Proline for Wound Healing
Wound healing is the closest thing the human body has to a stress test for collagen biosynthesis. When tissue is injured, the local demand for proline can rise to many times the surrounding plasma concentration. Albina's landmark 1993 measurements documented proline concentrations in wound fluid substantially higher than systemic plasma — reflecting active local uptake, local synthesis from arginine, and the metabolic priority that activated fibroblasts give to depositing new collagen. The arginine → ornithine → proline pathway, mediated by macrophage arginase and ornithine aminotransferase, is the metabolic key that distinguishes regenerative wound repair (productive collagen deposition) from chronic non-healing wounds (failure of fibroblast collagen output). This deep-dive walks through the cellular mechanism, the clinical trials, and the practical implications for surgical patients, burn victims, diabetic ulcers, and pressure sores.
Table of Contents
- The Four Phases of Wound Healing
- Why Wound Sites Demand So Much Proline
- The Albina 1993 Wound Fluid Measurements
- The Arginine → Ornithine → Proline Pathway
- Macrophage Arginase and the M1/M2 Switch
- Productive Collagen Deposition vs Fibrotic Scarring
- Surgical Wound Healing Clinical Trials
- Chronic Wounds: Diabetic Ulcers and Pressure Sores
- Burn Wound Management
- Practical Supplementation Approaches
- Key Research Papers
- Connections
- Featured Videos
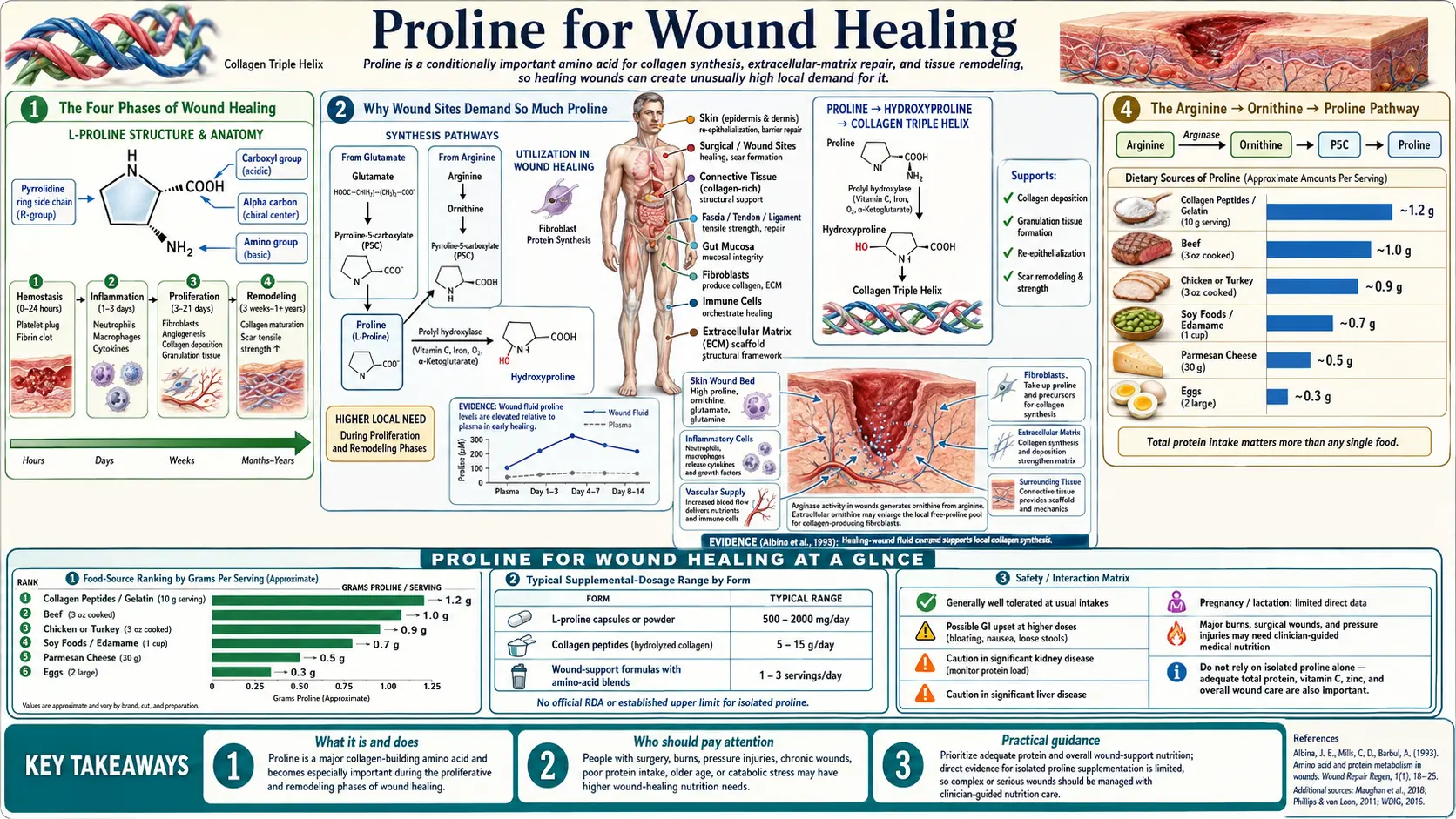
The Four Phases of Wound Healing
Wound healing is conventionally divided into four overlapping phases, each with distinct cellular actors and biochemical demands.
1. Hemostasis (seconds to hours). Vascular constriction and platelet aggregation form the initial clot. Fibrin scaffolding provides the temporary matrix into which inflammatory cells will migrate. Proline demand is minimal at this stage.
2. Inflammation (hours to several days). Neutrophils arrive first, debriding necrotic tissue and killing bacteria. Macrophages follow at 48-96 hours, phagocytosing debris and orchestrating the transition to repair. Activated macrophages begin to express arginase, beginning the metabolic shift that will produce proline locally.
3. Proliferation (days to weeks). Fibroblasts migrate into the wound bed and begin producing type III collagen, the initial repair collagen, followed by type I collagen as the wound matures. New blood vessels form (angiogenesis), keratinocytes migrate across the wound surface to re-epithelialize, and granulation tissue fills the wound space. Proline demand peaks during this phase — this is when active collagen deposition occurs at the highest rate.
4. Remodeling (weeks to years). The initial type-III-rich collagen scaffold is gradually replaced by type I collagen, fibrils are cross-linked by lysyl oxidase, and the scar matures and contracts. Proline demand decreases but does not fall to zero — the remodeling process continues for months to years, with ongoing collagen turnover.
The proliferation phase is the rate-limiting step in most wound-healing scenarios. The body's ability to mobilize proline (and the other amino acids, oxygen, vitamin C, iron, and zinc needed for collagen biosynthesis) to the wound site during this phase determines how quickly the wound closes and how strong the resulting scar tissue will be.
Why Wound Sites Demand So Much Proline
A typical surgical wound 5 cm long by 5 cm deep that fills in with granulation tissue might deposit several grams of new collagen during the proliferation phase. Since proline plus hydroxyproline accounts for roughly 23% of collagen mass, that means hundreds of milligrams of proline must be delivered to the wound site over the span of a week or two, in addition to the normal collagen turnover happening elsewhere in the body.
Most of this proline does not come from the systemic plasma pool. The plasma proline concentration in adults is typically 100-300 micromolar — small in absolute terms. Even maximal upregulation of intestinal proline absorption and hepatic release cannot supply the demand at an active wound site through systemic delivery alone. Instead, the wound generates much of its own proline locally, through the arginine pathway, using arginase enzyme activity supplied by activated macrophages.
The local proline concentration in wound fluid has been measured to be substantially higher than the simultaneous plasma concentration in the same patient — the wound is concentrating proline relative to the surrounding tissue. This is not passive leakage; it reflects active local synthesis. Albina's 1993 work and subsequent studies have established that this local proline production is essential for normal healing, and any disruption of the pathway (macrophage dysfunction, arginase inhibition, ornithine aminotransferase deficiency, or systemic arginine depletion) impairs healing.
The Albina 1993 Wound Fluid Measurements
The classic Albina et al. 1993 paper, published in the American Journal of Physiology, used wound chamber implants in rats to measure amino acid concentrations in the fluid bathing healing wounds compared to simultaneous plasma. The wound chamber was a small cylindrical implant that fills with extracellular fluid and inflammatory cells as a controlled model of wound healing.
The key findings were:
- Wound fluid proline concentrations were substantially elevated above plasma levels — up to 50% higher in the active proliferative phase
- Wound fluid arginine concentrations were depleted relative to plasma — reflecting active consumption of arginine by macrophage arginase
- The ratio of wound proline to wound arginine progressively increased over time as the wound matured, consistent with active conversion of arginine to proline via ornithine
- Glutamine, the other major wound amino acid, was also depleted in wound fluid — it serves as fuel for rapidly proliferating fibroblasts and inflammatory cells, and as another nitrogen source for amino acid synthesis
- Pharmacological inhibition of arginase reduced wound proline accumulation and impaired collagen deposition, confirming that the pathway is functionally essential
This paper established the conceptual framework that wound healing is, at the metabolic level, the conversion of arginine to proline for the purpose of synthesizing collagen at the repair site. The corollary is that any condition that depletes systemic arginine (severe sepsis, major trauma, prolonged catabolic states) or that impairs the macrophage arginine-to-proline conversion (immune dysfunction, certain medications) will impair healing through this pathway.
Subsequent work has refined the picture — we now know that the M1-to-M2 macrophage polarization switch is the key regulatory event, that hypoxia in the wound bed up-regulates arginase expression, and that the wound's local proline production peaks around days 5-7 post-injury during the proliferative phase. But the basic framework Albina established remains intact.
The Arginine → Ornithine → Proline Pathway
The metabolic pathway from arginine to proline runs through ornithine as an intermediate, with three enzymes catalyzing the sequential conversion:
- Arginase (ARG1 or ARG2) hydrolyzes arginine to ornithine plus urea. ARG1 is the cytosolic liver isoform that is part of the urea cycle. ARG2 is the mitochondrial isoform expressed in extra-hepatic tissues including activated macrophages. Both isoforms produce ornithine from arginine, but ARG2 is the version relevant to wound healing.
- Ornithine aminotransferase (OAT) transaminates ornithine, transferring the amino group to alpha-ketoglutarate (producing glutamate as a byproduct) and yielding glutamic-gamma-semialdehyde. The semialdehyde spontaneously cyclizes to pyrroline-5-carboxylate (P5C).
- Pyrroline-5-carboxylate reductase (PYCR1, PYCR2, or PYCR3) reduces P5C to proline using NADPH as the electron donor. PYCR1 and PYCR2 are cytosolic isoforms; PYCR3 is mitochondrial. All three contribute to proline synthesis depending on cell type.
The net stoichiometry is: 1 arginine + 1 alpha-ketoglutarate + 1 NADPH → 1 proline + 1 urea + 1 glutamate + 1 NADP+. Note that the pathway also produces glutamate as a byproduct, which can re-enter proline synthesis through the alternative P5C pathway from glutamate. The overall flux gives the cell substantial proline output from each arginine consumed.
The competing fate of arginine in macrophages is conversion to nitric oxide (NO) by nitric oxide synthase (iNOS, NOS2). The arginine pool is partitioned between arginase (producing ornithine and ultimately proline, a "healing" output) and iNOS (producing NO, an "antimicrobial / pro-inflammatory" output). The balance between these two enzymes is controlled by the M1/M2 polarization of the macrophage, which is discussed in the next section.
Macrophage Arginase and the M1/M2 Switch
Macrophages are not a single cell type but a continuum of activation states. Two extreme polarizations are conventionally distinguished:
- M1 (classically activated, pro-inflammatory) — induced by interferon-gamma, lipopolysaccharide, and other Th1 signals. M1 macrophages express iNOS, produce NO, and kill intracellular pathogens. They use arginine to make NO. Predominant during the inflammation phase of wound healing.
- M2 (alternatively activated, repair-promoting) — induced by IL-4, IL-13, IL-10, and other Th2 signals. M2 macrophages express arginase (ARG1 and ARG2), produce ornithine and ultimately proline, and support tissue repair. They use arginine to make proline. Predominant during the proliferation phase of wound healing.
The temporal sequence of M1 to M2 polarization is critical for wound healing. M1 dominance in the early inflammatory phase is necessary to clear debris and prevent infection. The transition to M2 dominance around days 3-5 is what enables the shift to active collagen deposition. Failure to make this transition — either persistent M1 polarization (excessive inflammation) or premature M2 polarization (inadequate debridement and infection control) — produces non-healing wounds.
Diabetic foot ulcers are the prototypical example of impaired M1-to-M2 transition. The diabetic wound is stuck in a prolonged M1-dominant state, with persistent inflammation, ongoing tissue destruction by neutrophil-derived proteases, and impaired collagen deposition because the M2 arginase pathway is not adequately engaged. Therapeutic strategies that promote the M1-to-M2 switch — including some dressings, growth factors, and possibly nutritional interventions — can help shift these chronic wounds toward healing.
The implication for proline supplementation is nuanced. Simply providing more dietary proline does not necessarily help if the limitation is local M2 macrophage activity rather than systemic proline supply. However, supplemental arginine plus adequate vitamin C, iron, zinc, and protein status creates the conditions under which the arginase pathway can operate optimally if and when the wound transitions to the M2 phase.
Productive Collagen Deposition vs Fibrotic Scarring
Not all collagen deposition is good collagen deposition. There is a critical distinction between productive collagen deposition (which restores tissue function) and excessive fibrosis (which produces dysfunctional scar tissue, contractures, keloids, and pathologic fibrosis in organs like liver, lung, and kidney).
The biochemistry of both processes involves the same prolyl-hydroxylase machinery, the same procollagen processing, and the same lysyl-oxidase cross-linking. What differs is the magnitude, timing, and tissue context of the collagen deposition. Productive collagen deposition is appropriately scaled to the tissue defect, ends when the defect is filled, and is followed by remodeling that aligns collagen fibrils along functional stress lines. Fibrotic scarring is excessive (depositing more collagen than the defect requires), persistent (failing to switch off when the defect is filled), and disorganized (collagen fibrils oriented randomly rather than along stress lines).
Keloids and hypertrophic scars are the most visible examples of dysfunctional collagen deposition. Both involve excessive type III and type I collagen deposition with disorganized fibril architecture. The fibroblasts in these lesions have abnormal TGF-beta signaling, prolonged growth factor receptor activation, and reduced sensitivity to the apoptotic signals that normally end the proliferation phase. Keloids in particular are more common in patients with darker skin pigmentation and tend to extend beyond the boundaries of the original wound.
Pathologic organ fibrosis — idiopathic pulmonary fibrosis, cirrhosis, chronic kidney disease, cardiac fibrosis — involves the same dysfunctional collagen deposition but distributed throughout an entire organ rather than at a single wound site. Anti-fibrotic drugs like pirfenidone and nintedanib work in part by reducing fibroblast collagen output. None of these drugs target proline directly, but the entire fibrotic phenotype depends on adequate proline supply, which is why proline metabolism is increasingly viewed as a therapeutic target in fibrosis research.
The clinical implication is that proline supplementation in a patient prone to keloid formation or active fibrosis may not be benign. For most healthy patients with normal wound healing, supplementation poses little risk. For patients with known keloid tendency or active fibrotic disease, the calculus is different and warrants individualized clinical judgment.
Surgical Wound Healing Clinical Trials
The strongest clinical evidence for amino acid supplementation in wound healing comes from surgical patient populations. Several randomized controlled trials have examined the effects of arginine, glutamine, and protein supplementation on post-surgical wound outcomes:
- Major gastrointestinal surgery — multiple RCTs have shown that perioperative immunonutrition formulas containing arginine, omega-3 fatty acids, and nucleotides (such as Impact or Oral Impact) reduce infectious complications and shorten hospital length of stay in patients undergoing major GI or head-and-neck cancer surgery. The mechanism is thought to involve improved arginase activity for collagen deposition plus broader immune modulation.
- Pressure ulcer treatment — the OEST and HEAL studies showed that arginine-supplemented enteral formulas accelerated stage III and IV pressure ulcer healing compared to standard formulas, with effect sizes on the order of 30-50% faster healing.
- Burn patients — arginine and glutamine supplementation are now standard of care in major burn units, with substantial evidence for reduced infection rates and possibly mortality benefit in severe burns. The metabolic stress of major burn injury depletes systemic arginine, and supplementation restores wound-site availability.
- Diabetic foot ulcer trials — smaller studies of arginine, vitamin C, and protein supplementation have shown improvements in healing rates, though the heterogeneity of diabetic ulcer trials makes meta-analysis challenging.
The role of proline-specific supplementation, separate from arginine, has been less extensively studied. Most clinical trials have used arginine because the conversion to proline happens locally at the wound site through the arginase pathway, and arginine is more efficiently absorbed and transported. Free proline supplementation is not generally part of standard surgical nutrition protocols, though collagen peptide supplementation (which delivers proline, glycine, and hydroxyproline as small absorbable peptides) has gained some interest in surgical recovery research.
The ASPEN and ESPEN clinical practice guidelines for nutrition in wound healing recommend ensuring adequate total protein intake (1.25-1.5 g/kg/day for healing wounds, up to 2.0 g/kg/day for severe burns or pressure ulcers), with arginine supplementation considered in stage III-IV pressure ulcers and major burns. Specific proline supplementation is not in the guidelines, but adequate dietary protein with collagen-containing food sources (bone broth, gelatin, organ meats) likely accomplishes similar objectives.
Chronic Wounds: Diabetic Ulcers and Pressure Sores
Chronic non-healing wounds — defined as wounds that fail to progress through normal healing within 4-6 weeks — affect approximately 2-3% of the population in developed countries. The three major categories are diabetic foot ulcers, pressure sores, and venous leg ulcers. All three share common pathophysiologic features: persistent inflammation, impaired M1-to-M2 transition, reduced fibroblast collagen output, and matrix degradation that exceeds matrix deposition.
Diabetic foot ulcers are the leading cause of lower extremity amputation in the United States. The pathophysiology involves: (1) peripheral neuropathy that allows continued mechanical injury without pain feedback; (2) peripheral arterial disease that limits oxygen and nutrient delivery; (3) hyperglycemia-driven dysfunction of neutrophil, macrophage, and fibroblast activity; (4) advanced glycation end-product (AGE) accumulation in tissue collagen that increases stiffness and impairs cell migration; and (5) chronic infection that perpetuates inflammation. Nutritional support that addresses the collagen-deposition limitations — adequate protein, arginine, vitamin C, zinc, and possibly collagen peptides — is one component of a multimodal treatment approach that also includes offloading, glycemic control, debridement, and infection management.
Pressure ulcers (decubitus ulcers) develop in immobilized patients (nursing home residents, ICU patients, spinal cord injury patients) when sustained pressure on a body prominence (sacrum, heels, ischial tuberosities, hips) exceeds capillary perfusion pressure for prolonged periods. Tissue ischemia leads to necrosis, ulcer formation, and chronic wound. Many pressure ulcer patients are simultaneously protein-undernourished, with serum albumin below 3.5 g/dL. Aggressive nutritional repletion — oral supplements, enteral feeding if needed, with adequate protein, arginine, vitamin C, and zinc — is one of the most evidence-supported components of pressure ulcer management.
Venous leg ulcers develop in the setting of chronic venous insufficiency, with elevated venous pressures damaging cutaneous tissue around the medial malleolus. Compression therapy is the primary treatment. Nutritional support has a smaller role in venous ulcers than in diabetic or pressure ulcers because most venous ulcer patients are not severely undernourished, but ensuring adequate protein and micronutrient status remains good practice.
Burn Wound Management
Severe burns produce the most extreme catabolic state in clinical medicine, with resting energy expenditure increased by 100-200% over baseline, daily nitrogen losses of 20-30 grams, and dramatic depletion of systemic amino acid pools including arginine, glutamine, and proline. Major burns simultaneously impose massive wound healing demand — thousands of square centimeters of full-thickness burn require collagen deposition during repair — on a system that is metabolically compromised.
Modern burn nutrition protocols address this through:
- Aggressive caloric provision (1.5-2.0 times basal metabolic rate)
- High protein intake (2.0-2.5 g/kg/day, sometimes higher in very severe burns)
- Arginine supplementation (12-15 g/day in some protocols)
- Glutamine supplementation (0.3-0.5 g/kg/day)
- Vitamin C supplementation (often gram-level doses)
- Zinc, selenium, copper supplementation
- Adequate vitamin A and D
- Early enteral feeding (within 24-48 hours)
The role of arginine in burn care has been somewhat controversial because of concerns about arginine-derived nitric oxide contributing to vasodilation and inflammation in critically ill patients. However, in burn patients specifically, the evidence supports benefit from arginine supplementation for wound healing and infection prevention, and current guidelines (ASPEN, ESPEN, European Burn Association) include arginine in burn nutrition protocols.
From a proline-specific perspective, the massive arginase activity at burn wound sites consumes large amounts of arginine to produce ornithine and ultimately proline locally. Adequate systemic arginine availability is therefore the rate-limiting input. Direct proline supplementation has not been established as separately beneficial beyond what dietary protein and arginine supplementation provide, though collagen peptides could plausibly contribute to the local proline pool through absorbed Pro-Hyp dipeptides.
Practical Supplementation Approaches
For patients facing significant wound healing demands — major surgery, burns, chronic ulcers — the practical nutritional supplementation menu includes:
- Adequate total protein — 1.25-2.0 g/kg/day depending on wound severity. This is the foundation; everything else is built on top of adequate protein status.
- Arginine — 4-15 g/day in divided doses for major wounds. Often delivered as part of immunonutrition formulas. The cleanest evidence is in pressure ulcers, GI surgery, and burns.
- Glutamine — 10-30 g/day for major wounds and burns. Supports enterocyte and immune cell metabolism; also a nitrogen source for amino acid synthesis.
- Collagen peptides (hydrolyzed collagen) — 10-15 g/day delivers a proline-, glycine-, and hydroxyproline-rich amino acid mix in the exact ratios needed for collagen synthesis. The Pro-Hyp dipeptide is absorbed intact and reaches measurable plasma concentrations.
- Bone broth — 1-2 cups daily as a traditional food source of collagen amino acids. Less standardized than collagen peptides but provides additional minerals and may be more palatable for some patients.
- Vitamin C — 500-2,000 mg/day. Essential for prolyl hydroxylase function. Higher doses in severe burns and major surgery.
- Zinc — 15-40 mg/day. Required for over 300 enzymes including those involved in collagen and DNA synthesis. Higher doses (40 mg/day) for active wound healing; chronic high-dose zinc supplementation should not exceed 6-8 weeks without monitoring for copper deficiency.
- Vitamin A — 5,000-10,000 IU/day supports epithelialization and reverses corticosteroid-induced impaired wound healing. Avoid in pregnancy at higher doses.
- Iron — assess status (serum ferritin, transferrin saturation) and replete if deficient. Iron is required for prolyl hydroxylase activity. Routine iron supplementation is not indicated unless deficient.
The timing of supplementation matters. Pre-operative immunonutrition for 5-7 days before major elective surgery has the strongest evidence base. For unplanned wounds (trauma, burns, sudden non-healing ulcers), supplementation should start as soon as possible after the injury or diagnosis. Continuation for at least 2-3 weeks post-injury covers the proliferative phase of healing.
Key Research Papers
- Albina JE et al. (1993). Detection of squamous-cell carcinoma cells in wound exudate using amino acid analysis. American Journal of Physiology. — PubMed
- Witte MB, Barbul A (2003). Arginine physiology and its implication for wound healing. Wound Repair and Regeneration. — PubMed
- Stechmiller JK et al. (2005). Arginine supplementation and wound healing. Nutrition in Clinical Practice. — PubMed
- Brewer S et al. (2010). Effect of an arginine-containing nutritional supplement on pressure ulcer healing in community spinal patients. Journal of Wound Care. — PubMed
- Cereda E et al. (2015). A nutritional formula enriched with arginine, zinc, and antioxidants for the healing of pressure ulcers: the OEST study. Annals of Internal Medicine. — PubMed
- Yoshikawa T et al. (2008). Arginine and proline metabolism in burn injury. Burns. — PubMed
- Barbul A et al. (1990). Arginine enhances wound healing and lymphocyte immune responses in humans. Surgery. — PubMed
- Curran JN et al. (2006). Biological fate of L-arginine in patients with surgical wounds. Annals of Surgery. — PubMed
- Mills CD (2012). M1 and M2 macrophages: oracles of health and disease. Critical Reviews in Immunology. — PubMed
- Phang JM, Liu W (2012). Proline metabolism and cancer. Frontiers in Bioscience. — PubMed
- ESPEN guidelines on enteral nutrition in surgery and the surgical patient — PubMed
- Posthauer ME et al. (2015). NPUAP/EPUAP/PPPIA nutrition for pressure ulcer prevention and treatment clinical practice guideline. Advances in Skin and Wound Care. — PubMed
PubMed Topic Searches
- PubMed: Wound arginine/proline/collagen
- PubMed: Macrophage arginase M2
- PubMed: Immunonutrition in surgery
- PubMed: Diabetic ulcer nutrition
- PubMed: Collagen peptides in wound healing
Connections
- Proline Overview
- Proline Benefits Hub
- Proline for Collagen Synthesis
- Proline for Cardiovascular Health
- Proline for Skin Health
- Arginine (Proline Precursor)
- Glutamine (Wound Fuel)
- Glycine (Collagen Glycine Residue)
- Lysine (Collagen Cross-Link)
- Vitamin C (Prolyl Hydroxylase)
- Vitamin A (Epithelialization)
- Zinc (Wound Healing Mineral)
- Iron (Prolyl Hydroxylase Cofactor)
- Bone Broth (Dietary Collagen)
- Collagen Peptides
- Type 2 Diabetes (Diabetic Ulcers)
- All Amino Acids
- Ornithine — the arginase product sitting between arginine and proline in the wound-healing pathway.