Proline for Cardiovascular Health
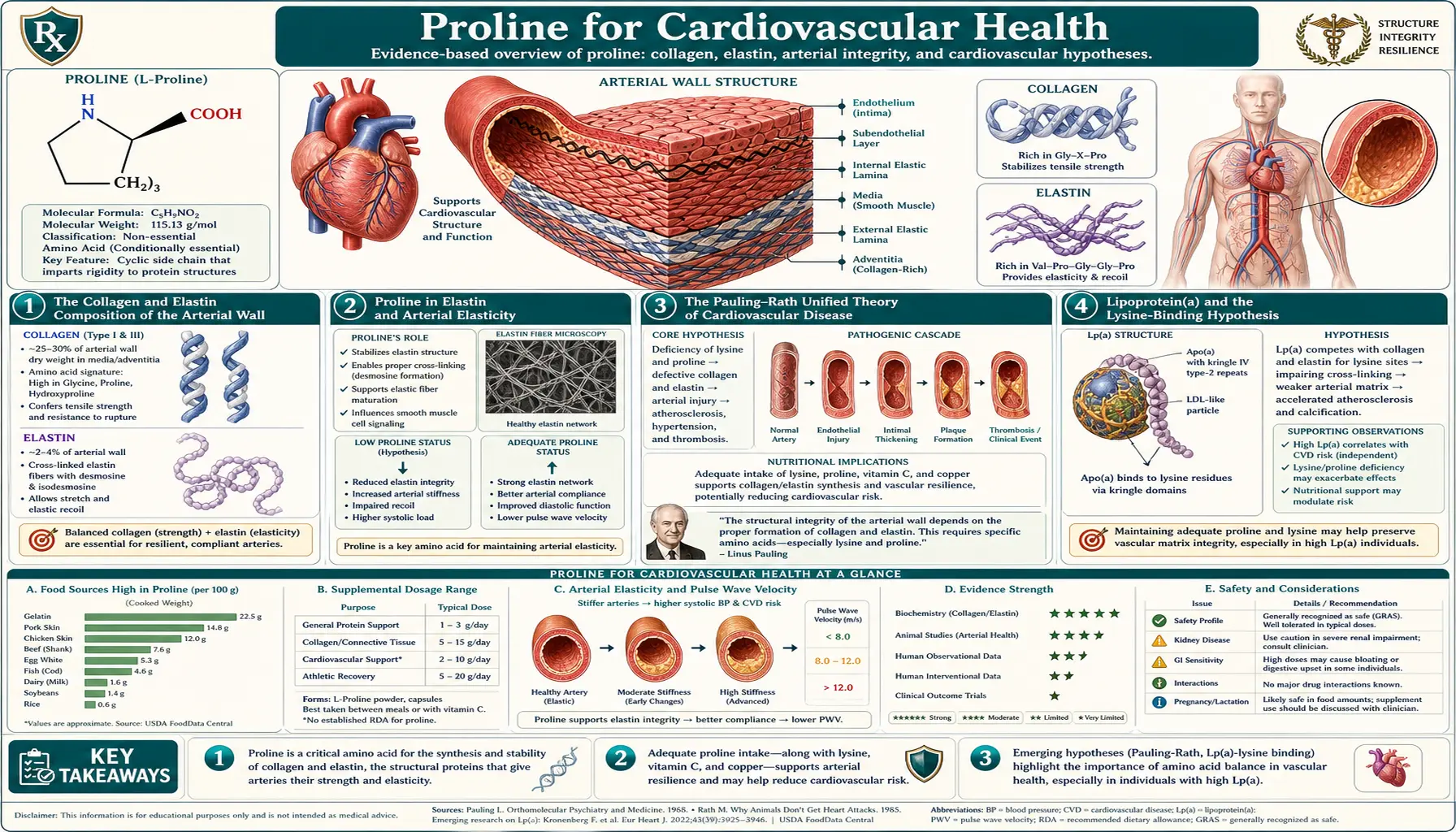
The walls of human arteries contain approximately 25-30% collagen by dry weight, plus elastin (which itself is also proline-rich), plus smooth muscle, plus the proteoglycan-rich extracellular matrix. Every arterial wall is fundamentally a proline-and-elastin construct, capable of resisting decades of pulsatile pressure precisely because proline residues in collagen and elastin give the wall both tensile strength and elastic recoil. In 1991-1994, two-time Nobel laureate Linus Pauling and physician Matthias Rath proposed a "unified theory" of cardiovascular disease in which atherosclerosis is fundamentally a chronic, subclinical scurvy of the arterial wall — with deposition of lipoprotein(a) and other lipoproteins acting as a "molecular Band-Aid" to compensate for defective collagen. The theory is unconventional and remains debated, but the underlying biochemistry — proline, lysine, and vitamin C as the structural backbone of arterial connective tissue — is uncontroversial. This deep-dive walks through the arterial-collagen biology, the Pauling-Rath hypothesis, the lipoprotein(a) connection, and the practical implications for vascular aging.
Table of Contents
- The Collagen and Elastin Composition of the Arterial Wall
- Proline in Elastin and Arterial Elasticity
- The Pauling-Rath Unified Theory of Cardiovascular Disease
- Lipoprotein(a) and the Lysine-Binding Hypothesis
- Subclinical Scurvy and Arterial Wall Weakness
- Vascular Aging, Cross-Linking, and Arterial Stiffness
- Aneurysm and Collagen-Elastin Matrix Failure
- Vascular Ehlers-Danlos Syndrome (Type III Collagen)
- The Pauling Protocol — Practical Application
- Cautions and Caveats
- Key Research Papers
- Connections
- Featured Videos
The Collagen and Elastin Composition of the Arterial Wall
The arterial wall consists of three layers: the intima (innermost, single-cell endothelial lining plus thin subendothelial layer), the media (middle, the muscular layer that gives arteries their contractile and elastic properties), and the adventitia (outermost, connective tissue sheath that anchors the artery in surrounding tissue). Each layer has a characteristic protein composition, but collagen and elastin together account for the bulk of the structural protein content across all three layers.
In a typical large elastic artery (such as the aorta), the dry weight composition is approximately:
- Collagen — 25-30% of arterial dry weight. Predominantly types I and III, with smaller amounts of types IV (basement membrane), V (fibril regulation), VI (microfibrils), and others. Type I collagen provides tensile strength; type III provides distensibility.
- Elastin — 25-30% of arterial dry weight in elastic arteries (aorta, large branches); progressively lower in muscular arteries. Provides the elastic recoil that smooths pulsatile flow.
- Smooth muscle cells — the active contractile element, more abundant in muscular arteries than in elastic arteries.
- Proteoglycans and glycosaminoglycans — hyaluronan, versican, and other proteoglycans that hydrate the matrix and modulate cell behavior.
- Other matrix proteins — fibrillin (the microfibril framework on which elastin is laid down), fibronectin, laminin, and others.
Proline plus hydroxyproline accounts for roughly 23% of the residues in arterial collagen, just as in collagen elsewhere. The total proline-derivative content of an adult aorta is therefore on the order of several grams — a significant amino acid pool that must be maintained throughout life.
The continuous mechanical stress on arterial walls (approximately 100,000 cardiac cycles per day, each one stretching and recoiling the artery) imposes constant low-level damage that must be continuously repaired through ongoing collagen turnover. The half-life of arterial collagen is months to years, much longer than the days-to-weeks half-life of skin collagen, but the cumulative turnover over decades requires sustained supply of proline, lysine, and the prolyl/lysyl hydroxylation cofactors.
Proline in Elastin and Arterial Elasticity
Elastin is the protein responsible for the elastic recoil of arteries, lungs, and skin. It is structurally distinct from collagen but shares one key feature: it is also proline-rich. Mature elastin is approximately 10-12% proline by residue count, plus additional hydroxyproline. The proline residues in elastin contribute to its characteristic random-coil-like flexibility that allows it to stretch and recoil over millions of cycles without fatigue.
Elastin synthesis is dramatically different from collagen synthesis in one critical respect: it occurs almost exclusively during fetal development and early childhood, with very limited capacity for synthesis in adult tissues. The elastin in your aorta was largely deposited before you were 12 years old, and that same elastin must last for the rest of your life. Adult vascular smooth muscle cells can synthesize small amounts of elastin under repair conditions, but the bulk elastin content of the arterial wall does not turn over substantially in adulthood.
This developmental constraint has profound implications for vascular aging. Elastin in the arterial wall is subjected to oxidative damage, advanced glycation end-product formation (especially in diabetes), proteolytic cleavage by matrix metalloproteinases, and calcium deposition over decades. The damage accumulates without effective repair, contributing to arterial stiffening and pulse pressure elevation that characterize older arteries. Proline supplementation in adulthood cannot rebuild the elastin lost to decades of damage, because the synthetic machinery for elastin assembly is largely turned off after development.
Collagen, by contrast, retains active turnover in adult arteries. The collagen in your aorta today is not the same collagen molecules that were there 20 years ago — collagen is continuously degraded by matrix metalloproteinases and replaced by newly synthesized collagen. This ongoing turnover is what makes adult vascular collagen amenable to nutritional support through proline, lysine, and vitamin C, whereas elastin is essentially fixed.
The clinical implication is that nutritional support for arterial wall integrity in adults primarily affects the collagen turnover pathway. The elastin damage that has already accumulated cannot be reversed by any nutritional intervention. The best one can do nutritionally is support the ongoing collagen repair and slow further damage to the existing elastin.
The Pauling-Rath Unified Theory of Cardiovascular Disease
In 1991 and 1992, Linus Pauling (two-time Nobel laureate — chemistry 1954, peace 1962) and Matthias Rath (a German physician who had previously published on lipoprotein(a) biology) jointly published a series of papers proposing what they called a "unified theory" of human cardiovascular disease. The theory rests on three core propositions:
- Atherosclerosis is fundamentally a chronic, subclinical form of scurvy — the arterial wall is constantly under low-level damage from blood pressure and shear stress, requiring continuous collagen-based repair. Suboptimal vitamin C status (insufficient to produce clinical scurvy but inadequate for optimal prolyl-hydroxylase function) results in chronic under-hydroxylation of newly synthesized arterial collagen and progressive arterial wall weakness.
- Lipoprotein(a), or Lp(a), functions as a molecular Band-Aid — the unique apolipoprotein(a) component of Lp(a) has high homology to plasminogen and contains "kringle" domains that bind lysine residues exposed in damaged collagen. Lp(a) accumulates at sites of arterial wall damage as the body's attempt to seal microscopic breaches in the failing collagen matrix. Over time, this accumulation produces the lipid-rich plaques characteristic of atherosclerosis.
- The treatment is restoration of the underlying collagen matrix — high-dose vitamin C (typically 3-6 g/day) plus lysine (3-6 g/day) plus proline (1-3 g/day) provides the building blocks needed for the arterial wall to rebuild its collagen. The lysine and proline saturate the lysine-binding sites on Lp(a), preventing further binding to arterial walls and potentially displacing existing Lp(a) from atherosclerotic plaques.
Pauling and Rath argued that this framework explains why humans (and the few other species that cannot synthesize vitamin C, such as guinea pigs and bats) develop atherosclerosis while species that synthesize abundant endogenous vitamin C (most other mammals) almost never do. They cited the historical observation that scorbutic guinea pigs develop atherosclerosis-like lesions in their arteries, and that providing vitamin C reverses the lesions. They proposed that human atherosclerosis is the cumulative result of millennia of marginal vitamin C intake combined with the genetic loss of endogenous synthesis.
The mainstream cardiology community has been skeptical of the unified theory for several reasons: (1) randomized trials of vitamin C supplementation alone (without lysine and proline) have not shown clear cardiovascular benefit; (2) the Lp(a)-as-band-aid hypothesis is mechanistically plausible but has not been definitively proven; (3) the theory does not fully account for the role of LDL cholesterol, oxidized LDL, inflammation, and other established atherosclerosis risk factors. However, the theory has gained considerable traction in naturopathic and integrative medicine circles, and the underlying observations — that arterial collagen requires vitamin C, lysine, and proline; that Lp(a) does bind lysine via its kringle domains; that vitamin C deficiency does produce arterial wall damage — are not in dispute.
Even cardiologists skeptical of the unified theory generally agree that maintaining adequate vitamin C intake and avoiding overt scurvy is important for cardiovascular health, and that the theory is at minimum a useful framework for thinking about the structural integrity of the arterial wall as a contributor (alongside lipid metabolism, inflammation, and endothelial function) to atherosclerosis.
Lipoprotein(a) and the Lysine-Binding Hypothesis
Lipoprotein(a), abbreviated Lp(a), is a unique lipoprotein particle consisting of an LDL-like core (apolipoprotein B-100, cholesterol, phospholipids) covalently linked via a disulfide bond to a special protein called apolipoprotein(a), or apo(a). The apo(a) protein has a highly unusual structure: it consists of multiple repeating "kringle" domains that are highly homologous to the kringle domains of plasminogen, the precursor of the fibrin-degrading enzyme plasmin.
The number of kringle IV type 2 repeats in apo(a) is genetically determined and varies between individuals from approximately 11 to 50+ repeats. The number of repeats is inversely correlated with serum Lp(a) concentration — people with few repeats produce small apo(a) proteins that are easily secreted and reach high serum concentrations; people with many repeats produce large apo(a) proteins that are inefficiently secreted and reach lower serum concentrations. Serum Lp(a) concentrations span a wide range, from less than 10 mg/dL to greater than 300 mg/dL, and are predominantly genetically determined.
High serum Lp(a) is an independent risk factor for cardiovascular disease, separate from LDL cholesterol. Elevations above approximately 50 mg/dL roughly double cardiovascular event risk in epidemiologic studies. The mechanism by which Lp(a) increases cardiovascular risk has been debated for decades, with proposed mechanisms including:
- Lp(a) binding to lysine-containing extracellular matrix at sites of arterial damage (the Pauling-Rath mechanism)
- Interference with plasmin-mediated fibrinolysis (Lp(a) competes with plasminogen)
- Pro-inflammatory effects of oxidized phospholipids carried on Lp(a)
- Direct uptake by macrophages to form foam cells
These mechanisms are not mutually exclusive; Lp(a) likely contributes to atherosclerosis through several simultaneous pathways. The Pauling-Rath insight that the kringle domains specifically bind lysine residues is mechanistically correct and has been confirmed by structural studies. Whether dietary lysine and proline supplementation can saturate these binding sites and prevent or reverse Lp(a) deposition in arteries is the central testable claim of the unified theory, and unfortunately definitive randomized trials have not been conducted.
Modern Lp(a)-targeted pharmaceutical therapies (antisense oligonucleotides, siRNA approaches) are in late-stage clinical trials. These drugs reduce serum Lp(a) by 80-90% through reduced hepatic production. Whether these will translate to clinical benefit in randomized cardiovascular outcome trials remains to be seen. Either way, the existence of Lp(a)-targeted drug development reflects mainstream cardiology's acceptance that Lp(a) plays a causal role in atherosclerosis — consistent with the Pauling-Rath framework even if the proposed nutritional treatment remains unproven.
Subclinical Scurvy and Arterial Wall Weakness
One of the most compelling lines of evidence for the role of vitamin C and proline in arterial wall integrity comes from animal models. Guinea pigs, like humans, cannot synthesize vitamin C and depend on dietary intake. When guinea pigs are fed marginal vitamin C diets — enough to prevent overt scurvy but below optimal intake — they develop atherosclerosis-like lesions in their arteries within weeks to months. Providing higher-dose vitamin C reverses the lesions and prevents new ones.
This work, originally done by Constance Spittle and others in the 1970s and 1980s, was extended by Rath and Pauling in the 1990s with guinea pig models specifically designed to test the unified theory. They showed that vitamin-C-deficient guinea pigs develop accumulation of Lp(a)-like apolipoproteins in their arterial walls, consistent with the molecular Band-Aid hypothesis. Adding back vitamin C reversed the deposition; adding lysine and proline to vitamin C provided additional benefit.
The mainstream cardiology counter-argument is that guinea pigs are an imperfect model for human atherosclerosis (guinea pig arteries differ in some respects from human arteries), and that the lesions in scorbutic guinea pigs may differ mechanistically from human atherosclerosis. These objections have some merit but do not eliminate the basic observation that vitamin C deficiency produces arterial damage in a species that cannot synthesize the vitamin — an observation that is at minimum consistent with the unified theory.
In humans, the evidence for subclinical scurvy contributing to cardiovascular disease is necessarily more indirect because severe vitamin C deficiency is rare in modern populations. Epidemiologic studies have generally shown that low serum vitamin C is associated with increased cardiovascular risk, though confounding factors (lower fruit and vegetable intake correlates with many other adverse health behaviors) make causal inference difficult. Randomized trials of vitamin C supplementation alone (without companion lysine and proline) have generally failed to show cardiovascular benefit, which Pauling-Rath proponents argue is because the protocol was incomplete — vitamin C alone, without the building blocks for new collagen, cannot reverse established arterial damage.
Vascular Aging, Cross-Linking, and Arterial Stiffness
One of the most important changes in arterial structure with aging is progressive arterial stiffening — arteries become less elastic, more rigid, and less able to dampen the pulsatile flow from the heart. This is measured clinically as pulse wave velocity (PWV), with higher PWV indicating stiffer arteries. Arterial stiffness predicts cardiovascular events, stroke, and dementia risk independently of blood pressure and other classical risk factors.
The biology of arterial stiffening involves several processes:
- Elastin damage and replacement by collagen — over decades, elastin fibers fragment, calcify, and lose their elastic recoil. The arterial wall progressively replaces the damaged elastin with collagen, which is stiffer than elastin. Net result: more collagen, less elastin, stiffer artery.
- Advanced glycation end-product (AGE) accumulation — glucose and other reducing sugars react with collagen lysine and hydroxylysine residues to form Schiff bases that progress to stable AGE cross-links over months to years. AGE cross-links increase collagen rigidity. AGE accumulation is dramatically accelerated in diabetes mellitus.
- Enzymatic cross-link accumulation — lysyl oxidase continues to create cross-links between collagen molecules throughout life. Cross-link density increases with age, contributing to stiffening.
- Calcification — calcium phosphate deposition in arterial wall (medial calcification) and in atherosclerotic plaques (intimal calcification) further stiffens the wall.
The role of proline supplementation in vascular aging is largely hypothetical — no controlled trials have specifically tested whether dietary proline can slow arterial stiffening. The mechanistic case is that adequate proline supply supports ongoing collagen turnover, which in turn allows replacement of older, more cross-linked collagen with fresh, less cross-linked collagen, partially counteracting the stiffening process. Whether this translates to measurable clinical benefit in randomized trials remains to be established.
What is clearly established is that hyperglycemia accelerates arterial stiffening through AGE cross-link formation, and that strict glycemic control slows this process. The other established intervention is regular aerobic exercise, which improves arterial elasticity through mechanisms that include enhanced nitric oxide production, reduced inflammation, and possibly favorable effects on collagen turnover. The combination of glycemic control, regular exercise, adequate vitamin C, adequate dietary protein with proline-rich sources, and possibly collagen peptide supplementation represents a reasonable nutritional approach to vascular aging, though none of these is definitively proven to reduce hard cardiovascular outcomes specifically through effects on arterial stiffness.
Aneurysm and Collagen-Elastin Matrix Failure
An aneurysm is a focal dilatation of an arterial wall that develops when the wall's structural matrix fails to resist the pulsatile pressure from within the lumen. Aneurysms occur most commonly in the abdominal aorta (abdominal aortic aneurysm, AAA), the thoracic aorta, and the cerebral arteries (intracranial aneurysm, which when ruptured produces subarachnoid hemorrhage). The mechanism in all cases involves progressive degradation of arterial wall collagen and elastin without adequate replacement.
The cellular biology of aneurysm formation involves:
- Matrix metalloproteinase (MMP) up-regulation, particularly MMP-2 and MMP-9, which degrade arterial wall collagen and elastin
- Inadequate compensatory matrix synthesis by vascular smooth muscle cells
- Inflammatory infiltrate (macrophages, T cells) producing additional cytokines that perpetuate the MMP elevation
- Loss of vascular smooth muscle cells through apoptosis
- Hemodynamic stress on the wall section with reduced structural integrity
Risk factors for aneurysm include smoking (the strongest modifiable risk factor for AAA), hypertension, atherosclerosis, family history, male sex, and several connective tissue diseases (Marfan syndrome, Loeys-Dietz syndrome, vascular Ehlers-Danlos syndrome). The connective tissue disease cases are particularly informative for proline biology because they directly implicate collagen and elastin in arterial wall integrity.
Marfan syndrome is caused by mutations in fibrillin-1 (FBN1), the microfibril protein on which elastin is assembled. Loss of normal fibrillin-1 disrupts elastic fiber assembly and produces the characteristic aortic root dilatation that progresses to aneurysm and dissection. Vascular Ehlers-Danlos syndrome (vEDS, also called type IV EDS) is caused by mutations in COL3A1, the gene encoding type III collagen — the second most abundant collagen in arteries. vEDS patients develop spontaneous arterial dissection and rupture at young ages, often without warning, and median survival is approximately 50 years.
Both of these genetic conditions emphasize that the arterial wall's structural integrity depends critically on the collagen-elastin matrix, and that disruption of either component produces life-threatening cardiovascular disease. While nutritional supplementation cannot fix the underlying genetic defect, optimization of available collagen synthesis pathways (proline, vitamin C, copper for lysyl oxidase) is a reasonable supportive intervention in these patients, alongside standard care including beta-blockade, angiotensin receptor blockade, and surgical or endovascular repair when indicated.
Vascular Ehlers-Danlos Syndrome (Type III Collagen)
Vascular Ehlers-Danlos syndrome (vEDS) deserves a dedicated section because it is the clinical condition that most directly demonstrates the importance of proline-rich type III collagen in arterial wall integrity. vEDS is caused by heterozygous loss-of-function or dominant-negative mutations in COL3A1, the gene encoding the alpha-1 chain of type III collagen.
Type III collagen co-distributes with type I collagen in skin, blood vessels, intestine, and uterus — tissues that need both tensile strength (type I) and distensibility (type III). In blood vessel walls, type III collagen makes up approximately 30% of the total collagen and is concentrated in the adventitia and the media. The arterial wall's resistance to sudden hemodynamic stress depends on the elastic-yet-strong type-III-rich matrix being intact.
vEDS patients present clinically with:
- Thin, translucent skin with prominent subcutaneous veins
- Easy bruising
- Spontaneous arterial rupture, often in the abdominal aorta or its branches
- Spontaneous sigmoid colon rupture
- Uterine rupture during pregnancy
- Characteristic facial features (large eyes, thin lips, lobeless ears, sunken cheeks)
- Hypermobility of small joints (sometimes; less prominent than in other EDS types)
The median life expectancy in vEDS is approximately 50 years, with cardiovascular events being the leading cause of death. Patients are advised to avoid contact sports, weightlifting, and other activities that increase arterial pressure. Pregnancy carries substantial risk of uterine and arterial rupture.
Treatment is largely supportive plus aggressive blood pressure control. Celiprolol (a beta-blocker with some intrinsic sympathomimetic activity) has been shown in a randomized trial to reduce arterial event rate. Surgical intervention for arterial complications is technically difficult because the tissue is friable and sutures pull through easily.
The implication for proline biology is striking: a single-gene defect in one collagen type, one component of a complex multi-protein arterial wall, is sufficient to produce catastrophic cardiovascular disease. This emphasizes how central the collagen matrix is to arterial wall function and how vulnerable the wall is to disruption of this matrix. From the broader perspective of vascular aging, the lesson is that maintaining optimal collagen synthesis (proline, lysine, vitamin C, iron, copper) is a foundational strategy for arterial health, even in patients without rare genetic disease.
The Pauling Protocol — Practical Application
For patients (or naturopathic practitioners) interested in implementing the Pauling-Rath approach to cardiovascular health, the basic protocol consists of three components taken throughout the day:
- Vitamin C — 3,000 to 6,000 mg per day, typically divided into multiple doses (e.g. 1,000 mg three times daily). Buffered vitamin C (calcium ascorbate, magnesium ascorbate, or sodium ascorbate) is often used to avoid the gastric acidity of ascorbic acid at gram-level doses. Liposomal vitamin C is an alternative for those who tolerate ascorbic acid poorly. Some practitioners use higher doses (up to 12 g/day) titrated to bowel tolerance.
- L-Lysine — 3,000 to 6,000 mg per day, typically divided. The rationale is to provide both raw material for arterial collagen and to saturate lysine-binding sites on Lp(a), inhibiting binding to arterial walls. Lysine is well-tolerated and inexpensive.
- L-Proline — 1,000 to 3,000 mg per day, typically divided. Often included as the lower-dose third member of the protocol because endogenous proline synthesis is generally adequate in healthy adults; supplementation primarily ensures saturation rather than replacing endogenous supply.
Some practitioners add additional components to the basic protocol: hydroxyproline (which is the modified form actually found in collagen, sometimes available as a supplement), vitamin E (as a complementary antioxidant for the arterial wall), CoQ10 (for mitochondrial support in vascular cells), N-acetylcysteine (as glutathione precursor for endothelial function), and omega-3 fatty acids (for their established anti-inflammatory effects). The expanded protocols vary by practitioner.
Practical considerations include:
- Taking the supplements consistently for at least 6-12 months before evaluating effect on cardiovascular markers (Lp(a), arterial stiffness measures, calcium score progression)
- Continuing standard cardiovascular care including statin therapy if indicated, blood pressure control, and lifestyle modification — the Pauling protocol is positioned as adjunctive rather than substitutive
- Periodic monitoring of serum vitamin C status, basic chemistry, and renal function (especially in patients with chronic kidney disease, where high-dose vitamin C can occasionally precipitate oxalate kidney stones)
- Discussing the protocol with the patient's cardiologist, who may not be familiar with it but should be informed
The evidence base for the Pauling protocol specifically is limited to case reports, case series, and a few small open-label studies. There have been no large randomized controlled trials. Proponents argue this reflects funding priorities (no patentable drug to motivate industry-funded research) rather than lack of efficacy. Skeptics argue it reflects lack of demonstrated effect. The truth is unknown in the absence of definitive trials.
Cautions and Caveats
- The Pauling-Rath unified theory is not mainstream cardiology — patients adopting the protocol should do so with informed understanding that it is not a substitute for standard cardiovascular care, including statin therapy when indicated, blood pressure control, antiplatelet therapy when indicated, and lifestyle modification.
- High-dose vitamin C and kidney stones — chronic intake of more than 2 g/day vitamin C can increase urinary oxalate excretion and modestly increase calcium oxalate kidney stone risk in susceptible individuals. Patients with personal or family history of kidney stones should use lower doses and ensure adequate hydration.
- Lysine and herpes simplex virus — lysine supplementation has been used to reduce HSV outbreak frequency. This is not generally a problem, but arginine supplementation (sometimes added to lysine-proline-C protocols) can worsen herpes outbreaks in susceptible individuals because HSV replication requires arginine. Patients with frequent herpes outbreaks may prefer to avoid arginine if adding it to a Pauling-style protocol.
- Drug interactions — high-dose vitamin C can interfere with some laboratory tests (most notably, urine glucose dipsticks and stool occult blood tests). It may also reduce the effectiveness of warfarin in some patients. Patients on warfarin should monitor INR more frequently when starting high-dose vitamin C.
- Hyperprolinemia — the rare inborn errors of proline metabolism (hyperprolinemia type I from PRODH mutations, hyperprolinemia type II from ALDH4A1 mutations) are contraindications to proline supplementation. These are very rare conditions, typically diagnosed in childhood.
- Pregnancy — high-dose vitamin C, lysine, and proline supplementation has not been specifically studied in pregnancy. Standard prenatal vitamin doses are well-established and safe; higher supplementation should be discussed with the obstetric care provider.
- The protocol does not replace lifestyle — the strongest evidence for cardiovascular disease prevention remains for smoking cessation, regular physical activity, weight management, blood pressure control, glycemic control, and dietary modification (Mediterranean-style or similar evidence-supported pattern). The Pauling protocol, even if effective, would be an adjunct rather than a substitute for these foundational interventions.
Key Research Papers
- Rath M, Pauling L (1992). A unified theory of human cardiovascular disease. Journal of Orthomolecular Medicine. — PubMed
- Rath M, Pauling L (1990). Hypothesis: lipoprotein(a) is a surrogate for ascorbate. Proceedings of the National Academy of Sciences. — PubMed
- Pauling L (1991). Case report: lysine/ascorbate-related amelioration of angina pectoris. Journal of Orthomolecular Medicine. — PubMed
- Maeda N et al. (2000). Aortic wall damage in mice unable to synthesize ascorbic acid. Proceedings of the National Academy of Sciences. — PubMed
- Tsimikas S (2017). A test in context: lipoprotein(a) diagnosis, prognosis, controversies, and emerging therapies. Journal of the American College of Cardiology. — PubMed
- Pepin M et al. (2000). Clinical and genetic features of Ehlers-Danlos syndrome type IV, the vascular type. New England Journal of Medicine. — PubMed
- Ong KT et al. (2010). Effect of celiprolol on prevention of cardiovascular events in vascular Ehlers-Danlos syndrome: a prospective randomised, open, blinded-endpoints trial. Lancet. — PubMed
- Mitchell GF (2014). Arterial stiffness and hypertension: chicken or egg? Hypertension. — PubMed
- Sesso HD et al. (2008). Vitamins E and C in the prevention of cardiovascular disease in men: the Physicians' Health Study II. JAMA. — PubMed
- Knekt P et al. (2004). Antioxidant vitamins and coronary heart disease risk: a pooled analysis of 9 cohorts. American Journal of Clinical Nutrition. — PubMed
- Tsao PS et al. Lysine-binding sites on apolipoprotein(a) and the lysine analog approach — PubMed
- O'Donnell CJ, Elosua R (2008). Cardiovascular risk factors: insights from Framingham Heart Study. Revista Española de Cardiología. — PubMed
PubMed Topic Searches
- PubMed: Pauling-Rath protocol
- PubMed: Lp(a) and lysine binding
- PubMed: Arterial stiffness and collagen
- PubMed: Aneurysm and arterial matrix
- PubMed: Vascular EDS
Connections
- Proline Overview
- Proline Benefits Hub
- Proline for Collagen Synthesis
- Proline for Wound Healing
- Proline for Skin Health
- Lysine (Pauling Protocol)
- Vitamin C (Pauling Protocol)
- Vitamin E (Antioxidant)
- Copper (Lysyl Oxidase)
- Arginine (Nitric Oxide / Caveat)
- Collagen Peptides
- Bone Broth
- Atherosclerosis
- Cardiology (All)
- Type 2 Diabetes (AGEs)
- All Amino Acids