Proline for Skin Health
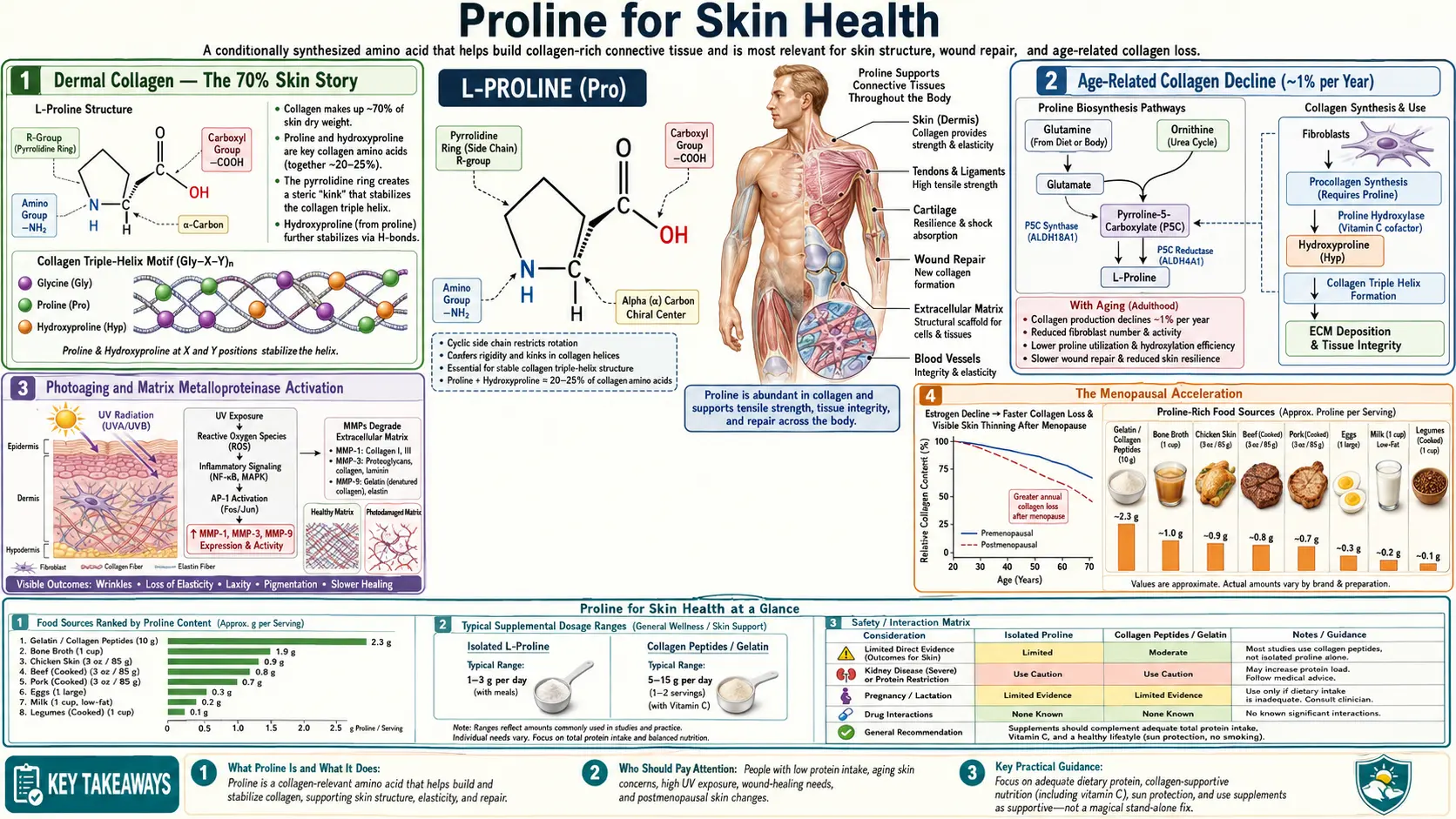
Skin is roughly 70% collagen by dry weight, and the dermal collagen pool turns over slowly but continuously throughout life. Beginning around age 25, dermal collagen content declines by approximately 1% per year, accelerating after menopause in women. The visible result is the familiar progression from firm youthful skin to fine lines, deeper wrinkles, sagging, and loss of facial volume. The oral collagen peptide story — proline, glycine, and hydroxyproline delivered as small hydrolyzed peptides that are absorbed intact and reach the dermis — is the most popular nutritional intervention for skin aging, and it now has a respectable evidence base from randomized double-blind placebo-controlled trials. This deep-dive walks through the dermal collagen biology, the age-related decline mechanism, the Proksch 2014 and Choi 2019 evidence, the practical dosing of collagen peptides, and the supporting role of bone broth as a traditional food source delivering the same amino acid profile.
Table of Contents
- Dermal Collagen — The 70% Skin Story
- Age-Related Collagen Decline (~1% per Year)
- Photoaging and Matrix Metalloproteinase Activation
- The Menopausal Acceleration
- Collagen Peptide Pharmacokinetics — Pro-Hyp Absorption
- Proksch 2014 — The Landmark RCT
- Choi 2019 Systematic Review and Subsequent Trials
- Bone Broth — The Traditional Food Source
- Practical Dosing and Product Selection
- Topical Retinoids vs Oral Collagen — Complementary Strategies
- Key Research Papers
- Connections
- Featured Videos
Dermal Collagen — The 70% Skin Story
Skin consists of three layers: the epidermis (the thin outer keratinocyte-rich layer), the dermis (the thick middle layer responsible for structural support), and the subcutis or hypodermis (the deepest layer containing fat and connective tissue). The dermis is the layer responsible for what we colloquially call "skin quality" — firmness, elasticity, hydration, and resistance to wrinkle formation.
The dermis is approximately 70% collagen by dry weight, with the remainder being elastin (about 5%), glycosaminoglycans and proteoglycans, fibroblasts, blood vessels, lymphatics, nerve endings, sebaceous glands, hair follicles, and sweat glands. The dominant collagen types in the dermis are:
- Type I collagen — 80-85% of dermal collagen, forming the thick fibrils that give skin its tensile strength
- Type III collagen — 10-15% of dermal collagen, providing distensibility and acting as scaffolding for new type I deposition
- Type V collagen — a few percent, co-distributed with type I and regulating fibril diameter
- Type IV collagen — at the dermal-epidermal junction, forming the basement membrane that anchors the epidermis to the dermis
- Type VII collagen — forms anchoring fibrils that further attach the epidermis to the dermis (mutations cause epidermolysis bullosa)
Proline plus hydroxyproline accounts for approximately 23% of all dermal collagen residues. The total proline-derivative content of adult human skin has been estimated at several hundred grams, distributed across many trillions of individual collagen molecules in the dermal extracellular matrix.
This collagen pool is not static. Dermal fibroblasts continuously synthesize new collagen while matrix metalloproteinases (MMPs) degrade old collagen. In healthy young skin, synthesis and degradation are balanced, and the total collagen pool is maintained. With aging, photoaging, and hormonal changes, the balance shifts toward degradation exceeding synthesis, and the collagen pool slowly contracts. This is the molecular basis of visible skin aging.
Age-Related Collagen Decline (~1% per Year)
The most cited statistic about skin aging is that dermal collagen content declines by approximately 1% per year beginning in the third decade of life. This figure comes from histological studies of dermal collagen content in skin biopsies from women across age ranges and represents an average rate — some individuals decline faster, some slower, and the decline accelerates in women after menopause.
The mechanisms driving age-related collagen decline include:
- Reduced fibroblast collagen synthesis — aged fibroblasts produce less procollagen per cell, even when adequate amino acid substrates are available. The mechanism involves reduced transforming growth factor beta (TGF-beta) signaling, reduced procollagen gene transcription, and accumulation of cellular senescence markers in older fibroblasts.
- Increased matrix metalloproteinase (MMP) activity — MMP-1 (collagenase), MMP-2, MMP-3, and MMP-9 are up-regulated in aged skin, particularly photoaged skin. These enzymes degrade existing dermal collagen faster than fibroblasts can replace it.
- Reduced fibroblast cell number and changed cell distribution — the dermis becomes less cellular with aging, with fewer active fibroblasts per unit dermal volume.
- Glycation cross-linking of existing collagen — glucose and other reducing sugars react with collagen lysine and hydroxylysine residues to form advanced glycation end-products (AGEs) that increase collagen rigidity and impair its function. AGE accumulation also makes the collagen molecules less susceptible to normal MMP turnover, which paradoxically traps damaged collagen in place.
- Oxidative damage to fibroblasts and existing collagen — reactive oxygen species damage both the synthetic machinery (fibroblast DNA, ribosomes, ER chaperones) and existing collagen fibrils (causing fragmentation that is then targeted for degradation).
- Reduced cofactor availability — vitamin C status declines somewhat with aging, and the prolyl hydroxylase machinery may operate sub-optimally even when proline and other amino acids are adequate.
The cumulative effect over decades is dramatic. Skin biopsies from elderly individuals show approximately 30-50% less dermal collagen than skin biopsies from young adults from the same anatomical site. Visible aging changes — wrinkles, sagging, thinning, fragility — reflect this underlying collagen loss.
The implication for proline biology is that any intervention aimed at slowing or reversing skin aging needs to either increase fibroblast collagen synthesis, reduce MMP-mediated degradation, prevent AGE cross-linking, or some combination. Oral collagen peptides are hypothesized to work primarily by stimulating fibroblast synthesis through a feedback mechanism that we'll discuss in the pharmacokinetics section.
Photoaging and Matrix Metalloproteinase Activation
Ultraviolet (UV) radiation is the single most important environmental driver of accelerated skin aging. UV exposure produces a distinct pattern of skin changes — photoaging — that is qualitatively and quantitatively different from chronological intrinsic aging. The hallmarks of photoaging are: coarse wrinkles, irregular pigmentation (lentigines, "age spots"), telangiectasias, leathery texture, sallow color, and increased risk of skin cancer.
The molecular mechanism of photoaging involves UV-induced reactive oxygen species formation in the skin, which then activate transcription factor AP-1 (activator protein 1). AP-1 drives expression of multiple matrix metalloproteinases including MMP-1 (interstitial collagenase), MMP-3 (stromelysin-1), and MMP-9 (gelatinase B). These MMPs aggressively degrade dermal collagen at a rate exceeding fibroblast replacement capacity. The result is net loss of dermal collagen with each significant UV exposure, with cumulative effects over years to decades.
Photoaging is most prominent on chronically sun-exposed areas (face, neck, hands, forearms) and can be assessed by comparison with sun-protected areas (typically the inner upper arm or the buttock). The dramatic difference between an elderly individual's sun-exposed face and sun-protected inner upper arm illustrates the cumulative effect of decades of UV exposure.
Prevention of photoaging is essentially identical to prevention of skin cancer: broad-spectrum sunscreen (SPF 30 or higher), avoidance of midday sun exposure, protective clothing, and reasonable sun avoidance behaviors. Once photoaging has developed, treatment is more limited — topical retinoids (tretinoin, retinol, retinaldehyde) and alpha-hydroxy acids can produce modest improvement by stimulating fibroblast collagen synthesis and increasing epidermal turnover. Cosmetic procedures (laser resurfacing, microneedling, fillers, botulinum toxin) address the visible manifestations but do not reverse the underlying dermal damage.
The proline-related implication is that adequate substrate supply for fibroblast collagen synthesis — through dietary protein, collagen peptides, and the prolyl hydroxylase cofactors (vitamin C, iron) — complements UV protection and topical retinoid therapy. None of these interventions in isolation is fully effective for photoaging; the combination of UV avoidance, topical retinoid use, and nutritional support represents a coherent multi-pronged approach.
The Menopausal Acceleration
The age-related 1%-per-year collagen decline accelerates in women after menopause due to loss of estrogen. Estrogen normally supports dermal fibroblast collagen synthesis through estrogen receptor signaling in fibroblasts, and the abrupt loss of estrogen at menopause produces an accelerated phase of collagen loss in the first 5-10 years post-menopause.
The classic study by Brincat et al. (1987) measured dermal collagen content in postmenopausal women and found that approximately 30% of dermal collagen is lost in the first five years after menopause, with a further decline of approximately 2% per year thereafter. This represents a much faster collagen loss than the slow background 1%-per-year that occurs in earlier adulthood.
Hormone replacement therapy (HRT) reverses or substantially slows this accelerated decline. Studies of postmenopausal women on HRT consistently show better-preserved dermal collagen content, skin thickness, and skin elasticity compared to women not on HRT. The skin-aging benefit of HRT is one of several considerations in the risk-benefit calculation for HRT initiation, though it is rarely the primary indication.
For postmenopausal women who are not candidates for HRT (or who prefer not to take HRT), the nutritional support strategy becomes more important as a partial compensatory measure. Oral collagen peptide supplementation has been studied specifically in postmenopausal women, with several trials showing measurable improvements in skin elasticity and reductions in wrinkle depth over 8-12 weeks. The effect sizes are modest but real, and the safety profile is excellent.
Other relevant interventions for postmenopausal skin health include: phytoestrogens (soy isoflavones, red clover) for women who prefer plant-source estrogen-like compounds; topical estrogen creams (sometimes used for vulvar and vaginal atrophy, with possible incidental skin benefit at adjacent sites); and the broader anti-aging measures including adequate sleep, stress management, smoking cessation, and Mediterranean-style dietary patterns rich in antioxidants and polyphenols.
Collagen Peptide Pharmacokinetics — Pro-Hyp Absorption
For oral collagen supplementation to affect dermal collagen, the supplement must somehow reach the dermis as either intact peptides, free amino acids, or signaling molecules that influence fibroblast behavior. Until the mid-2000s, the prevailing assumption was that all dietary proteins are digested to free amino acids before absorption, and that any "collagen-specific" benefit must operate through provision of the amino acids glycine, proline, and hydroxyproline in the ratios found in collagen.
This assumption was overturned by pharmacokinetic studies that detected intact proline-hydroxyproline (Pro-Hyp) and hydroxyproline-glycine (Hyp-Gly) dipeptides in the bloodstream after oral collagen peptide ingestion. The intestinal peptide transporter PEPT1 absorbs di- and tri-peptides intact, and certain collagen-derived peptides — particularly those containing hydroxyproline, which protects the peptide from intestinal proteases — reach measurable plasma concentrations.
The Pro-Hyp dipeptide is particularly interesting because:
- It appears in plasma within 1-2 hours of oral collagen peptide ingestion
- It reaches peak concentrations of approximately 20-40 micromolar after a standard 10-gram collagen peptide dose
- It persists in plasma for many hours due to slow clearance
- It accumulates in skin (detectable by skin biopsy after sustained supplementation)
- It appears to act as a signaling molecule on dermal fibroblasts, increasing collagen synthesis and reducing MMP-1 expression
The fibroblast signaling effect is the key mechanistic insight. Pro-Hyp at physiologically achievable concentrations stimulates dermal fibroblast proliferation, increases hyaluronic acid synthesis, and shifts the balance of MMP-1 (collagenase) versus TIMP-1 (tissue inhibitor of metalloproteinase 1) toward reduced collagen degradation. This is a fundamentally different mechanism from simple "amino acid provision" — the intact dipeptide acts as a regulator of fibroblast behavior, not just a building block.
The mechanistic plausibility of this signaling effect makes collagen peptide supplementation distinct from generic dietary protein supplementation. A patient could meet total protein requirements with chicken breast and rice and not get the Pro-Hyp signaling benefit. Collagen-derived peptides specifically deliver this signaling molecule because hydroxyproline is essentially unique to collagen and must come from collagen-source protein.
Proksch 2014 — The Landmark RCT
The Proksch et al. 2014 paper, published in Skin Pharmacology and Physiology, was the first large rigorous double-blind placebo-controlled trial of oral collagen peptide supplementation for skin elasticity. The study enrolled 69 women aged 35-55 years, randomized to either 2.5 grams or 5.0 grams of specific bioactive collagen peptides (Verisol, manufactured by Gelita) or placebo, taken daily for 8 weeks.
The primary outcome was skin elasticity, measured with a cutometer (a validated instrument that measures skin elastic recovery after applied negative pressure). Secondary outcomes included skin moisture, transepidermal water loss, and skin roughness.
Key findings:
- Skin elasticity improved significantly in both collagen peptide groups compared to placebo (effect size approximately 7% improvement in elastic recovery at 8 weeks)
- The effect was statistically significant at both 4 weeks and 8 weeks
- Older subjects (over 50) showed the largest effect, consistent with the age-related collagen decline being the relevant biology
- Effects persisted partially for 4 weeks after discontinuation
- No safety issues
The Proksch study was followed by a second Proksch paper in 2014 in the same journal examining different bioactive collagen peptides for skin wrinkles (eye-area wrinkle volume measured by skin replica analysis). That study showed measurable reduction in eye-wrinkle volume after 8 weeks of supplementation with 2.5 grams daily of specific collagen peptides, with effects persisting after discontinuation.
These two papers established the modern evidence base for oral collagen peptide supplementation for skin. They are notable for several reasons: (1) the doses tested were realistic for consumer products; (2) the methods were rigorous double-blind placebo-controlled; (3) the outcomes were objective instrumented measurements rather than subjective satisfaction surveys; (4) the effect sizes were modest but meaningful and reproducible.
Choi 2019 Systematic Review and Subsequent Trials
The Choi FD et al. 2019 systematic review in the Journal of Drugs in Dermatology pooled the available evidence on oral collagen supplementation for dermatological applications. The review identified 11 randomized controlled trials with a total of approximately 800 patients, most examining skin elasticity, moisture, or wrinkle outcomes in middle-aged to older women.
The overall conclusions:
- Oral collagen supplementation produces statistically significant improvements in skin elasticity in most placebo-controlled trials
- Skin moisture (hydration) is improved in many trials
- Wrinkle reduction is detectable but with smaller effect sizes
- Most studies have used 2.5-10 grams per day of hydrolyzed collagen for 8-12 weeks
- Effects are dose-dependent in the studied range
- Safety has been excellent across all trials
- The available evidence base is dominated by industry-funded studies, which is a methodological limitation
Subsequent trials published after the Choi review have largely confirmed the basic findings. The Bolke et al. 2019 study, the Asserin et al. 2015 study, the Inoue et al. 2016 study, and others have all shown measurable improvements in objective skin parameters. The Cochrane Skin Group has not yet produced a formal Cochrane review on oral collagen for skin aging.
The major remaining uncertainties in the field are:
- How much of the effect is attributable to the specific Pro-Hyp signaling mechanism versus simple provision of amino acids
- Whether different collagen peptide products (different molecular weight distributions, different bovine/porcine/marine sources) produce different clinical effects
- Whether long-term supplementation (years) sustains the effects seen at 8-12 weeks
- Whether the effect is maintained or lost after discontinuation
- The cost-effectiveness comparison with topical retinoids or cosmetic procedures
Despite these uncertainties, the available evidence is sufficient to conclude that oral collagen peptide supplementation produces modest but real improvements in skin elasticity and hydration in middle-aged and older women, with an excellent safety profile. It is one of the few nutritional interventions for skin aging with credible RCT support, and it is a reasonable addition to a comprehensive skin health regimen.
Bone Broth — The Traditional Food Source
Long before collagen peptide supplements were commercially available, traditional cultures across the world prepared bone broth as a nourishing food — particularly for the convalescent, the elderly, and pregnant women. From a modern biochemical perspective, bone broth is exactly the same thing as a collagen peptide supplement, just prepared by slow simmering bones in water for many hours rather than by enzymatic hydrolysis in a factory.
The slow simmering process hydrolyzes the collagen in the bones, cartilage, and connective tissue into a complex mixture of:
- Free amino acids (glycine, proline, hydroxyproline, glutamate, alanine, others)
- Small peptides (di-, tri-, and tetra-peptides including Pro-Hyp and Hyp-Gly)
- Larger gelatin molecules (intermediate-molecular-weight protein that sets to a gel on cooling)
- Trace minerals from the bones (calcium, phosphorus, magnesium, in modest amounts)
- Glycosaminoglycans (chondroitin sulfate, hyaluronic acid from cartilage)
- Fat-soluble compounds dissolved in the rendered fat (vitamin K2, conjugated linoleic acid, etc., depending on the source)
The amino acid profile of bone broth is essentially identical to that of collagen peptide supplements, since both come from the same collagen-rich starting material. A cup of well-made bone broth (approximately 8 ounces) typically contains 6-10 grams of protein in the form of gelatin and free amino acids, including approximately 1.5-2.5 grams of glycine, 1-1.5 grams of proline, and 1-1.5 grams of hydroxyproline.
The case for bone broth versus collagen peptide supplements is largely a matter of preference, cost, and food culture. Bone broth offers:
- The amino acid profile is delivered as part of a traditional food rather than as an isolated supplement
- Additional nutritional components (minerals, glycosaminoglycans, fat-soluble vitamins)
- Lower cost per serving if homemade
- Palatability for those who enjoy the food
- Versatility as a base for soups, sauces, and braises
The case for collagen peptides over bone broth includes:
- Standardized dose per scoop, with known protein content
- Convenience (mix into coffee, smoothies, oatmeal)
- Tasteless and odorless
- Highly hydrolyzed for fast absorption
- Quality-controlled manufacturing
- No bone-broth preparation time required
For patients who enjoy bone broth and have time to prepare it, traditional bone broth is an excellent way to deliver the collagen amino acid profile. For patients who want the convenience of a standardized supplement, collagen peptides are equally effective. Both work; neither is dramatically superior to the other.
The traditional preparation method matters for bone broth quality. The longest-simmered (24-48 hours for beef bones, 12-24 hours for chicken bones, 4-8 hours for fish bones) broths extract the most collagen and gelatin from the bones. Adding an acid (apple cider vinegar, lemon juice) to the simmering water helps extract minerals and break down the collagen matrix. Roasting the bones first improves flavor. Using bones with attached cartilage, marrow, and connective tissue (knuckle bones, oxtail, chicken feet, fish heads, fish skin) increases the collagen content of the resulting broth.
Practical Dosing and Product Selection
For patients interested in oral collagen supplementation for skin health, practical recommendations include:
- Dose — 10 grams of hydrolyzed collagen peptides per day is a reasonable starting point. Some research has used as little as 2.5 grams (and shown effect), some uses up to 15 grams. Higher doses do not appear to produce dramatically larger effects.
- Duration — expect a minimum of 8 weeks before evaluating effect. Skin biology operates slowly. The Proksch trials measured effect at 4 and 8 weeks, with the 8-week measurement being more reliable.
- Timing — can be taken any time of day. Some people prefer with morning coffee, others mixed into a smoothie or yogurt. Empty stomach versus with food does not appear to matter substantially for collagen peptides (unlike some other supplements).
- Source — bovine, porcine, and marine collagen peptides have all been shown effective in trials. Bovine is the most common and least expensive. Marine collagen has slightly higher proline content. Porcine is less common in the US market. Choose based on dietary preferences (kosher / halal considerations may exclude porcine, vegetarian and vegan diets exclude all animal sources).
- Type — "type I" collagen peptides are most commonly used for skin. "Type II" collagen peptides are sometimes marketed specifically for joint support (the rationale being that articular cartilage is type II). In practice, all hydrolyzed collagen peptide products are highly digested mixtures of amino acids and small peptides regardless of starting collagen type, so the marketing distinction has limited mechanistic meaning.
- Brand — major brands include Vital Proteins, Great Lakes, Ancient Nutrition, Sports Research, Gelita (Verisol, used in the Proksch trials), and many others. Quality is generally consistent across major brands. Look for third-party testing certifications if heavy-metal contamination is a concern.
- Vitamin C co-supplementation — ensure adequate vitamin C intake (200-500 mg/day from supplements or diet) to support the prolyl hydroxylase machinery. This is more important than the specific collagen product chosen.
- Combined products — some products combine collagen peptides with vitamin C, hyaluronic acid, biotin, and other "skin-supporting" ingredients. These are reasonable but typically more expensive per gram of actual collagen.
Patients with food allergies should check the source — bovine collagen can occasionally cause issues in patients with severe beef allergy or alpha-gal syndrome; marine collagen can cause issues in patients with severe fish or shellfish allergy. Patients on certain restrictive diets (carnivore, ketogenic) may already get adequate collagen from connective-tissue-rich meat cuts and slow-cooked stews; supplementation may be redundant for them.
Topical Retinoids vs Oral Collagen — Complementary Strategies
For patients interested in evidence-based anti-aging skin care, oral collagen peptides and topical retinoids represent the two interventions with the strongest scientific evidence base. They operate through entirely different mechanisms and are complementary rather than competing strategies.
Topical retinoids (tretinoin / Retin-A by prescription; over-the-counter retinol and retinaldehyde products) work through retinoic acid receptor (RAR/RXR) signaling in epidermal keratinocytes and dermal fibroblasts. They increase epidermal turnover, normalize keratinocyte differentiation, stimulate fibroblast collagen synthesis, and reduce MMP-1 expression. Effects on dermal collagen content and skin wrinkles are well-documented in multiple RCTs spanning decades. Side effects include initial dryness, peeling, and photosensitivity. Long-term consistent use is required for sustained benefit. See our Vitamin A for Skin page for the full discussion.
Oral collagen peptides work through systemic delivery of Pro-Hyp dipeptide and free amino acids to the dermis, plus signaling effects on dermal fibroblasts. The effect is more subtle than topical retinoids but is achieved without local skin irritation. Particularly useful for patients who cannot tolerate topical retinoids or who want a complementary internal-side intervention.
Combining both interventions is a reasonable evidence-based approach for patients prioritizing anti-aging skin care. A typical regimen might be:
- Morning: oral collagen peptide supplement (10 g, mixed into coffee or smoothie), oral vitamin C (500 mg), broad-spectrum sunscreen SPF 30+ on face/neck/hands
- Evening: topical retinoid (tretinoin 0.025-0.05% or over-the-counter retinaldehyde 0.05-0.1%), moisturizer over retinoid
- Periodic: cosmetic procedures as desired (chemical peels, microneedling, laser resurfacing)
This combination addresses the dermal collagen pool from multiple angles: providing substrate and signaling molecules (collagen peptides + vitamin C), stimulating fibroblast activity directly (topical retinoid), preventing further damage (sunscreen), and treating existing damage (cosmetic procedures as needed). None of these interventions in isolation is fully effective; the combination represents a coherent multi-modal approach with reasonable evidence for each component.
Key Research Papers
- Proksch E et al. (2014). Oral supplementation of specific collagen peptides has beneficial effects on human skin physiology: a double-blind, placebo-controlled study. Skin Pharmacology and Physiology. — PubMed
- Proksch E et al. (2014). Oral intake of specific bioactive collagen peptides reduces skin wrinkles and increases dermal matrix synthesis. Skin Pharmacology and Physiology. — PubMed
- Choi FD et al. (2019). Oral collagen supplementation: a systematic review of dermatological applications. Journal of Drugs in Dermatology. — PubMed
- Asserin J et al. (2015). The effect of oral collagen peptide supplementation on skin moisture and the dermal collagen network: evidence from an ex vivo model and randomized, placebo-controlled clinical trials. Journal of Cosmetic Dermatology. — PubMed
- Inoue N et al. (2016). Ingestion of bioactive collagen hydrolysates enhance facial skin moisture and elasticity and reduce facial ageing signs in a randomised double-blind placebo-controlled clinical study. Journal of the Science of Food and Agriculture. — PubMed
- Bolke L et al. (2019). A collagen supplement improves skin hydration, elasticity, roughness, and density: results of a randomized, placebo-controlled, blind study. Nutrients. — PubMed
- Iwai K et al. (2005). Identification of food-derived collagen peptides in human blood after oral ingestion of gelatin hydrolysates. Journal of Agricultural and Food Chemistry. — PubMed
- Ohara H et al. (2007). Comparison of quantity and structures of hydroxyproline-containing peptides in human blood after oral ingestion of gelatin hydrolysates from different sources. Journal of Agricultural and Food Chemistry. — PubMed
- Brincat M et al. (1987). Long-term effects of the menopause and sex hormones on skin thickness. British Journal of Obstetrics and Gynaecology. — PubMed
- Fisher GJ et al. (2002). Mechanisms of photoaging and chronological skin aging. Archives of Dermatology. — PubMed
- Varani J et al. (2006). Decreased collagen production in chronologically aged skin: roles of age-dependent alteration in fibroblast function and defective mechanical stimulation. American Journal of Pathology. — PubMed
- Shoulders MD, Raines RT (2009). Collagen structure and stability. Annual Review of Biochemistry. — PubMed
PubMed Topic Searches
- PubMed: Oral collagen peptide RCTs
- PubMed: Pro-Hyp dipeptide signaling
- PubMed: Dermal collagen and aging
- PubMed: Photoaging and MMP
- PubMed: Bone broth amino acid analysis
Connections
- Proline Overview
- Proline Benefits Hub
- Proline for Collagen Synthesis
- Proline for Wound Healing
- Proline for Cardiovascular Health
- Glycine (Collagen Co-Star)
- Lysine (Collagen Cross-Link)
- Vitamin C (Prolyl Hydroxylase)
- Vitamin A (Topical Retinoid)
- Vitamin A for Skin
- Zinc (Skin Healing)
- Copper (Lysyl Oxidase)
- Collagen Peptides
- Bone Broth
- Acne
- All Amino Acids