N-acetyl-cysteine (NAC) for COPD & Lung Health
NAC has been used as an inhaled mucolytic since 1963 and as an oral mucolytic across Europe for over fifty years. The 21st-century PANTHEON trial (Zheng 2014) established that 600 mg twice daily for one year reduced acute exacerbations by 22% in moderate-to-severe COPD — an effect size comparable to long-acting bronchodilators in selected patients. This deep-dive walks through the three lung-relevant NAC mechanisms (disulfide cleavage, bronchial-epithelial glutathione restoration, ROS scavenging), the PANTHEON, BRONCUS, HIACE, IFIGENIA, and PANTHER-IPF trials, the COPD vs chronic bronchitis vs cystic fibrosis vs bronchiectasis vs IPF nuances, oral vs nebulized routes, and the asthma bronchospasm caution that matters most clinically.
Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- Three Lung Mechanisms in One Molecule
- Mucolytic Mechanism — Disulfide Bond Cleavage
- Bronchial-Epithelial Glutathione Replenishment
- ROS Scavenging in the Airway
- PANTHEON — the Definitive COPD Trial
- BRONCUS and HIACE
- Chronic Bronchitis and Mucus Hypersecretion
- Cystic Fibrosis
- Idiopathic Pulmonary Fibrosis (IFIGENIA vs PANTHER-IPF)
- Bronchiectasis
- Oral vs Nebulized Routes
- Asthma Bronchospasm Caution
- Dosing Protocols by Indication
- Cautions
- Key Research Papers
- Connections
- Featured Videos
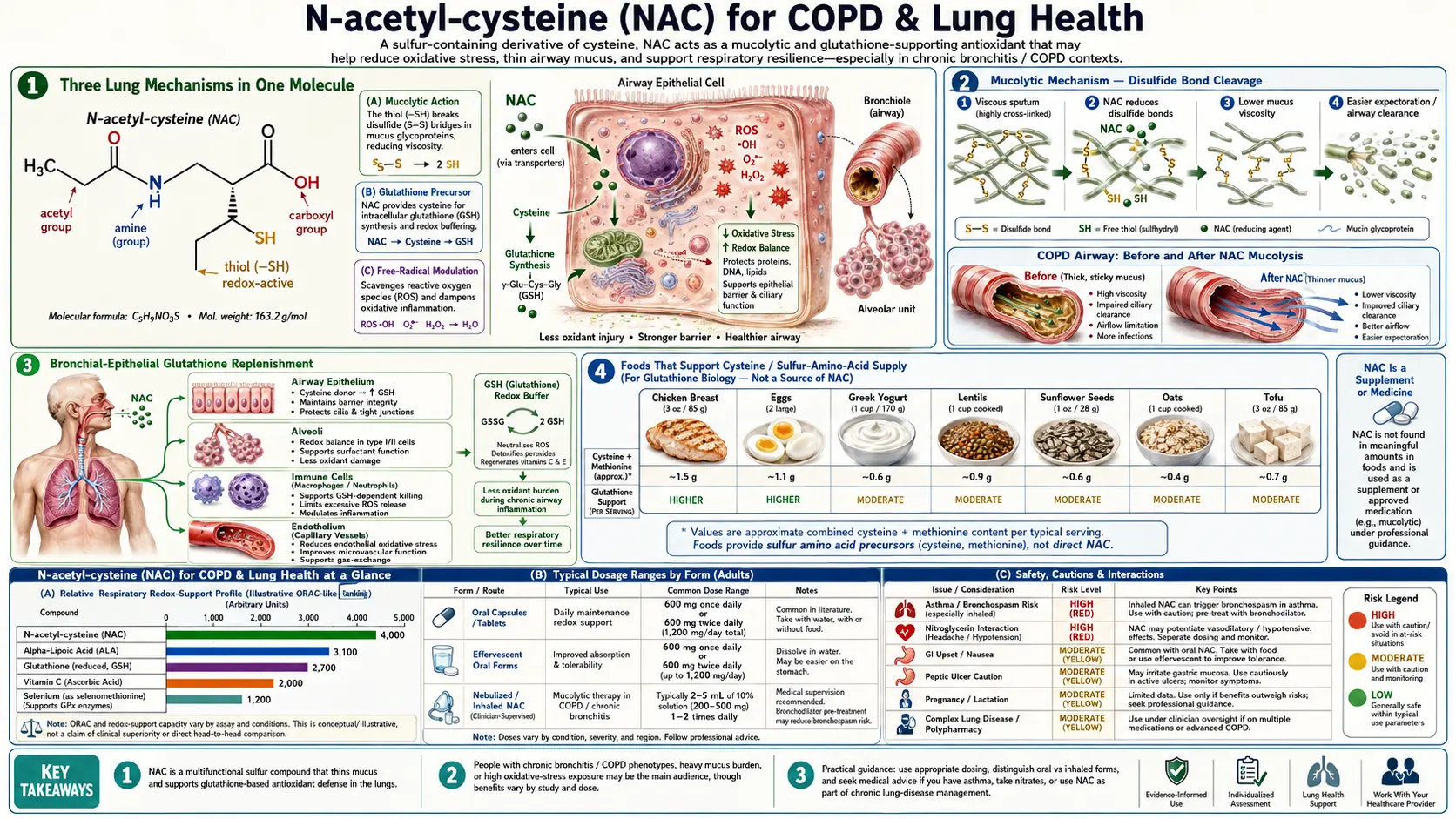
Three Lung Mechanisms in One Molecule
NAC produces clinical benefit in airway disease through three mechanisms that operate in parallel, each contributing meaningfully to the overall effect:
- Mucolytic disulfide cleavage — the original 1963 Mucomyst indication. The free thiol on NAC reduces disulfide bonds in mucin glycoproteins, which collapses the mucus gel structure and reduces sputum viscosity.
- Bronchial-epithelial glutathione restoration — the bronchial epithelium maintains a glutathione concentration in its airway-lining fluid that is approximately 100-fold higher than plasma, reflecting the oxidative load from inhaled tobacco smoke, pollution, and pathogens. Chronic insult depletes this pool; NAC restores it.
- Direct ROS scavenging — particularly relevant in acute exacerbations when neutrophil influx generates large quantities of hypochlorous acid, hydroxyl radical, and peroxynitrite that overwhelm even a healthy glutathione system.
Importantly, no single one of these mechanisms fully explains the PANTHEON or BRONCUS findings. The 22% exacerbation reduction in PANTHEON probably reflects the simultaneous action of all three: improved mucus clearance during stable disease, restored antioxidant defense during the chronic oxidative stress of smoking-related lung damage, and direct radical scavenging during the inflammatory burst that defines an exacerbation.
Mucolytic Mechanism — Disulfide Bond Cleavage
Mucus in the airway is a gel composed primarily of mucin glycoproteins. Mucins are large polypeptides whose three-dimensional structure is held together by disulfide bonds between cysteine residues. The disulfide cross-links make mucin chains entangle into a viscoelastic gel that traps inhaled particles for mucociliary clearance.
In healthy airways, the mucus gel is appropriately viscous — thick enough to trap particles, thin enough for cilia to move it upward toward the pharynx. In chronic bronchitis, COPD, and cystic fibrosis, the mucus becomes pathologically thick and tenacious because of three things: hypersecretion (too much mucus), abnormal mucin composition (more cross-linkable cysteine residues), and dehydration (water loss from the gel, particularly in cystic fibrosis where chloride channel dysfunction prevents water from following sodium into the airway-lining fluid).
NAC's free thiol attacks the disulfide bonds in mucin glycoproteins, reducing them to free thiols. The cross-links break. The mucin chains can no longer maintain the gel network. Mucus viscosity drops by roughly 50% within minutes of NAC contact in vitro, and sputum viscosity drops measurably within hours in patients treated with oral or inhaled NAC.
The clinical implications: easier sputum expectoration, reduced cough productivity, improved mucociliary clearance, and reduced infectious load (because trapped bacteria are cleared rather than sitting in stagnant mucus). This is the mechanism behind the historical role of NAC as a "chest medicine" across European primary care.
Bronchial-Epithelial Glutathione Replenishment
The bronchial epithelium maintains an extraordinarily high glutathione concentration in its airway-lining fluid — on the order of 400 μM, compared to 5–10 μM in plasma. Cantin et al. (1989) demonstrated this concentration gradient by bronchoalveolar lavage in healthy subjects, and showed that it falls measurably in smokers, COPD patients, and patients with cystic fibrosis.
The high airway GSH concentration exists for a reason: every breath delivers oxidants. Ambient air contains nitrogen oxides, ozone, particulate matter, and (in smokers) a chemical cocktail that includes hydrogen peroxide, free radicals, and reactive aldehydes. The airway-lining fluid is the first line of antioxidant defense, and glutathione is its principal antioxidant.
Chronic oxidative stress depletes this airway GSH pool. NAC restores it — oral NAC raises bronchial-epithelial-lining fluid glutathione concentrations measurably within days of starting consistent dosing, and the restoration correlates with reduced markers of oxidative damage in sputum and exhaled breath condensate.
The clinical significance: chronic smokers and COPD patients live in a state of ongoing airway oxidative stress that drives mucus hypersecretion, mucociliary dysfunction, and the inflammatory cascade that produces exacerbations. Restoring the airway GSH pool addresses the upstream driver, not just the downstream symptoms.
ROS Scavenging in the Airway
During a COPD exacerbation, neutrophil influx into the airway generates a burst of reactive oxygen species that includes hypochlorous acid (from myeloperoxidase), superoxide (from NADPH oxidase), and hydroxyl radical (from iron-catalyzed Fenton chemistry). The oxidative burst is the proximate cause of much of the symptomatic worsening: it activates inflammatory transcription, damages bronchial epithelium, and increases mucus viscosity by oxidatively modifying mucin proteins.
NAC's free thiol directly scavenges these radicals independent of the glutathione system. The thiol-radical reaction kinetics are fast, particularly for hypochlorous acid (rate constant on the order of 107–108 M-1s-1). At the relatively high concentrations of NAC reached in airway tissue after oral dosing, meaningful direct radical scavenging occurs.
This mechanism is why NAC produces effect during exacerbations themselves, not just in stable disease — the airway oxidative burst is being directly buffered while the glutathione system is being replenished in parallel.
PANTHEON — the Definitive COPD Trial
The PANTHEON trial (Zheng et al., Lancet Respiratory Medicine, 2014) is the largest and most rigorous trial of NAC in COPD. 1,006 patients with moderate-to-severe COPD (post-bronchodilator FEV1 30–70% predicted) randomized to NAC 600 mg twice daily or placebo for one year. Primary outcome: rate of acute exacerbations over the treatment year.
Results:
- 22% reduction in exacerbation rate — 1.16 exacerbations per patient-year on NAC versus 1.49 on placebo (rate ratio 0.78, 95% CI 0.67–0.90; p=0.0011)
- Benefit was most pronounced in the GOLD II/III moderate-to-severe subgroup
- Time to first exacerbation was prolonged
- No significant difference in lung function (FEV1) over the trial year — NAC's effect is on exacerbation frequency, not the underlying rate of lung function decline
- Adverse event profile was similar between NAC and placebo, with mild GI symptoms slightly more frequent on NAC
PANTHEON established 600 mg twice daily as the evidence-based dose for COPD — not 600 mg once daily, which was the dose used in some earlier negative trials. The higher dosing was important enough to flip the meta-analytic picture: pre-PANTHEON meta-analyses had shown only marginal benefit; post-PANTHEON, the picture is consistent and clinically meaningful.
The clinical implication: any patient with GOLD II/III/IV COPD who is willing to take a twice-daily oral medication should be offered NAC 600 mg BID as an adjunct to inhaled bronchodilators and inhaled steroids. The number needed to treat to prevent one additional exacerbation per patient-year is approximately 3 over a one-year treatment period.
BRONCUS and HIACE
BRONCUS (Decramer 2005)
BRONCUS (Bronchitis Randomized On NAC Cost-Utility Study) randomized 523 COPD patients to NAC 600 mg once daily versus placebo for 3 years. The primary outcome (rate of FEV1 decline) was not different between groups; secondary outcomes (exacerbation rate) showed modest benefit only in patients not taking inhaled corticosteroids.
BRONCUS was the trial that initially cast doubt on routine NAC use in COPD. In retrospect, the limitations are clear:
- The 600 mg once daily dose was too low — PANTHEON later showed that 600 mg twice daily is the effective dose
- The primary outcome (FEV1 decline) is not what NAC affects; exacerbation rate is
- Inhaled corticosteroids appear to mask the NAC effect by addressing some of the same inflammatory pathways
HIACE (Tse 2013)
HIACE (High-dose Acetylcysteine in COPD Exacerbation) tested NAC 600 mg twice daily versus placebo in 120 Chinese COPD patients over one year. Results: 41% reduction in exacerbation rate in the NAC group, plus modest improvements in small-airway function. HIACE was the proof-of-concept for the dose used in PANTHEON.
Chronic Bronchitis and Mucus Hypersecretion
The 2019 Cochrane meta-analysis (Poole, Sathananthan, Fortescue) pooled 41 randomized trials of mucolytics in chronic bronchitis and COPD. Across mucolytic agents (NAC, ambroxol, erdosteine, carbocisteine), the meta-analysis showed:
- Reduction in monthly exacerbation rate of approximately 0.04 per month (roughly half an exacerbation per year)
- Reduction in days of illness per month
- Reduction in days requiring antibiotics
- The benefit was larger in patients not on inhaled corticosteroids, smaller (but still present) in those who were
For chronic bronchitis specifically (productive cough on most days for 3 months in 2 consecutive years), NAC's mucolytic action provides symptomatic benefit: easier sputum clearance, reduced cough frequency, and improved quality of life measures even when exacerbation rates are modestly affected.
Across European primary care, oral NAC has been prescribed for decades for chronic productive cough at doses of 200–600 mg one to three times daily. The clinical impression is that the regimen works; the cleanest randomized evidence is for the 600 mg BID dose in COPD specifically.
Cystic Fibrosis
Cystic fibrosis produces airway mucus that is particularly thick, dehydrated, and tenacious because the underlying CFTR chloride channel dysfunction prevents proper hydration of the airway-lining fluid. The disulfide-rich mucin gel becomes extraordinarily difficult to clear, leading to mucus plugging, bacterial colonization (especially Pseudomonas aeruginosa and Staphylococcus aureus), and progressive bronchiectasis.
NAC has been studied in CF for decades. Inhaled NAC (nebulized) has documented mucolytic effect but has been largely supplanted by dornase alfa (DNase) which targets the neutrophil-derived DNA component of CF mucus, and by hypertonic saline which addresses the hydration problem. Oral NAC at high doses (700 mg three times daily) has been studied for its glutathione-restoring properties — CF patients are known to have low airway and systemic glutathione concentrations, and the Tirouvanziam trial showed restoration of neutrophil glutathione with high-dose oral NAC.
Current CF practice typically does not include routine NAC as a first-line agent (CFTR modulators like elexacaftor-tezacaftor-ivacaftor have transformed the picture for most genotypes), but NAC remains a reasonable adjunct in patients with persistent mucus issues or low glutathione status.
Idiopathic Pulmonary Fibrosis (IFIGENIA vs PANTHER-IPF)
The IPF story is one of the most instructive in NAC clinical research because it shows how a positive trial can be overturned by a larger, better-controlled successor trial.
IFIGENIA (Demedts 2005, NEJM)
The IFIGENIA trial randomized 182 IPF patients to triple therapy with prednisone + azathioprine + NAC (600 mg three times daily) or prednisone + azathioprine + placebo. The NAC group showed less decline in vital capacity and DLCO at one year. This led to NAC's adoption as part of the standard IPF triple-therapy regimen for the better part of a decade.
PANTHER-IPF (Raghu 2014)
PANTHER-IPF was designed as the definitive three-arm comparison: triple therapy (prednisone + azathioprine + NAC) versus NAC alone versus placebo. Results were dramatic:
- The triple-therapy arm was stopped early because of harm — increased mortality, hospitalizations, and serious adverse events compared to placebo
- The NAC-alone arm showed no significant benefit over placebo on the primary outcome (vital capacity decline)
- NAC alone was not harmful — just not helpful in this population
PANTHER-IPF rewrote IPF guidelines worldwide. Triple therapy was abandoned (the azathioprine+prednisone combination was the proximate harm). NAC monotherapy is no longer routinely recommended for IPF, although it remains an option for selected patients with predominantly oxidative-stress phenotypes. The current first-line IPF drugs are pirfenidone and nintedanib, both anti-fibrotic agents.
The lesson is broader than IPF: positive trials need replication, and the addition of a marginal agent to a harmful background therapy can obscure both effects.
Bronchiectasis
Non-CF bronchiectasis is characterized by dilated airways, chronic mucus retention, and recurrent infection. The BENE trial and several smaller studies have tested NAC in this population. Findings: NAC reduces sputum viscosity, improves clearance, and modestly reduces exacerbation rate. Doses studied are typically 600 mg twice daily, mirroring the COPD evidence.
In modern bronchiectasis practice, airway clearance techniques (active cycle of breathing, oscillatory PEP devices), hypertonic saline nebulization, and inhaled antibiotics for chronic Pseudomonas colonization are the mainstays. NAC is a reasonable oral adjunct, particularly in patients with viscous sputum that is hard to clear.
Oral vs Nebulized Routes
| Property | Oral NAC | Nebulized NAC (Mucomyst) |
|---|---|---|
| Site of action | Systemic + bronchial via blood | Direct airway luminal contact |
| Onset of mucolytic effect | Hours to days | Minutes |
| Systemic glutathione restoration | Yes, robust | Minimal |
| Convenience | High — oral capsule or effervescent tablet | Low — nebulizer required |
| Bronchospasm risk | Minimal | Real — pre-treat with bronchodilator in asthmatics |
| Best for | Stable COPD, chronic bronchitis, long-term maintenance | Acute mucus plugging, ICU airway management, CF exacerbation adjunct |
For the typical outpatient with COPD or chronic bronchitis, oral NAC 600 mg BID is the default. Nebulized NAC is used in inpatient and ICU settings for acute mucus retention — particularly in intubated patients where mucus plugging of an endotracheal tube can rapidly become life-threatening.
Asthma Bronchospasm Caution
Inhaled or nebulized NAC can provoke bronchospasm in asthmatic and hyperreactive airways. The mechanism is direct airway smooth-muscle irritation by the sulfhydryl compound, particularly at the typical nebulized concentration of 10–20%. Patients with known asthma, COPD with bronchospastic component, or hyperreactive airways should be pre-treated with an inhaled short-acting bronchodilator (albuterol 90 mcg, 2 puffs) 5–10 minutes before nebulized NAC.
Oral NAC does not cause bronchospasm because the systemic concentration is far below what produces airway smooth-muscle irritation. Patients with asthma can safely take oral NAC at standard doses.
For COPD patients with an asthmatic phenotype (overlap syndrome, eosinophilic COPD), oral NAC remains appropriate. The PANTHEON trial included patients with bronchodilator response and did not exclude asthma-COPD overlap; no safety signal emerged.
Dosing Protocols by Indication
- Stable moderate-to-severe COPD (PANTHEON dose): 600 mg orally twice daily indefinitely. Take with or without food. Expect benefit over 6–12 months of consistent use; exacerbation reduction is the primary measurable outcome.
- Chronic bronchitis with productive cough: 600 mg orally one to two times daily. Some European protocols use 200 mg three times daily. Effect on cough productivity within 1–2 weeks.
- COPD exacerbation adjunct: 600 mg orally twice daily continued through and beyond the exacerbation. Does not replace bronchodilators, corticosteroids, or antibiotics; supplements them.
- Cystic fibrosis (oral GSH restoration): 700 mg three times daily in adults (Tirouvanziam protocol). Adjunctive only — not a substitute for CFTR modulators or airway clearance.
- Bronchiectasis: 600 mg twice daily, similar to the COPD protocol. Combined with airway clearance techniques.
- Nebulized for inpatient mucus plugging: 3–5 mL of 10% or 20% solution nebulized every 6–8 hours. Pre-treat with bronchodilator.
- Idiopathic pulmonary fibrosis: No longer routinely recommended after PANTHER-IPF. Selected patients with predominantly oxidative-stress phenotypes may still benefit at 600 mg TID, but pirfenidone or nintedanib are first-line.
Cautions
- Pre-treat asthmatics with bronchodilator before nebulized NAC. Bronchospasm risk is real and can be severe.
- The PANTHEON dose is 600 mg twice daily. Once-daily dosing (as in BRONCUS) is sub-therapeutic for exacerbation prevention.
- NAC is an adjunct, not a substitute for bronchodilators or inhaled steroids. Continue inhaled LABA/LAMA and ICS as prescribed.
- Sulfurous breath odor is the most common practical complaint — not dangerous, but bothersome enough that effervescent tablets dissolved in juice are often better tolerated than capsules.
- Patients on chronic nitrates — NAC potentiates nitrate-induced vasodilation. The combination is not contraindicated but the patient should be aware of possible enhanced hypotension. See the Cardiovascular Health page.
- This is not COVID-related. NAC's lung benefits are firmly grounded in COPD, chronic bronchitis, and pulmonary fibrosis evidence dating back decades. Discussion of acute respiratory infection management here covers the De Flora 1997 influenza prophylaxis trial and the chronic-bronchitis exacerbation reduction literature only.
Key Research Papers
- Zheng JP et al. (2014). Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respiratory Medicine. — PubMed
- Decramer M et al. (2005). Effects of N-acetylcysteine on outcomes in chronic obstructive pulmonary disease (Bronchitis Randomized on NAC Cost-Utility Study, BRONCUS): a randomised placebo-controlled trial. Lancet. — PubMed
- Tse HN et al. (2013). High-dose N-acetylcysteine in stable COPD: the 1-year, double-blind, randomized, placebo-controlled HIACE study. Chest. — PubMed
- Poole P et al. (2019). Mucolytic agents versus placebo for chronic bronchitis or chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews. — PubMed
- Demedts M et al. (2005). High-dose acetylcysteine in idiopathic pulmonary fibrosis (IFIGENIA). New England Journal of Medicine. — PubMed
- Raghu G et al. (2014). Randomized trial of acetylcysteine in idiopathic pulmonary fibrosis (PANTHER-IPF). New England Journal of Medicine. — PubMed
- Cantin AM et al. (1989). Glutathione deficiency in the epithelial lining fluid of the lower respiratory tract in idiopathic pulmonary fibrosis. American Review of Respiratory Disease. — PubMed
- De Flora S et al. (1997). Attenuation of influenza-like symptomatology and improvement of cell-mediated immunity with long-term N-acetylcysteine treatment. European Respiratory Journal. — PubMed
- Tirouvanziam R et al. (2006). High-dose oral N-acetylcysteine, a glutathione prodrug, modulates inflammation in cystic fibrosis. PNAS. — PubMed
- Calzetta L et al. (2018). N-acetylcysteine in COPD: why, how, and when? Multidisciplinary Respiratory Medicine. — PubMed
PubMed Topic Searches
- PubMed: NAC and COPD
- PubMed: NAC and chronic bronchitis
- PubMed: NAC and cystic fibrosis
- PubMed: NAC and pulmonary fibrosis
- PubMed: NAC and bronchiectasis
- PubMed: NAC mucolytic mechanism
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- NAC Overview
- NAC Benefits Hub
- NAC as Acetaminophen Antidote
- NAC for Mental Health
- NAC as Glutathione Precursor
- NAC & Respiratory Health (Overview)
- Glutathione
- COPD
- Pulmonology Overview
- Oxidative Stress
- Detox Protocols
- Cysteine
- Glycine
- All Toxins
- All Antioxidants