R et al. (2018). Oral supplementation with liposomal glutathione elevates body stores of glutathione and markers of immune function. European Journal of Clinical Nutrition. — PubMed
- Bumrungpert A et al. (2018). Whey protein supplementation improves nutritional status, glutathione levels, and immune function in cancer patients. Journal of Medicinal Food. — PubMed
- Houghton CA et al. (2016). Sulforaphane and other nutrigenomic Nrf2 activators: can the clinician's expectation be matched by the reality? Oxidative Medicine and Cellular Longevity. — PubMed
PubMed Topic Searches
- PubMed: NAC glutathione precursor
- PubMed: GlyNAC glycine + cysteine
- PubMed: cysteine bioavailability
- PubMed: GCL rate-limiting enzyme
- PubMed: liposomal glutathione
- PubMed: whey protein glutathione
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- NAC Overview
- NAC Benefits Hub
- NAC as Acetaminophen Antidote
- NAC for COPD & Lung
- NAC for Mental Health
- NAC & Glutathione (Overview)
- Glutathione (Master Antioxidant)
- Glutathione & GlyNAC for Aging
- Alpha Lipoic Acid
- CoQ10
- All Antioxidants
- Cysteine
- Glycine
- Selenium
- Vitamin C
- Liver Cleansing
- Detox Protocols
- Oxidative Stress
- Longevity Protocols