N-acetyl-cysteine (NAC) for Mental Health: OCD, Trichotillomania & Beyond
NAC is one of the most surprising stories in modern psychiatry. The same molecule used as an inhaled mucolytic since 1963 and as the acetaminophen antidote since 1979 has, over the past two decades, accumulated randomized controlled trial evidence in trichotillomania, obsessive-compulsive disorder, bipolar depression, schizophrenia, autism spectrum irritability, and substance-use disorders. The unifying mechanism is glutamate homeostasis through the cystine-glutamate antiporter (system xc−) in prefrontal cortex and nucleus accumbens, layered on top of the broader antioxidant and anti-inflammatory effects that matter in essentially every major psychiatric disorder. This deep-dive walks through the Grant 2009 trichotillomania trial that launched the field, the Afshar 2012 OCD augmentation data, the Berk bipolar and schizophrenia trials, and the underlying neurobiology that explains why a simple sulfur amino acid derivative reaches places SSRIs do not.
Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- Why a Sulfur Amino Acid Reaches Psychiatric Targets
- The Glutamate-Homeostasis Mechanism
- Trichotillomania — the Field-Defining Indication
- Obsessive-Compulsive Disorder (OCD)
- Skin Picking (Excoriation) and Nail Biting
- Bipolar Depression
- Schizophrenia and Negative Symptoms
- Autism Spectrum Disorder Irritability
- Cocaine, Cannabis, Nicotine, Gambling
- PTSD with Substance Use
- Practical Timeline of Psychiatric Response
- Dosing by Indication
- Cautions
- Key Research Papers
- Connections
- Featured Videos
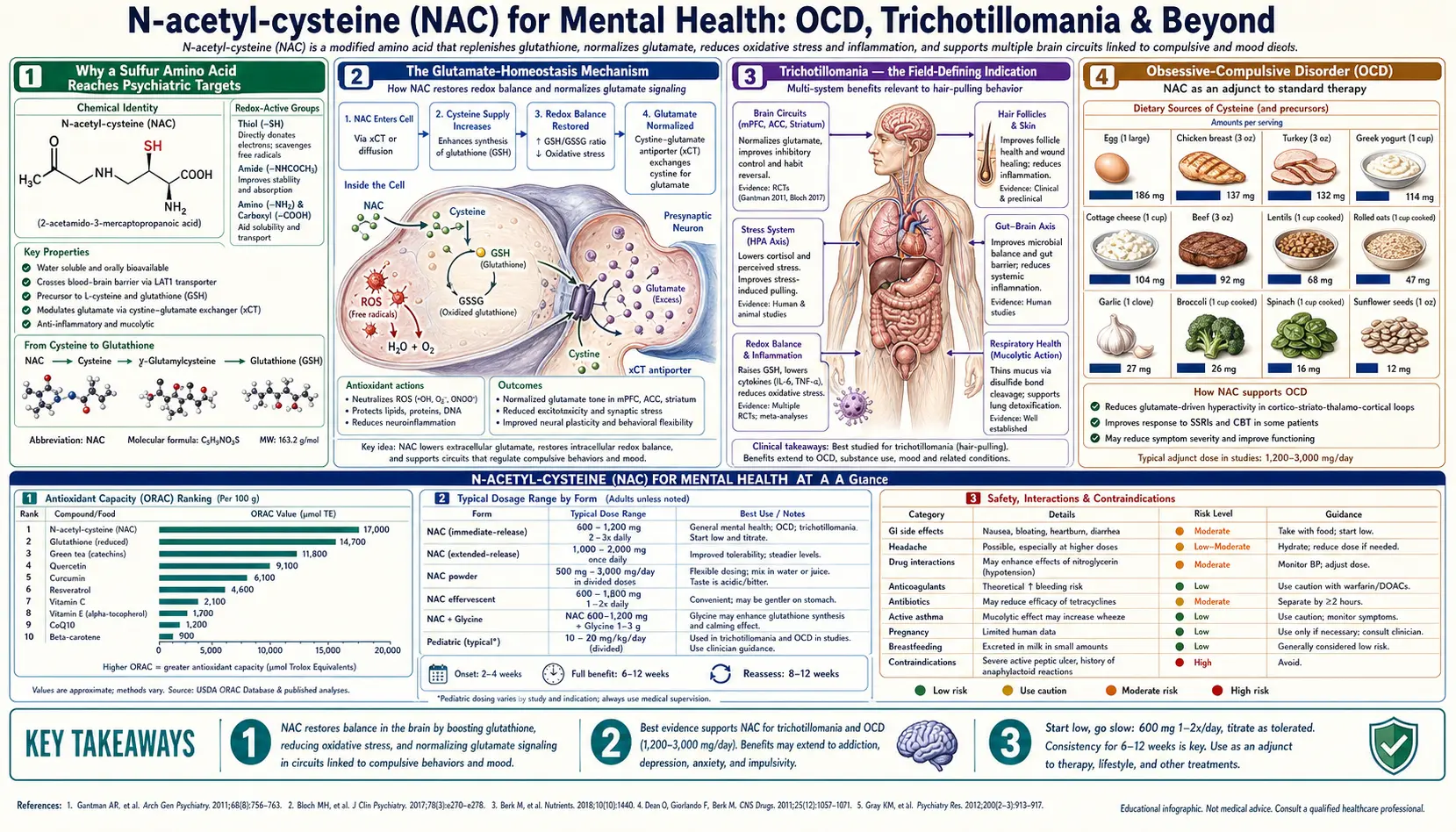
Why a Sulfur Amino Acid Reaches Psychiatric Targets
The standard pharmacological framework for treating psychiatric disorders involves manipulating monoamine neurotransmitters — serotonin, norepinephrine, dopamine. SSRIs, SNRIs, atypical antipsychotics, and TCAs all work on monoamine receptors or reuptake systems. The framework has been productive but incomplete: many patients do not respond to monoamine-targeted drugs, and some of the most disabling features of psychiatric illness (negative symptoms in schizophrenia, anhedonia in depression, compulsive behaviors in OCD-spectrum disorders) often persist despite optimized monoamine pharmacology.
The past 25 years of psychiatric neuroscience has identified glutamate, the brain's principal excitatory neurotransmitter, as a parallel target. Glutamate-system dysfunction shows up in essentially every major psychiatric disorder. The challenge has been finding drugs that modulate glutamate gently — direct NMDA-receptor antagonism (like ketamine) is too dramatic for chronic use, and conventional glutamate-targeted drugs have been hard to develop.
NAC offers something unusual: a way to modulate extrasynaptic glutamate tone indirectly through cystine-glutamate exchange. The mechanism is gentle, gradual, and well-tolerated for indefinite dosing. Layered on top of the glutamate effect are NAC's antioxidant and anti-inflammatory actions, both of which matter independently in mood, psychotic, and neurodevelopmental disorders. The result is a single molecule with documented benefit across an unusually wide psychiatric range.
The Glutamate-Homeostasis Mechanism
The cystine-glutamate antiporter (system xc−) is a plasma-membrane transporter expressed on astrocytes that exchanges one cystine molecule from extracellular fluid for one glutamate molecule from inside the cell. Function: import cystine for glutathione synthesis inside the astrocyte; export glutamate to maintain a baseline extracellular glutamate concentration outside the synapse.
The extrasynaptic glutamate tone matters because it activates metabotropic glutamate receptors mGluR2 and mGluR3, which are inhibitory presynaptic autoreceptors. When mGluR2/3 are activated, they reduce phasic glutamate release at the synapse. In other words: extrasynaptic tonic glutamate dampens synaptic glutamate signaling. This is a homeostatic feedback loop that keeps glutamate signaling in a useful range.
In disorders characterized by glutamate dysregulation — OCD, trichotillomania, addictions, bipolar depression, schizophrenia — system xc− activity is reduced. Extrasynaptic glutamate tone falls. The mGluR2/3 brake on synaptic glutamate fails. Phasic glutamate release becomes dysregulated. The patient experiences this as compulsive behaviors, craving, mood instability, or positive psychotic symptoms depending on the affected circuit.
NAC delivers cysteine, which is rapidly converted (intracellularly and extracellularly) to cystine. The increased cystine availability drives system xc− activity. Extrasynaptic glutamate rises. mGluR2/3 activation restores the brake on phasic glutamate release. The result is reduced compulsive drive, reduced craving, and improved mood/cognitive symptoms — over weeks of consistent dosing, not minutes.
This mechanism is best documented in the nucleus accumbens (for addictions) and the orbitofrontal cortex (for OCD-spectrum disorders), but system xc− is expressed throughout the brain and the effect generalizes.
Trichotillomania — the Field-Defining Indication
Trichotillomania is compulsive hair-pulling. Patients pull scalp hair, eyebrows, eyelashes, or pubic hair, often without conscious awareness during the act. The condition affects approximately 1–2% of adults, is more common in women, and has historically been resistant to SSRI treatment.
The Grant 2009 trial (Archives of General Psychiatry) was a 12-week double-blind placebo-controlled trial of NAC 1,200–2,400 mg/day in 50 adults with trichotillomania. Results:
- 56% of NAC patients were rated "much improved" or "very much improved" on the Clinical Global Impression scale, versus 16% of placebo patients (p < 0.001)
- Significant reductions in Massachusetts General Hospital Hair Pulling Scale scores
- Symptomatic improvement was apparent by week 9 of treatment
- Side effects were minimal — some GI upset, no serious adverse events
This trial was a turning point. Trichotillomania had no FDA-approved treatment; SSRIs had repeatedly failed in randomized trials; and habit-reversal therapy (the behavioral standard of care) was only partially effective for many patients. The Grant 2009 results offered the first robust pharmacological option, and the mechanistic story (glutamate modulation in OCD-spectrum disorders) was internally consistent with what was known about the disorder's neurobiology.
Subsequent trials in adolescents with trichotillomania (Grant 2014) showed smaller effect sizes, suggesting the response may be more reliable in adults than in children. Open-label experience consistently supports the adult finding.
The clinical implication: any adult with trichotillomania who has not responded to habit-reversal therapy should be offered NAC 1,200–2,400 mg/day as a first-line pharmacological intervention. Expect 8–12 weeks to assess response. The intervention is well-tolerated and inexpensive.
Obsessive-Compulsive Disorder (OCD)
OCD treatment standardly involves SSRIs (often at high doses) and exposure-response prevention (ERP) therapy. Approximately 40–60% of patients have partial response or non-response to standard treatment. Augmentation strategies historically included atypical antipsychotics (risperidone, aripiprazole) which have meaningful side effect burdens.
Afshar et al. (2012, Journal of Clinical Psychopharmacology) randomized 48 OCD patients with partial SSRI response to NAC 600 mg three times daily (1,800 mg total) or placebo for 12 weeks, on top of their existing SSRI. Results: significantly greater reduction in Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores in the NAC group, with separation from placebo emerging at week 6 and increasing through week 12.
A subsequent trial by Sarris et al. (2015) in treatment-resistant OCD showed mixed results — nominal benefit but not reaching statistical significance on the primary outcome. A 2017 meta-analysis of the available trials concluded NAC has modest but real augmentation benefit in OCD when added to SSRIs, with effect size approximately 0.4 (small-to-moderate).
Practical OCD augmentation protocol: NAC 600 mg three times daily for at least 12 weeks on top of an optimized SSRI dose. If response is partial, increase to 1,200 mg three times daily (3,600 mg total) and continue for an additional 4–8 weeks before judging final response. The 12-week minimum trial reflects how slowly the glutamate-homeostasis mechanism operates — patients should be told upfront that effect builds gradually and is not visible in the first few weeks.
Skin Picking (Excoriation) and Nail Biting
Skin-picking disorder (excoriation) and nail biting (onychophagia) share the compulsive-behavior phenotype with trichotillomania and have similar response patterns to NAC. The Grant 2016 placebo-controlled trial in 66 adults with excoriation disorder tested NAC 1,200 mg twice daily for 12 weeks. Results: 47% of NAC patients were responders versus 19% on placebo. Effect sizes were similar to the trichotillomania trial.
Open-label experience with NAC for nail biting and lip biting is also positive. Doses used are similar (1,200–2,400 mg/day). The mechanism is presumed identical — glutamate homeostasis in the orbitofrontal-striatal loop that mediates compulsive grooming behaviors.
Bipolar Depression
Bipolar depression is notoriously difficult to treat. Antidepressants risk inducing manic switches; lithium and lamotrigine help some patients but leave many partially treated; the spectrum of approved adjunctive agents is narrow.
The Berk group at Deakin University in Australia has produced the most influential NAC psychiatric work. Berk 2008 (Biological Psychiatry) randomized 75 bipolar patients to NAC 2 g/day or placebo as adjunct to their existing mood stabilizers, for 24 weeks. Primary outcome: Montgomery-Åsberg Depression Rating Scale (MADRS) at week 24. Results: significantly greater MADRS reduction in the NAC group, with effect emerging gradually over weeks 8–24. Secondary outcomes (Bipolar Depression Rating Scale, Clinical Global Impression) also favored NAC.
Berk 2014 attempted a replication in a larger 252-patient bipolar trial. Results were less robust: NAC produced a non-significant trend toward depression reduction on the primary outcome but secondary outcomes still favored NAC. The 2014 trial enrolled a less depressed baseline population, which may have reduced sensitivity.
A 2016 meta-analysis (Fernandes) pooling Berk 2008, Berk 2014, and several smaller trials concluded NAC has modest adjunctive benefit in bipolar depression with effect size approximately 0.5, supporting use as an add-on for partially responsive patients.
Practical bipolar depression protocol: NAC 1 g twice daily (2 g total) added to existing mood stabilizers. Continue for at least 16–24 weeks before assessing response. The slow onset is consistent with the broader pattern in psychiatric NAC trials.
Schizophrenia and Negative Symptoms
Antipsychotic medications are reasonably effective for the positive symptoms of schizophrenia (hallucinations, delusions, disorganized thought) but largely ineffective for negative symptoms (amotivation, anhedonia, social withdrawal, flat affect). Negative symptoms are the principal driver of long-term functional disability in schizophrenia and are an area of intense research interest.
Berk 2008 (Biological Psychiatry, second trial that year) randomized 140 chronic schizophrenia patients on stable antipsychotic regimens to NAC 1 g twice daily or placebo for 24 weeks. Primary outcome: Positive and Negative Syndrome Scale (PANSS) total score. Results: NAC group showed significantly greater improvement in PANSS total, with the effect largely driven by reductions in negative symptoms and general psychopathology rather than positive symptoms.
The result is mechanistically coherent: glutamate dysfunction (the hypoglutamatergic hypothesis of schizophrenia) is thought to underlie negative symptoms and cognitive deficits more than positive symptoms. NAC's gentle pro-glutamatergic action through system xc− activation would be expected to target precisely these dimensions.
Subsequent trials (Conus 2018 in early-stage psychosis, Sepehrmanesh 2018 augmentation) have largely supported the Berk finding with modest effect sizes. NAC is not a substitute for antipsychotic treatment, but is a reasonable adjunct for residual negative symptoms in stable patients. Dose: 1 g twice daily on top of existing antipsychotic regimen, 24 weeks minimum trial.
Autism Spectrum Disorder Irritability
Hardan et al. (2012, Biological Psychiatry) at Stanford randomized 33 children with autism spectrum disorder to NAC 900–2,700 mg/day (titrated upward over the trial) or placebo for 12 weeks. Primary outcome: Aberrant Behavior Checklist-Irritability subscale. Results: NAC group showed significantly greater reduction in irritability scores, including measures of tantrums, aggression, and self-injurious behavior. Effect was apparent by week 4 and continued through week 12. Side effects were minimal.
The Hardan trial was small and has not been definitively replicated at large scale, but the finding is consistent with NAC's broader profile of effects on compulsive and dysregulated behaviors. The mechanism is presumed to involve both glutamate modulation and the antioxidant/neuroinflammatory pathways that show abnormalities in autism brain tissue.
Practical use: NAC 600–1,200 mg twice daily in autistic children with significant irritability, particularly when atypical antipsychotics (the standard pharmacological option) are causing weight gain or other side effects. The benefit is modest but the safety profile is favorable.
Cocaine, Cannabis, Nicotine, Gambling
The cystine-glutamate antiporter is densely expressed in the nucleus accumbens, the brain reward circuitry that mediates addiction. Animal models showed that chronic cocaine exposure reduces system xc− activity in the nucleus accumbens, and restoring it (with NAC) reduces drug-seeking behavior after withdrawal. This mechanistic story drove a wave of clinical trials in the late 2000s and early 2010s.
- Cocaine — LaRowe and colleagues conducted several trials of NAC for cocaine craving and use. Results have been mixed. The most rigorous trial (LaRowe 2013, 111 participants, 8 weeks) showed no significant difference in cocaine use between NAC and placebo on the primary outcome, but secondary analyses suggested NAC was helpful for already-abstinent patients in preventing relapse. The current view: NAC has a role in relapse prevention but not in active-use reduction.
- Cannabis (adolescents) — Gray et al. (2012, American Journal of Psychiatry) randomized 116 cannabis-dependent adolescents to NAC 1,200 mg twice daily or placebo for 8 weeks alongside brief counseling. Results: NAC group showed more than 2-fold higher odds of negative urine cannabinoid screens during treatment. This was the most positive addiction trial of NAC. A subsequent adult cannabis trial (Gray 2017) was negative, suggesting the adolescent finding may not generalize.
- Nicotine — Knackstedt et al. (2009) showed NAC reduced nicotine reinforcement in animal models. Human smoking-cessation trials have been mixed; modest effect on craving and reduced cigarette consumption, but not yet at the level of established cessation pharmacotherapies (varenicline, bupropion, NRT).
- Pathological gambling — Grant et al. (2007) open-label trial of NAC in 27 pathological gamblers showed reduction in gambling thoughts and urges. The effect held in subsequent placebo-controlled work but the literature is thin.
The pattern across addictions: NAC is most useful as a relapse-prevention adjunct in already-abstinent patients, less useful in active-use reduction. Doses are typically 1,200 mg twice daily.
PTSD with Substance Use
Back et al. (2016, Journal of Clinical Psychiatry) randomized 35 veterans with comorbid PTSD and substance use disorder to NAC 2,400 mg/day or placebo for 8 weeks alongside cognitive-behavioral therapy. Results: NAC group showed greater reduction in PTSD symptoms and substance craving compared to placebo. The trial was small but the mechanism (glutamate and oxidative-stress involvement in both PTSD and addiction) is coherent.
This finding has not yet been definitively replicated at scale but is suggestive enough to consider NAC adjunctively in patients with the dual diagnosis. Dose: 1,200 mg twice daily, 8–16 weeks.
Practical Timeline of Psychiatric Response
One of the most important things to communicate to patients starting NAC for a psychiatric indication is that the response is slow. The glutamate-homeostasis mechanism builds over weeks, not hours. The general timeline:
- Week 1–2: No subjective change. Some patients report mild GI upset that resolves.
- Week 3–6: Subtle changes may begin — reduced craving, slightly easier to resist compulsive urges, mildly improved mood. Often noticed in retrospect rather than during the week.
- Week 8–12: Most trials show separation from placebo emerging in this window. If a response is going to happen, it usually starts being clearly perceptible here.
- Week 16–24: Maximum response in most trials. Continue indefinitely if effective.
- Discontinuation: Symptoms typically return over weeks-to-months after stopping. Psychiatric NAC is best framed as an ongoing maintenance medication, not a course of treatment.
This timeline is dramatically different from SSRIs (where some benefit is often visible by week 2–4) and from acute interventions like benzodiazepines or stimulants. Setting accurate expectations is essential to retention — patients who quit at week 4 because "it's not working" never give the medication a fair trial.
Dosing by Indication
| Indication | Typical Dose | Trial Duration |
|---|---|---|
| Trichotillomania | 1,200–2,400 mg/day divided | 12 weeks minimum |
| OCD (SSRI augmentation) | 600 mg TID = 1,800 mg/day | 12 weeks minimum |
| Skin picking / nail biting | 1,200–2,400 mg/day divided | 12 weeks minimum |
| Bipolar depression (adjunct) | 1 g BID = 2,000 mg/day | 16–24 weeks |
| Schizophrenia (adjunct) | 1 g BID = 2,000 mg/day | 24 weeks |
| Autism irritability | 600–1,200 mg BID (weight-adjusted) | 12 weeks |
| Cannabis (adolescent) | 1,200 mg BID = 2,400 mg/day | 8 weeks |
| PTSD with substance use | 1,200 mg BID = 2,400 mg/day | 8–16 weeks |
Across all psychiatric indications, divide the daily dose into 2–3 administrations to maintain steady cysteine availability. Effervescent or solution forms are often better tolerated than capsules because the sulfur taste is masked. Take with or without food.
Cautions
- Slow onset. Set expectations: 8–12 weeks minimum before judging response. Many patients quit prematurely.
- NAC is an adjunct, not a substitute for primary psychiatric medication. Continue mood stabilizers, antipsychotics, and SSRIs as prescribed. Do not stop primary medications without psychiatric supervision.
- Manic switch risk in bipolar: theoretically low (NAC has no monoamine activity) and not documented in the Berk trials, but reasonable to monitor for affective shift after starting in a patient with bipolar history.
- GI tolerability: nausea is the main practical limit. Start at half the target dose for one week, then escalate. Take with food if needed.
- Sulfur breath: common, sometimes socially awkward, harmless.
- Pregnancy: Category B. The trichotillomania, OCD, and bipolar literature has not enrolled pregnant women systematically; NAC's safety in pregnancy is established primarily through its use in acetaminophen overdose (where it has been given at very high doses without teratogenic signal).
- Pediatric autism dosing should be weight-adjusted and titrated. Start at the lower end of the dose range.
- Drug interactions: see the main NAC overview and the Cardiovascular Health page. The nitroglycerin interaction (potentiated vasodilation) is the most clinically significant.
Key Research Papers
- Grant JE et al. (2009). N-acetylcysteine, a glutamate modulator, in the treatment of trichotillomania: a double-blind, placebo-controlled study. Archives of General Psychiatry. — PubMed
- Afshar H et al. (2012). N-acetylcysteine add-on treatment in refractory obsessive-compulsive disorder: a randomized, double-blind, placebo-controlled trial. Journal of Clinical Psychopharmacology. — PubMed
- Berk M et al. (2008). N-acetyl cysteine for depressive symptoms in bipolar disorder — a double-blind randomized placebo-controlled trial. Biological Psychiatry. — PubMed
- Berk M et al. (2014). The efficacy of adjunctive N-acetylcysteine in major depressive disorder: a double-blind, randomized, placebo-controlled trial. Journal of Clinical Psychiatry. — PubMed
- Berk M et al. (2008). N-acetyl cysteine as a glutathione precursor for schizophrenia — a double-blind, randomized, placebo-controlled trial. Biological Psychiatry. — PubMed
- Hardan AY et al. (2012). A randomized controlled pilot trial of oral N-acetylcysteine in children with autism. Biological Psychiatry. — PubMed
- Gray KM et al. (2012). A double-blind randomized controlled trial of N-acetylcysteine in cannabis-dependent adolescents. American Journal of Psychiatry. — PubMed
- LaRowe SD et al. (2013). A double-blind placebo-controlled trial of N-acetylcysteine in the treatment of cocaine dependence. American Journal on Addictions. — PubMed
- Grant JE et al. (2016). N-acetylcysteine in the treatment of excoriation disorder: a randomized clinical trial. JAMA Psychiatry. — PubMed
- Back SE et al. (2016). A double-blind, randomized, controlled pilot trial of N-acetylcysteine in veterans with posttraumatic stress disorder and substance use disorders. Journal of Clinical Psychiatry. — PubMed
- Deepmala et al. (2015). Clinical trials of N-acetylcysteine in psychiatry and neurology: A systematic review. Neuroscience & Biobehavioral Reviews. — PubMed
- Fernandes BS et al. (2016). N-acetylcysteine in depressive symptoms and functionality: a systematic review and meta-analysis. Journal of Clinical Psychiatry. — PubMed
PubMed Topic Searches
- PubMed: NAC trichotillomania
- PubMed: NAC OCD
- PubMed: NAC bipolar depression
- PubMed: NAC schizophrenia negative symptoms
- PubMed: NAC autism irritability
- PubMed: system xc- addiction mechanism
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- NAC Overview
- NAC Benefits Hub
- NAC as Acetaminophen Antidote
- NAC for COPD & Lung
- NAC as Glutathione Precursor
- NAC & Mental Health (Overview)
- Glutathione
- OCD
- Bipolar Disorder
- Schizophrenia
- Autism
- Cysteine
- Glycine
- Natural Anxiety Relief
- Oxidative Stress
- All Antioxidants