Methionine for Hair and Nails
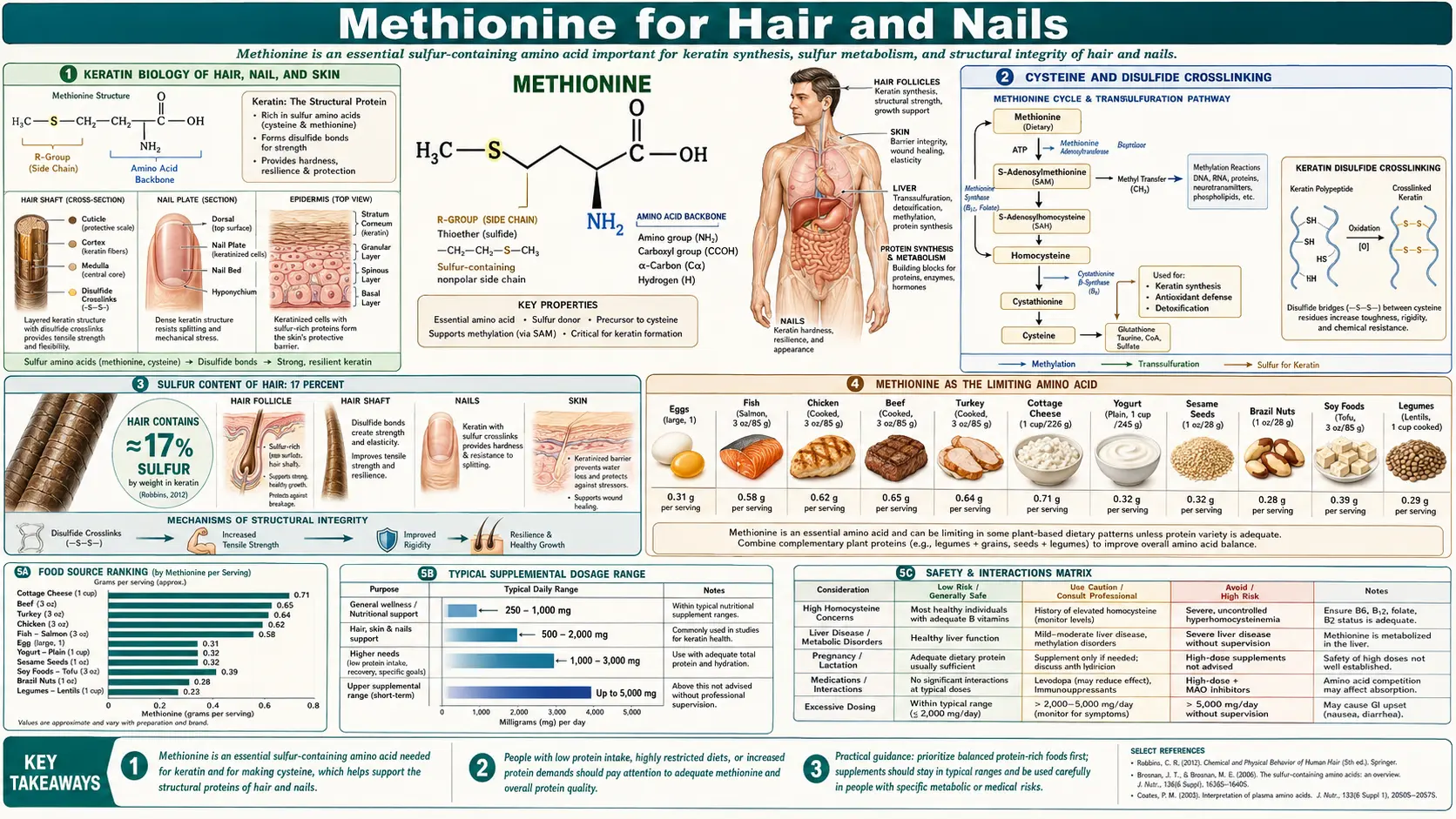
Hair, nails, and the outer layer of skin are built primarily from keratins, a family of intermediate-filament proteins crosslinked by hundreds of disulfide bonds between cysteine residues. The sulfur for those bonds, and the cysteine itself, ultimately comes from dietary methionine via the transsulfuration pathway. Hair shaft keratin is approximately 17% cysteine by amino-acid composition (compared to less than 2% for most cytoplasmic proteins), which means hair synthesis is one of the most sulfur-demanding biosynthetic activities in the body. Methionine is also the textbook example of a "limiting amino acid" in plant proteins — the amino acid present in the smallest amount relative to human requirements in nearly every legume protein (beans, lentils, peas), making it the rate-limiting nutrient for protein quality in any plant-protein-dominant diet. Vegan and vegetarian populations, particularly those eating legume-only protein patterns without grain or seed complementation, have measurably lower methionine status and have been observed in clinical practice to present with hair, nail, and skin quality concerns more often than mixed-diet eaters. This deep-dive walks through keratin biosynthesis, the chemistry of disulfide crosslinking, the limiting-amino-acid concept and protein quality scoring, the clinical patterns of methionine and cysteine inadequacy, and the practical nutritional approach to optimizing hair, nail, and skin building blocks.
Table of Contents
- Keratin Biology of Hair, Nail, and Skin
- Cysteine and Disulfide Crosslinking
- Sulfur Content of Hair: 17 Percent
- Methionine as the Limiting Amino Acid
- Protein Quality Scoring: PDCAAS, DIAAS, PER
- Vegan and Vegetarian Diet Patterns
- Clinical Signs of Sulfur Amino Acid Deficiency
- Nail Disorders and Methionine Status
- Hair Loss Conditions and Methionine
- Practical Nutritional Stack for Hair, Nails, Skin
- Cautions in Hair/Nail Supplementation
- Key Research Papers
- Connections
- Featured Videos
Keratin Biology of Hair, Nail, and Skin
Keratins are intermediate filament proteins that constitute the principal structural component of the cytoskeleton in epithelial cells, and the dominant extracellular matrix of hair, nail, and the outer epidermal layer (stratum corneum). The human genome encodes 54 functional keratin genes, organized into two families:
- Type I (acidic) keratins — K9 through K28 (soft/cytokeratins) and Ha1 through Ha8, Ka35, Ka36 (hard/hair keratins). Generally smaller proteins, around 40-55 kDa.
- Type II (basic-neutral) keratins — K1 through K8 (soft/cytokeratins) and Hb1 through Hb6 (hard/hair keratins). Larger, around 50-70 kDa.
Mature keratin filaments are obligate heterodimers of one type I and one type II monomer, which then assemble into rod-like protofilaments, protofibrils, and finally the macroscopic intermediate filaments visible by electron microscopy. The mechanical properties of the assembled filament (stiffness, tensile strength, resistance to compression) depend on both the primary sequence (different keratins assemble into filaments with different properties) and the post-translational crosslinking pattern (especially disulfide bonds).
The three tissues of interest each have a characteristic keratin pattern:
- Hair shaft — predominantly hair-specific hard keratins (Ka and Hb families) plus an exceptionally large complement of keratin-associated proteins (KAPs). KAPs are small (10-30 kDa) cysteine-rich proteins (some are 30% cysteine by composition) that form the matrix between keratin intermediate filaments, with extensive disulfide crosslinking that produces the characteristic mechanical resilience of hair.
- Nail plate — predominantly hard keratins (similar to hair), with characteristic nail-specific patterns of K81, K83, K85, K86. Cysteine content is high (approximately 10-22% in different nail keratins), and disulfide bonding produces the hardness and flexibility of healthy nail plate.
- Stratum corneum — the outermost layer of epidermis. Predominantly K1 and K10 (soft cytokeratins), with terminal differentiation involving conversion of viable keratinocytes to anucleate corneocytes through a programmed cornification process. Cysteine content is lower than hair or nail (more like 3-5%), and the crosslinking includes both disulfide bonds and isopeptide bonds (transglutaminase-catalyzed) plus a lipid envelope.
The metabolic implication is that hair and nail growth represent unusually high sulfur amino acid demand per unit of new tissue mass. A typical adult grows approximately 0.5 mm of hair per day across 100,000 follicles, plus approximately 0.1 mm per day of fingernail and toenail across 20 nail plates, totaling roughly 8-10 grams of new keratin protein per month. If this protein is 10-17% cysteine, that represents approximately 1-1.5 grams of cysteine per month committed to keratin synthesis alone — entirely beyond the cysteine requirements of every other protein in the body.
Cysteine and Disulfide Crosslinking
The fundamental chemistry of cysteine-derived structural strength is the disulfide bond, a covalent bond between two cysteine residues formed by oxidation of their respective thiol (-SH) groups:
Cys-SH + HS-Cys + 1/2 O2 → Cys-S-S-Cys + H2O
Disulfide bonds have a bond energy of approximately 60 kcal/mol — significantly higher than the hydrogen bonds (5-7 kcal/mol) and van der Waals interactions that hold most folded proteins together. A single keratin protein can contain dozens of intramolecular disulfide bonds (linking distant cysteines within the same chain) plus intermolecular disulfides (linking adjacent chains within the filament). The cumulative effect of hundreds of disulfide bonds across many neighboring keratin and KAP molecules produces an extraordinarily robust covalent network.
Three practical consequences follow from this chemistry:
- Hair, nails, and stratum corneum are physically resilient because of disulfide crosslinking — this is why hair and nails persist on skeletal remains long after soft tissue has decayed; the disulfide network is chemically and biologically stable.
- Permanent waving (perms) chemically reduces and re-oxidizes disulfide bonds — the reducing agent in perm solution (typically ammonium thioglycolate) breaks the existing disulfide bonds, the hair is mechanically reshaped, and an oxidizing solution (hydrogen peroxide) reforms disulfide bonds in the new configuration. Hair straightening uses the same chemistry.
- The sulfur smell of burned hair — hair on fire generates volatile sulfur compounds (hydrogen sulfide, sulfur dioxide, mercaptans) from the high cysteine content, producing the characteristic distinctive odor that differentiates burned hair from other burned materials.
The cysteine for hair, nail, and skin keratin synthesis must come from somewhere. There are three sources:
- Direct dietary cysteine — cysteine is conditionally essential (the body can synthesize it from methionine via transsulfuration, but dietary intake reduces methionine requirement). Foods particularly high in cysteine include eggs (especially the egg white), poultry, organ meats, sunflower seeds, oats, and broccoli (modest amounts).
- Transsulfuration from dietary methionine — the major pathway for endogenous cysteine production. Methionine is converted to homocysteine to cystathionine to cysteine via CBS and CGL (B6-dependent).
- Recycling from protein turnover — existing body proteins are continuously catabolized, releasing their constituent amino acids back into the cellular pool for reuse. This is a major source for any individual amino acid in a steady-state adult, but it does not substitute for adequate dietary intake.
When the combined cysteine supply from these three sources is inadequate, the body prioritizes essential functions: protein synthesis for the immune system, the gut epithelium, and other rapidly dividing tissues. Keratin synthesis for hair and nail growth, while important for the patient, is metabolically deprioritized in protein-restricted states. This is why hair and nail quality is one of the earliest clinically apparent signs of inadequate sulfur amino acid intake, often appearing months before measurable changes in serum albumin or other conventional protein status markers.
Sulfur Content of Hair: 17 Percent
Hair shaft keratin is one of the most cysteine-rich proteins in the body. Different sources give slightly different numbers because the analysis depends on which keratin and which keratin-associated protein subset is measured, but the integrated bulk amino acid composition of mature hair-shaft protein is approximately:
- Cysteine/cystine: 16-18% by mole fraction (sometimes reported as 4-5% by elemental sulfur weight)
- Glutamic acid + glutamine: approximately 13%
- Arginine: approximately 9%
- Serine: approximately 9%
- Leucine: approximately 7%
- Threonine: approximately 7%
- The remaining 35% distributed across other amino acids
By comparison, a typical cytoplasmic protein has cysteine content of 1-2%, and even insulin (which has six cysteine residues holding together its two chains) is only 7% cysteine. Hair is therefore unusual in cysteine demand by approximately an order of magnitude over the average.
The elemental analysis of intact hair shows approximately 5% sulfur by mass, distributed almost entirely as cysteine and methionine residues in keratin and KAP proteins. Forensic and archaeological studies have used hair sulfur content (and the isotopic ratio of S-34/S-32) to infer dietary patterns and geographic origin of human and animal remains. Modern food forensics uses hair sulfur isotope analysis to assess whether livestock were fed plant-protein-dominant or animal-protein-dominant diets.
The clinical extension of this elemental analysis is that hair mineral analysis (HMA) is sometimes promoted as a tool to assess sulfur amino acid status. The evidence base for this is weak — hair sulfur content is dominated by structural keratin and is relatively insensitive to short-term dietary changes. More informative are direct measures: serum free cysteine, fasting plasma methionine, fasting homocysteine, and clinical evaluation of hair shaft quality (cross-sectional area, breakage pattern, growth rate).
Methionine as the Limiting Amino Acid
The concept of a "limiting amino acid" comes from agricultural and nutritional science. A dietary protein source is described as "limiting" for the amino acid that is present in the smallest amount relative to the requirements for human nutrition. The other amino acids may be abundant, but the limiting amino acid sets the ceiling on how much protein synthesis can proceed before that one amino acid runs out, regardless of the abundance of the others.
The textbook examples are:
- Methionine is the limiting amino acid in essentially all legume proteins — beans (black, pinto, kidney, navy, lima), peas, lentils, chickpeas, soybeans (somewhat less so). The methionine content of legume protein is typically 1.0-1.3%, compared to a human reference requirement of approximately 2.5% methionine + cysteine in the ideal protein pattern. Lysine in legumes is high, leucine is adequate, but methionine is the bottleneck.
- Lysine is the limiting amino acid in essentially all grain proteins — wheat, rice, corn, oats. The lysine content of grain protein is typically 1.5-3.0%, compared to a human reference requirement of approximately 5.8% lysine. Methionine in grains is adequate but lysine is the bottleneck.
- Tryptophan can be limiting in corn-dominated diets — the historical pellagra epidemic in the American South was driven by maize-dominated diets that were both niacin-poor (the maize-bound niacin is unavailable without alkali treatment) and tryptophan-limited (tryptophan can be partially converted to niacin in humans).
The complementary protein concept — combining legumes with grains in the same meal or within the same day so that each compensates for the other's limiting amino acid — is the dietary strategy traditionally used in plant-protein-dominant cuisines. Examples include:
- Beans and rice (Latin American, Caribbean)
- Hummus (chickpeas) and pita (wheat) (Middle Eastern)
- Lentils and rice or chapati (South Asian)
- Tofu (soy) and rice (East Asian)
- Peanut butter (legume) and bread (grain) (American)
- Beans and corn tortilla (Mexican)
These combinations produce a protein with a more balanced essential amino acid pattern than either source eaten alone, and Frances Moore Lappé's 1971 book "Diet for a Small Planet" popularized the concept that combining required eating both items in the same meal. Later research (particularly the FAO 1985 consultation and subsequent updates) showed that combining within the same day is sufficient because the body maintains an amino acid pool with several hours of buffering capacity. The exact-meal-pairing dogma turned out to be unnecessary, but the day-level complementation is real and matters for plant-protein-dominant diets.
Protein Quality Scoring: PDCAAS, DIAAS, PER
Three formal scoring systems are used in nutrition science to compare the quality of dietary protein sources:
- Protein Digestibility Corrected Amino Acid Score (PDCAAS) — the standard adopted by FAO/WHO in 1991 and still widely used in food labeling. The score is calculated as (amino acid content of the test protein, divided by amino acid content of the reference pattern) multiplied by digestibility coefficient, with the value capped at 1.0. PDCAAS scores for common foods:
- Egg white: 1.0 (truncated; uncapped would be higher)
- Whey isolate: 1.0 (truncated)
- Casein: 1.0 (truncated)
- Soy protein isolate: 1.0 (truncated, though uncapped is approximately 0.91-0.92, limited by methionine)
- Beef: 0.92
- Wheat gluten: 0.25 (limited by lysine)
- Most legumes: 0.6-0.8 (limited by methionine)
- Most cereal grains: 0.4-0.6 (limited by lysine)
- Digestible Indispensable Amino Acid Score (DIAAS) — the FAO's 2013 update intended to replace PDCAAS. DIAAS uses true ileal digestibility (measured in the small intestine, more accurate than fecal digestibility) and does not truncate scores at 1.0. DIAAS scores tend to be lower for plant proteins than PDCAAS scores because the ileal digestibility numbers are more accurate. For example:
- Milk protein concentrate: 1.18 (uncapped)
- Whey isolate: 1.09
- Soy protein isolate: approximately 0.90-0.98
- Pea protein isolate: approximately 0.65-0.82 (limited by methionine + cysteine)
- Wheat flour: approximately 0.40 (limited by lysine)
- Protein Efficiency Ratio (PER) — an older biological assay measuring weight gain per gram of protein consumed in growing rats. Largely replaced by PDCAAS and DIAAS for formal labeling but still cited in some contexts.
The relevant point for our methionine discussion is that all three scoring systems identify methionine-and-cysteine as the limiting amino acid in legume-based protein sources, and assign correspondingly lower quality scores. This is a real nutritional fact, not a value judgment about plant vs animal protein. The clinical implication is that people whose protein intake is dominated by legumes need either more total protein (to compensate for the lower quality), or grain complementation (to balance the amino acid pattern), or additional methionine source (eggs, dairy, or a small amount of fish or poultry if dietary preferences allow).
Vegan and Vegetarian Diet Patterns
Vegan and vegetarian dietary patterns have many documented health benefits (favorable cardiovascular risk profile, lower BMI, lower diabetes risk in cohort studies, environmental sustainability arguments). Methionine adequacy is one of the specific nutritional considerations for these patterns. Empirical observations:
- Average methionine intake — vegans consume an average of 0.5-0.8 g/day of methionine, compared to omnivores at 1.5-2.5 g/day. Lacto-ovo vegetarians (who include dairy and eggs) average 1.0-1.5 g/day, intermediate between vegans and omnivores. The vegan average is below the WHO methionine + cysteine recommendation for some adults (approximately 1.0-1.3 g/day combined for a 70 kg adult).
- Plasma methionine and cysteine — vegans typically have measurably lower fasting plasma methionine and cysteine concentrations than omnivores, in the 15-30% range. This is biochemically consistent with their lower intake but is not necessarily clinically symptomatic.
- IGF-1 and other markers — lower methionine intake is associated with lower IGF-1, which is the proposed mechanism behind the longevity hypothesis (lower IGF-1 is associated with longer lifespan in cohort studies).
- Hair, nail, and skin quality — the clinical observation in integrative-medicine practice is that vegan patients more often present with concerns about hair quality, hair shedding, brittle nails, and dry skin than mixed-diet patients. The mechanism is plausibly inadequate sulfur amino acid intake feeding inadequate cysteine for keratin synthesis. This pattern is not universal; many vegans have excellent hair and nail quality. It is more common in those with low total protein intake (under 0.8 g/kg/day), high-volume endurance exercise (increased protein turnover), pregnancy or postpartum, or chronic illness.
The practical approach for vegan or vegetarian patients with hair/nail concerns:
- Assess total protein intake — aim for at least 0.8-1.0 g/kg body weight per day, higher (1.2-1.6 g/kg) for active patients, pregnant or postpartum patients, and patients over age 65 with sarcopenia risk
- Optimize protein quality — emphasize sources with relatively high methionine for plant proteins: hemp seeds (good methionine, complete protein), sesame seeds, sunflower seeds, Brazil nuts, oats (relatively rich in methionine for a grain), quinoa, and soy products (soy is the highest-quality plant protein, with DIAAS around 0.9)
- Add complementary patterns — combine legumes with grains, seeds, or nuts within the day
- Consider quality plant-protein supplements — soy isolate, pea protein with rice, or hemp protein concentrate
- Optional cysteine support — NAC 600 mg/day or supplemental L-cysteine 500-1000 mg/day for short-term repletion in vegan patients with documented low protein status and hair/nail concerns
- Address related deficiencies — vegan diets carry structural risk for vitamin B12, vitamin D, omega-3 EPA/DHA (algae-derived is the vegan-appropriate source), zinc, iron, iodine, and calcium. A vegan-appropriate multivitamin plus B12 plus algae omega-3 covers most of this.
This is not an argument against vegan or vegetarian eating. It is a recognition that nutrient adequacy in plant-protein-dominant diets requires more planning than in mixed-diet patterns, and that hair/nail quality is a sensitive early clinical signal of marginal sulfur amino acid intake.
Clinical Signs of Sulfur Amino Acid Deficiency
Marginal sulfur amino acid intake produces a recognizable but non-specific clinical picture in adult patients:
- Hair — thinning hair, diffuse shedding (telogen effluvium pattern, with increased anagen-to-telogen conversion), dry and lusterless texture, brittle and breaking easily, reduced length growth rate, mid-shaft breakage that does not reach maximum length, premature graying (a contested claim with mixed evidence but biochemically plausible because melanocytes depend on methionine for tyrosine pathway support and on glutathione for oxidative protection of the melanin-synthesis enzyme tyrosinase)
- Nails — brittle nails (onychorrhexis, longitudinal ridging), splitting nails (onychoschizia), slow growth, opaque or whitish discoloration, pitting (more characteristic of psoriasis or alopecia areata), spoon-shaped or koilonychia (more typical of iron deficiency but can be seen)
- Skin — dry and scaling skin, reduced elasticity, slow wound healing, increased susceptibility to UV damage, eczematous patches, particularly on the extremities
- Systemic — fatigue (multifactorial; methionine pathway support of creatine, carnitine, and SAMe overlap), reduced exercise tolerance, mood changes, increased susceptibility to infection (from glutathione/immune effects), elevated homocysteine
The differential diagnosis for hair and nail concerns in clinical practice is broad and includes iron deficiency (especially ferritin under 50 ng/mL), thyroid dysfunction (both hypo- and hyperthyroidism), zinc deficiency, vitamin D deficiency, biotin deficiency (uncommon but classic textbook association with hair and nail brittleness), essential fatty acid deficiency, severe protein-calorie undernutrition, telogen effluvium from postpartum or post-illness or post-stress states, androgenetic alopecia, alopecia areata, traction alopecia, and certain medication side effects. A thorough work-up before attributing hair/nail concerns to sulfur amino acid status should include:
- Complete blood count, ferritin, iron studies
- TSH, free T4 (and free T3 if symptomatic)
- 25-hydroxyvitamin D
- Comprehensive metabolic panel including total protein and albumin
- Fasting homocysteine
- Serum zinc
- RBC magnesium
- Optional: serum biotin, free fatty acid panel, sex hormone panel if androgenetic pattern suspected, scalp dermatology evaluation if pattern unclear
Methionine-pathway support is appropriate adjunctive intervention alongside addressing whatever primary deficiency or dermatologic condition is identified.
Nail Disorders and Methionine Status
Nail disorders associated with methionine and cysteine status include:
- Brittle nail syndrome — the most common nail complaint in adult dermatology practice, affecting approximately 20% of adults at some point. Classified as fragilitas unguium when isolated, or as brittle nails secondary to a systemic condition. Sulfur amino acid status, biotin status, hydration of the nail plate, repeated wet-dry cycling exposure (frequent hand washing, restaurant/medical/cleaning occupations), and certain nail-care products all contribute.
- Onychoschizia (lamellar splitting) — horizontal layered splitting of the distal nail plate. Strongly associated with chronic occupational wet-dry cycling and sometimes with sulfur amino acid status.
- Onychorrhexis (longitudinal ridging) — vertical ridges running from cuticle to tip. Increasingly prominent with age and often without underlying systemic cause, but can be exacerbated by sulfur amino acid inadequacy.
- Beau's lines — transverse depressions reflecting temporary growth disruption (severe illness, chemotherapy, severe nutrient deficit). Specific date can be inferred from the position of the line and the known nail growth rate (approximately 0.1 mm/day for fingernail, 0.03 mm/day for toenail).
- Koilonychia (spoon nails) — concave or spoon-shaped nail. Classic association with severe iron deficiency anemia but also reported with severe protein malnutrition.
- Mees' lines (transverse white lines) — classically associated with arsenic poisoning, thallium poisoning, and severe systemic illness. The toxicology component links back to the methionine-arsenic methylation discussion.
The supplementation evidence for nail disorders is mixed. Biotin (2.5-5 mg/day) has been studied in brittle nail syndrome with some positive trials, though the evidence base is weak and many of the positive trials are small and uncontrolled. Methionine-and-cysteine supplementation specifically for nail disorders has been less studied but is biologically reasonable in patients with documented marginal protein intake or vegan dietary patterns. The product category "hair, skin, nail" combines biotin, sometimes silica, zinc, vitamin C, B-complex, and sometimes cysteine or MSM. Effect sizes for any of these in isolated nail disorders are small to modest in controlled studies.
Hair Loss Conditions and Methionine
Hair loss is a complex topic with many causes that are not primarily nutritional, but the nutritional component is real and often partially addressable. Major categories:
- Androgenetic alopecia (male and female pattern hair loss) — the most common cause. Pattern follows characteristic distribution (vertex and frontal recession in men; diffuse central thinning in women) and is mediated by genetic susceptibility plus androgen sensitivity (dihydrotestosterone effects on follicle miniaturization via the type II 5-alpha reductase enzyme). Standard treatments are topical minoxidil (Rogaine), oral finasteride or dutasteride (men, and some women), low-level laser therapy, platelet-rich plasma (PRP) injections, and hair transplantation. Methionine and sulfur amino acid optimization is supportive (provides the building blocks for any remaining functional follicles to produce optimal-quality hair shaft) but does not reverse the underlying miniaturization process.
- Telogen effluvium — diffuse, reversible shedding of hair following a triggering event (postpartum, high fever, severe illness, surgery, severe psychological stress, sudden dietary change, certain medications). Onset is typically 2-4 months after the trigger as the synchronously shifted follicles complete telogen and shed. Spontaneous recovery within 6-12 months is typical. Nutritional optimization (protein adequacy, iron repletion if ferritin under 50 ng/mL, vitamin D adequacy, B-complex sufficiency, sulfur amino acid adequacy) supports recovery.
- Alopecia areata — autoimmune patchy hair loss. Modern treatments include topical and intralesional corticosteroids, topical immunotherapy, oral JAK inhibitors (newer therapy class with substantial efficacy in moderate to severe cases). Nutritional optimization is supportive but not primary.
- Traction alopecia — from tight hairstyles, extensions, weaves. Resolved by avoiding the inciting hair-care practice.
- Hair loss from severe restrictive dieting — rapid weight loss (more than 1 kg/week sustained) commonly triggers telogen effluvium. Bariatric surgery patients are at structural risk and routinely advised to take protein supplements and multivitamins.
- Hair loss from specific medications — chemotherapy (anagen effluvium), certain immunosuppressants, retinoids in high doses, certain antidepressants, certain antihypertensives, certain anticoagulants. Hair regrows after medication cessation in most cases.
- Hair loss from iron deficiency — ferritin under 50 ng/mL is associated with diffuse hair shedding in women, particularly in the setting of heavy menstrual bleeding. Repletion of iron to ferritin 70-100 ng/mL is the standard target.
- Hair loss from thyroid dysfunction — both hypothyroidism (most commonly) and hyperthyroidism. Treatment of the underlying thyroid disorder typically results in hair recovery.
For any clinically significant hair loss, a thorough work-up to identify treatable contributors is appropriate. Nutritional intervention with sulfur amino acid optimization is part of comprehensive management but does not substitute for accurate diagnosis and condition-specific treatment.
Practical Nutritional Stack for Hair, Nails, Skin
A pragmatic nutritional approach for adult patients with hair, nail, or skin quality concerns:
- Dietary foundation — adequate total protein (at least 0.8-1.0 g/kg/day, higher for older or active patients). Include sulfur-rich foods: eggs (1-2 daily for non-vegans), wild fish 2-3 times weekly, sunflower and pumpkin seeds, sesame, hemp seeds, Brazil nuts (also for selenium), garlic and onions (allium sulfur compounds), cruciferous vegetables (broccoli, Brussels sprouts, kale for sulforaphane and cysteine).
- L-methionine and L-cysteine — for patients with documented low intake or vegan diets, supplemental L-methionine 500 mg/day or L-cysteine 500-1000 mg/day for 8-12 weeks is reasonable. N-acetylcysteine 600 mg twice daily is more commonly used and has better bioavailability than free cysteine.
- Biotin — 2.5-5 mg/day for brittle nail syndrome or hair shedding. Caution: high-dose biotin interferes with multiple laboratory assays including troponin (false negative in possible heart attack), TSH (false low), and ferritin. Stop biotin at least 3-7 days before lab tests.
- Zinc — 15-30 mg/day with food. Higher doses (50-75 mg) can be used short-term for documented zinc deficiency but require copper monitoring. Zinc is a cofactor for keratinocyte differentiation and protein synthesis.
- Iron — only if ferritin under 50 ng/mL or hemoglobin low. Iron bisglycinate 25-50 mg elemental iron at bedtime with vitamin C, away from coffee/tea/calcium.
- Vitamin D — aim for 25(OH)D of 40-60 ng/mL. Typical dose 2000-5000 IU/day depending on baseline.
- B-complex — methylated forms (L-methylfolate, methylcobalamin, P5P) are preferred. Supports the methionine cycle and provides biotin alongside other B vitamins.
- Silica — 5-20 mg/day of bioavailable silica (orthosilicic acid or choline-stabilized silica) has some evidence for hair tensile strength and nail brittleness improvement in small trials.
- Collagen peptides — 10-20 g/day of hydrolyzed collagen. Provides glycine, proline, and hydroxyproline that support extracellular matrix turnover. Some hair/nail/skin appearance benefit in commercial trials with the caveat that most are industry-sponsored.
- MSM (methylsulfonylmethane) — 1000-3000 mg/day. Provides bioavailable sulfur; some clinical use for hair, skin, and joint indications with modest evidence base.
- Omega-3 EPA/DHA — 1000-2000 mg/day combined EPA + DHA. Supports skin barrier function and reduces low-grade inflammation that contributes to telogen effluvium and skin dryness.
The full stack is not necessary for everyone — the prescription should be matched to the patient's documented deficiencies and dietary pattern. A typical entry-level approach for an otherwise healthy adult vegetarian with hair quality concerns would be a quality methylated B-complex, NAC 600 mg/day, biotin 2.5 mg/day, zinc 15 mg/day, vitamin D to documented adequacy, and protein/dietary optimization. Reassess at 12-16 weeks (the timeline for new keratin to grow into the visible hair shaft).
Cautions in Hair/Nail Supplementation
- Biotin and lab interference — high-dose biotin (5 mg/day or more) interferes with streptavidin-biotin-based laboratory assays widely used for troponin, TSH, T4, T3, vitamin D, parathyroid hormone, ferritin, and others. False-negative or false-low values can have serious clinical consequences (missed heart attack diagnosis is the highest-stakes example). Stop biotin at least 3-7 days before any lab work; some assays require longer washout. The FDA has issued specific safety communications on this.
- Zinc and copper — chronic high-dose zinc (above 40 mg/day) can produce copper deficiency through competitive absorption interference. Copper deficiency presents with anemia, neutropenia, and (rarely) a myelopathy that mimics B12 deficiency. Match zinc supplementation with copper 1-2 mg/day if dose exceeds 40 mg/day or duration exceeds 8 weeks.
- Iron overload risk — do not supplement iron without documented deficiency. Hereditary hemochromatosis (HFE gene mutations) is common (carrier frequency around 10% in Northern European ancestry, homozygote frequency around 1 in 200-400) and iron supplementation in these patients accelerates the iron-overload pathology. Check ferritin and transferrin saturation before initiating iron.
- Collagen and amino acid composition — collagen is not a complete protein (low in tryptophan and methionine). Collagen peptides should be in addition to, not in place of, complete-protein meals.
- Methionine supplementation for vegan patients — straightforward L-methionine supplementation in vegan patients is generally well tolerated but can acutely raise homocysteine if B12 status is also marginal (a common combination in vegans). Pair methionine supplementation with methylcobalamin B12 1000 mcg/day and methylfolate 400-800 mcg/day.
- Hair loss specialists — significant hair loss that does not respond to a reasonable nutritional optimization trial warrants dermatology referral with hair specialist (trichologist) interest. Scalp biopsy, trichoscopy, and condition-specific treatments (oral or topical) may be needed for accurate diagnosis and management.
- Marketing claims — the hair/skin/nail supplement category is heavily marketed with weak evidence. Skepticism toward dramatic claims is warranted. Documented nutritional repletion has modest but real effects; supplements promising rapid transformation are overselling.
Key Research Papers
- Schweizer J et al. (2007). New consensus nomenclature for mammalian keratins. Journal of Cell Biology. — PubMed
- Rogers MA et al. (2006). Human hair keratin-associated proteins (KAPs). International Review of Cytology. — PubMed
- Robbins CR (2012). Chemical and Physical Behavior of Human Hair, 5th edition. (foundational text on hair keratin chemistry, cysteine content, and disulfide bonding) — PubMed
- Wolfram LJ (2003). Human hair: a unique physicochemical composite. Journal of the American Academy of Dermatology. — PubMed
- Stipanuk MH (2004). Sulfur amino acid metabolism: pathways for production and removal of homocysteine and cysteine. Annual Review of Nutrition. — PubMed
- Schaafsma G (2000). The protein digestibility-corrected amino acid score. Journal of Nutrition. — PubMed
- Mathai JK, Liu Y, Stein HH (2017). Values for digestible indispensable amino acid scores (DIAAS) for some dairy and plant proteins. British Journal of Nutrition. — PubMed
- Young VR, Pellett PL (1994). Plant proteins in relation to human protein and amino acid nutrition. American Journal of Clinical Nutrition. — PubMed
- Mahajan VK et al. (2008). Brittle nail syndrome: a clinical and dermoscopic study. Indian Journal of Dermatology, Venereology and Leprology. — PubMed
- Goluch-Koniuszy ZS (2016). Nutrition of women with hair loss problem during the period of menopause. Przeglad Menopauzalny. — PubMed
- Rushton DH (2002). Nutritional factors and hair loss. Clinical and Experimental Dermatology. — PubMed
- Trueb RM (2016). Serum biotin levels in women complaining of hair loss. International Journal of Trichology. — PubMed
PubMed Topic Searches
- PubMed: Hair keratin sulfur content
- PubMed: Methionine as limiting amino acid
- PubMed: PDCAAS and DIAAS scoring
- PubMed: Vegan amino acid intake
- PubMed: Biotin and brittle nails
- PubMed: Collagen and hair/nail/skin
Connections
- Methionine Overview
- Methionine Benefits Hub
- Methylation and SAMe
- Methionine for Liver Health
- Methionine for Detoxification
- Cysteine
- Lysine
- Glycine
- N-Acetylcysteine (NAC)
- NAC & Glutathione
- Sulfur
- Zinc
- Selenium
- Collagen
- Vitamin B12
- Vitamin D3
- Eggs
- All Amino Acids