Glutamic Acid, Umami, and MSG — The Long History of a Misunderstood Molecule
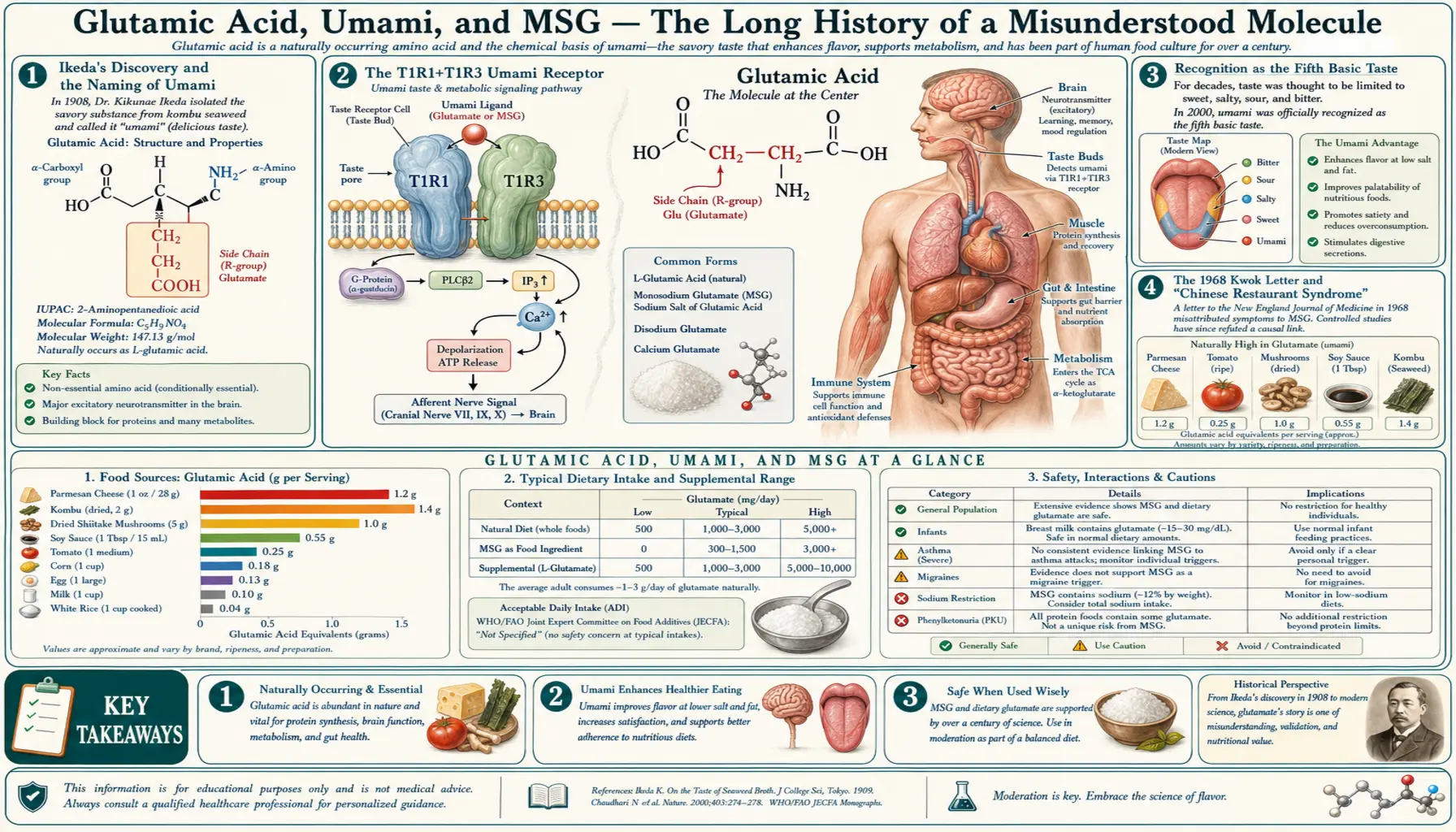
In 1908, the Tokyo Imperial University chemist Kikunae Ikeda isolated glutamic acid from kombu seaweed broth and identified it as the chemical responsible for the savory, broth-like taste he called umami — the "fifth taste" beyond sweet, sour, salty, and bitter. Within a year, Ikeda and his collaborator Saburosuke Suzuki had patented the manufacturing process for monosodium glutamate (MSG) and founded the Ajinomoto Company, which still produces most of the world's MSG today. For sixty years, MSG was an unremarkable global ingredient. Then in 1968, a single letter to the editor of The New England Journal of Medicine by Robert Ho Man Kwok — describing a vague symptom complex he attributed to monosodium glutamate in Chinese restaurant food — launched what became one of the longest-running food safety panics in modern history, complete with the now-discredited term "Chinese Restaurant Syndrome." Decades of progressively better-controlled double-blind trials have failed to reproduce a consistent MSG-symptom relationship in the general population. The FDA, EFSA, JECFA, FAO/WHO, and essentially every major food safety body now classify MSG as Generally Recognized as Safe (GRAS), and in 2020 a coalition of Asian-American chefs, scientists, and advocates persuaded Merriam-Webster to update its definition of "Chinese Restaurant Syndrome" to acknowledge its xenophobic origins. The biology is straightforward: MSG is identical to the free glutamate that occurs naturally in tomatoes, Parmesan cheese, mushrooms, anchovies, breast milk, and the digestive tracts of every human. The blood-brain barrier blocks dietary glutamate from entering the brain in any meaningful quantity. The umami taste receptor T1R1+T1R3 is one of the body's sophisticated signaling systems for sensing protein content in food. This deep dive walks through the discovery, the controversy, the receptor biology, the natural high-glutamate foods, and the modern scientific consensus.
Table of Contents
- Ikeda's Discovery and the Naming of Umami
- The T1R1+T1R3 Umami Receptor
- Recognition as the Fifth Basic Taste
- The 1968 Kwok Letter and "Chinese Restaurant Syndrome"
- Decades of Poor Science
- The Modern Scientific Consensus
- FDA GRAS Status and Global Regulatory Position
- MSG and Migraine — A Real but Narrow Signal
- Why Dietary MSG Does Not Cause Brain Excitotoxicity
- Natural High-Glutamate Foods
- Culinary Applications and Sodium Reduction
- Labeling and "Hidden Glutamates"
- Key Research Papers
- Connections
- Featured Videos
Ikeda's Discovery and the Naming of Umami
Kikunae Ikeda was a German-trained physical chemist at Tokyo Imperial University in the early 1900s when he noticed that the taste of dashi — the Japanese broth made from dried bonito flakes and kombu seaweed — was distinct from the four traditionally recognized tastes of sweet, sour, salty, and bitter. He set out to identify the molecule responsible. After processing 40 kilograms of dried kombu, he isolated 30 grams of brown crystals in 1908 and identified them as glutamic acid. The sodium salt — monosodium glutamate — provided a far stronger and more soluble form of the same taste.
Ikeda coined the term umami for the taste — from the Japanese words umai (delicious) and mi (taste). He filed the manufacturing patent in 1908 and partnered with iodine manufacturer Saburosuke Suzuki to commercialize the product under the brand name Aji-no-moto (Japanese for "essence of taste"). The first commercial MSG went on sale in 1909, and the Ajinomoto Company remains the world's largest MSG manufacturer over a century later.
Two important contextual notes:
- Ikeda's discovery did not invent the umami taste; he merely identified its chemical basis. Cooks across the world had been intensifying umami for millennia — fish sauces in Southeast Asia, soy sauce and miso in East Asia, garum and aged cheeses in the Mediterranean, slow-roasted bones in French and Chinese cuisine, sun-dried tomatoes in Italy. These traditional preparations all work by enzymatic and microbial breakdown of bound glutamate in protein, releasing the free glutamate that activates the umami receptor.
- Ikeda's claim that umami was a distinct fifth taste was not universally accepted in Western food science for nearly ninety years. The Japanese tradition retained it, and the Chinese tradition called it xian wei, but Western textbooks continued to list four basic tastes well into the 1990s. The discovery of the specific umami taste receptor in 2000 (Chaudhari et al., Nature) settled the question scientifically — there is a dedicated molecular receptor for glutamate on the tongue, distinct from the receptors for sweet, sour, salty, and bitter.
The T1R1+T1R3 Umami Receptor
The dedicated taste receptor for L-glutamate is a heterodimer of two G-protein coupled receptor subunits: T1R1 (TAS1R1) and T1R3 (TAS1R3). The same T1R3 subunit pairs with T1R2 to form the sweet-taste receptor, and with T1R1 to form the umami-taste receptor. This combinatorial logic is similar to other GPCR receptor families.
The T1R1+T1R3 umami receptor has a fascinating positive cooperativity feature: the umami response is dramatically enhanced (synergistically, by 10- to 30-fold or more) when L-glutamate is combined with 5'-ribonucleotides — specifically inosine 5'-monophosphate (IMP, abundant in meat and bonito flakes) or guanosine 5'-monophosphate (GMP, abundant in dried shiitake mushrooms). This synergy is the chemical reason traditional broths use both kombu (glutamate source) and bonito (IMP source), why dashi tastes so much richer than either ingredient alone, and why MSG combined with disodium inosinate / guanylate (a common food-industry blend marketed as "I+G") tastes more intensely savory than MSG alone at the same total nucleotide concentration.
The mechanism: IMP and GMP bind to a separate site on the T1R1 subunit and stabilize the active conformation of the dimer, dramatically increasing its affinity for glutamate. The synergy is so pronounced that it served as one of the key pieces of evidence that umami is a distinct taste with its own molecular machinery, not just a modification of salt or sweet perception.
The T1R1+T1R3 receptor is expressed in three locations:
- Type II taste receptor cells in fungiform, foliate, and circumvallate papillae on the tongue. The classical "taste bud" location.
- Enteroendocrine cells throughout the gastrointestinal tract. These cells release hormones (CCK, GLP-1, PYY, ghrelin) in response to luminal nutrients. Luminal glutamate sensing via T1R1+T1R3 triggers cephalic-phase digestive responses (gastric acid secretion, pancreatic enzyme release, gut motility) and produces the satiety-promoting effect of umami-rich meals.
- Vagal afferent fibers in the gut, which relay glutamate-sensing signals to the brainstem and contribute to the satiety and pleasure response to high-protein foods.
The evolutionary logic is clean: umami is the taste of protein. Free glutamate signals the presence of broken-down protein (digestion-ready, easily absorbable amino acids), and the body's detection apparatus is wired both to recognize and to reward consumption of protein-containing foods through this receptor family. The high concentration of free glutamate in human breast milk (the highest free amino acid concentration in breast milk, at approximately 1500 micromolar) suggests that babies are wired from birth to recognize and prefer umami flavors as a developmental cue to seek protein-dense food sources.
Recognition as the Fifth Basic Taste
The four traditional tastes — sweet, sour, salty, bitter — date back to ancient Greek physiology (Aristotle wrote about them in De Anima). They became canonized in Western nutrition and physiology textbooks through the 19th and 20th centuries. Umami was either dismissed as a Japanese cultural quirk or filed under some hybrid of "salty" and "savory" by Western food scientists.
The case for umami as a distinct basic taste rested on several lines of evidence accumulated through the late 20th century:
- Phenomenological distinctness — trained tasters could reliably distinguish glutamate solutions from salty, sweet, sour, and bitter solutions, and the umami descriptor was consistent across cultures.
- Independence from sodium — the umami taste of free glutamate persists when sodium is replaced by potassium, calcium, or even when administered as glutamic acid itself, ruling out a purely salt-perception explanation. (The MSG form is preferred commercially because sodium is much more palatable and soluble than calcium or potassium glutamates.)
- Cross-cultural recognition — cultures with no exposure to MSG could be trained to identify and label umami in foods like ripe tomato, mushroom broth, and aged cheese.
- The IMP/GMP synergy — the dramatic enhancement of umami by ribonucleotides has no parallel in salt or sweet perception.
- The 2000 Chaudhari et al. discovery — the identification of the T1R1+T1R3 receptor provided the definitive molecular evidence for a dedicated glutamate-sensing taste machinery on the tongue. After this paper, the resistance to recognizing umami in Western food science evaporated. By 2002, the basic tastes list was being updated in textbooks; by 2010, umami was standard curriculum in introductory physiology classes.
A more recent candidate — oleogustus, the taste of free fatty acids — is now being proposed as a sixth basic taste, with reasonable but not yet definitive evidence. Calcium and water have also been proposed as candidate basic tastes by some researchers. The conventional list of five is likely to expand in the coming decades.
The 1968 Kwok Letter and "Chinese Restaurant Syndrome"
On April 4, 1968, the New England Journal of Medicine published a letter from Robert Ho Man Kwok, a Chinese-American physician working at the Maryland National Biomedical Research Foundation. The letter, titled "Chinese Restaurant Syndrome," reported that Dr. Kwok experienced "numbness at the back of the neck, gradually radiating to both arms and the back, general weakness and palpitation" after eating at Chinese restaurants in the United States. He speculated several possible causes, including soy sauce, alcohol used in cooking, monosodium glutamate, and the sodium load of the meals.
The letter was 257 words long. It was a casual observation, not a clinical study. There were no controls, no exposure quantification, no biochemical measurements. It would not have qualified as a research letter today. But it landed at exactly the wrong moment, in exactly the wrong cultural context. The 1965 Hart-Celler Act had just opened large-scale Chinese immigration to the United States after almost a century of Chinese exclusion laws, and Chinese restaurants were proliferating in American cities. The country was primed to be suspicious of unfamiliar foreign food.
The next few weeks brought a flood of additional letters to the NEJM from physicians and laypeople reporting similar symptom complexes after Chinese meals. Several major news outlets covered the story. By the end of 1969, "Chinese Restaurant Syndrome" had entered the medical and popular lexicon as a real diagnostic entity, with monosodium glutamate as the presumed culprit. The New York Times published a sensationalized story. The MSG industry went into damage-control mode.
What followed over the next five decades was an ironic study in how a poorly-controlled anecdote, amplified by xenophobic cultural assumptions, can become entrenched in the public consciousness for generations — in a way that no amount of subsequent rigorous research can fully dislodge.
In 2018, a survey of historical evidence by Howard Markel suggested that Kwok's original letter may have been intended as a joke or satire, sent on a whim. Dr. Kwok died in 2014. The "Chinese Restaurant Syndrome" entry in the Merriam-Webster Dictionary was finally updated in 2020 after a campaign led by chef Eddie Huang and the Ajinomoto Company to acknowledge the term's origins in racism.
Decades of Poor Science
The first wave of MSG safety studies in the 1970s was methodologically poor by modern standards. Olney's 1969 paper in Science — "Brain lesions, obesity, and other disturbances in mice treated with monosodium glutamate" — showed that very high doses of glutamate injected subcutaneously into neonatal mice produced selective neuronal death in brain regions outside the blood-brain barrier. The paper was scientifically rigorous within its parameters but was immediately misinterpreted by the press and the public as showing that dietary MSG caused human brain damage. The actual relevance to human dietary exposure (oral, in adults, with intact BBB) was tenuous at best — the doses required to produce the lesions in neonatal mice corresponded to enormous amounts in adult humans, and the BBB-bypass route was impossible to replicate dietarily. But the damage was done.
Subsequent challenge studies in the 1970s and 1980s were often badly designed: open-label, often without proper placebo control, often using doses far above any realistic dietary intake, and often relying on self-report of subjective symptoms. The methodology was so loose that the studies tended to find what the researchers (or the subjects) expected to find. Symptom reports correlated more with whether subjects believed they had been given MSG than with actual exposure.
Better-designed studies emerged in the 1990s and 2000s. The Geha 2000 study (Federation of American Societies for Experimental Biology, FASEB) used a rigorous protocol: double-blind, placebo-controlled, with self-identified MSG-sensitive individuals as subjects. Even in this carefully selected group of self-reported MSG-sensitive subjects, only a minority reacted to MSG when given without their knowledge, and the reactions were inconsistent on rechallenge. The conclusion was that for the small minority of individuals who appear to be genuinely sensitive to high doses of pure MSG taken on an empty stomach, the reaction tends to be mild, brief, and self-limited — with no evidence of any serious or lasting harm.
The 1995 FASEB report to the FDA, the 1991 European Food Safety Authority review, and the 2017 JECFA (Joint FAO/WHO Expert Committee on Food Additives) reaffirmation all converged on the same conclusion: MSG is safe for the general population at typical dietary intake levels, and the small fraction of individuals who report sensitivity should simply avoid it.
The Modern Scientific Consensus
As of the mid-2020s, the consensus across regulatory and scientific bodies is straightforward:
- MSG is the sodium salt of glutamic acid, identical to the glutamate naturally present in many foods. The body cannot distinguish MSG-derived glutamate from naturally-occurring food glutamate — both are metabolized identically.
- MSG is Generally Recognized as Safe (GRAS) by the FDA, with no acceptable daily intake limit specified (the JECFA originally set an ADI in the 1970s but withdrew it in 1988 as unnecessary).
- Population-level placebo-controlled trials have not demonstrated a consistent symptom syndrome attributable to MSG. A minority of self-identified sensitive individuals may experience mild, brief, self-limited symptoms (headache, flushing, sweating) at high doses (3 grams or more) of pure MSG taken on an empty stomach. These reactions are not seen at typical dietary intake levels with food.
- The early animal studies showing neuronal damage from injected or gavaged glutamate at extremely high doses are not relevant to oral dietary exposure in adults with intact blood-brain barriers.
- Glutamate in the diet has minimal effect on brain glutamate concentrations because the blood-brain barrier severely restricts dietary glutamate entry and because gut glutamate is largely metabolized by enterocytes before it reaches the systemic circulation.
- The "Chinese Restaurant Syndrome" framing is now recognized as having had racist origins and is no longer used in scientific or medical literature.
This does not mean that everyone tolerates MSG identically — food sensitivities of all kinds exist on a spectrum, and a small fraction of people will report subjective discomfort after MSG-containing foods just as they might after dairy, gluten, histamine-rich foods, or any other dietary component. The naturopathic position is to respect individual variation: if a patient reliably feels worse after meals containing MSG (or any other ingredient), avoiding it is reasonable. But there is no evidence that population-level avoidance of MSG provides health benefit, and the cumulative cultural impact of the MSG panic has done substantial damage to perception of Chinese cuisine and to Asian-American food businesses.
FDA GRAS Status and Global Regulatory Position
MSG holds GRAS (Generally Recognized as Safe) status with the U.S. FDA, granted in 1958 when the FDA created the GRAS category for food ingredients with a long history of safe use. GRAS status was reaffirmed by the FDA Federation of American Societies for Experimental Biology (FASEB) reports in 1980 and 1995. The FDA does require that monosodium glutamate be declared on food ingredient labels when added — but does not require disclosure of MSG's presence when it occurs naturally in ingredients like hydrolyzed soy protein, yeast extract, or autolyzed yeast.
Internationally:
- European Food Safety Authority (EFSA) — in 2017 set an Acceptable Daily Intake (ADI) of 30 mg/kg body weight/day for glutamic acid and its salts. Above this level, EFSA noted that some sensitive individuals might experience symptoms; below it, no safety concerns. Most population-level intake of MSG is well below this threshold.
- JECFA (Joint FAO/WHO Expert Committee on Food Additives) — "ADI not specified," meaning that, on the basis of available data, the total dietary intake of MSG arising from its use at the levels necessary to achieve the desired technological effect and from its acceptable background levels in food does not represent a hazard to health.
- Codex Alimentarius Commission — classifies MSG as a permitted food additive (E621 in the European numbering system; INS 621 internationally).
The labeling rules vary by country but generally require declaration when MSG is added to processed foods. In the United States, the "No MSG Added" or "MSG-Free" claims are permitted but tightly regulated — the food must contain no added MSG and must not contain other ingredients that contribute free glutamate (hydrolyzed proteins, autolyzed yeast, soy protein isolate, etc.).
MSG and Migraine — A Real but Narrow Signal
Among the broader population of self-reported MSG-sensitive individuals, the strongest signal in controlled studies is in patients with established migraine disorder. The mechanism is biologically plausible: migraine pathophysiology involves cortical hyperexcitability, possibly mediated by glutamatergic dysfunction, and migraine patients have measurably elevated CSF glutamate concentrations between attacks. In principle, a high dietary load of free glutamate could contribute to triggering an attack in a susceptible individual through subtle changes in peripheral or central glutamate handling, or possibly through trigeminal afferent stimulation in the gut.
The clinical evidence is mixed but suggestive. Some controlled provocation studies in migraine patients have shown increased headache frequency or intensity with high-dose MSG challenge (3-6 grams) compared to placebo. Other studies have failed to show a clear effect. The American Headache Society lists MSG as a possible but not well-established dietary trigger, alongside aged cheeses, nitrates, red wine, and chocolate — all of which are anecdotally reported as triggers in some patients but inconsistently confirmed in controlled studies.
The practical clinical advice for migraine patients: if you reliably notice that MSG-containing foods trigger your headaches, avoiding them is reasonable. There is no need for the general non-migraine population to restrict MSG. For migraine prophylaxis, the more impactful interventions are: magnesium (400-600 mg/day), riboflavin (400 mg/day), CoQ10 (100-300 mg/day), regular sleep, adequate hydration, and identifying personal triggers including (if relevant) high free-glutamate foods. See the Migraine page for fuller treatment.
Why Dietary MSG Does Not Cause Brain Excitotoxicity
One of the most enduring misconceptions about MSG is that dietary glutamate causes brain excitotoxicity equivalent to the NMDA-mediated calcium overload seen in stroke or ALS (discussed on the Neurotransmission page). The biology that prevents this is robust and well-characterized:
- Enterocyte first-pass metabolism — the cells lining the small intestine consume an enormous fraction of luminal glutamate as their preferred metabolic fuel. Studies have estimated that 90% or more of orally ingested glutamate is consumed by enterocytes before it ever reaches the portal circulation. The remaining glutamate is largely cleared on first pass through the liver.
- Blood-brain barrier exclusion — the BBB does not have facilitative transporters for glutamate from the blood side. The few small molecule transporters present (LAT1 for large neutral amino acids, EAAT3 expressed in some brain endothelial cells) do not handle glutamate efficiently as a substrate from the peripheral side. The BBB also expresses glutamate transporters on the abluminal (brain) side that remove glutamate from brain extracellular space back into the bloodstream, further protecting the brain from peripheral glutamate fluctuations.
- The brain manufactures its own glutamate — as detailed on the Nitrogen Metabolism page, the brain synthesizes essentially all of its own glutamate from glutamine and alpha-ketoglutarate. The brain's glutamate pool is functionally sealed off from the body's glutamate pool by these multiple layers of protection.
- Compartmentalization within the synapse — even within the brain, glutamate that reaches the synapse is rapidly cleared by astrocyte transporters (EAAT1/2) within milliseconds, preventing extrasynaptic spillover. The brain has many layers of redundant protection against excitotoxic glutamate accumulation.
The result is that even gram-quantity doses of oral MSG produce minimal changes in brain glutamate concentrations in any of the imaging or microdialysis studies that have attempted to measure it. The neonatal mouse subcutaneous injection studies that started the "MSG causes brain damage" narrative have no relevance to oral dietary exposure in adult humans.
There is one important exception: the circumventricular organs (area postrema, arcuate nucleus, organum vasculosum laminae terminalis, subfornical organ, median eminence) are brain regions outside the BBB by design — they need to sample circulating hormones and signal back to the body. These regions are theoretically vulnerable to circulating glutamate fluctuations and were the actual site of Olney's 1969 neuronal lesions in his mouse studies. But adult humans do not develop circumventricular organ lesions from dietary MSG at any realistic intake level, and the clinical relevance of this animal-model finding remains hypothetical.
Natural High-Glutamate Foods
For perspective on dietary glutamate exposure, here is the approximate free-glutamate content of selected common foods (in milligrams per 100 grams, varying with ripeness, preparation, and source):
- Parmigiano-Reggiano (aged 36 months) — ~1200 mg/100g
- Roquefort cheese — ~1280 mg/100g
- Soy sauce — ~500-1100 mg/100g (depending on style)
- Tomato (sun-dried) — ~650 mg/100g
- Anchovies — ~630 mg/100g
- Cured ham (Iberico, prosciutto) — ~340 mg/100g
- Marmite / Vegemite — ~1750 mg/100g (highest of common foods, hence the strong taste)
- Kombu seaweed (dried) — ~2240 mg/100g (Ikeda's original source)
- Walnuts — ~660 mg/100g
- Green peas — ~200 mg/100g
- Tomato (fresh, ripe) — ~140-250 mg/100g
- Mushrooms (shiitake, dried) — ~1060 mg/100g (also high in GMP for the umami synergy)
- Mussels — ~140 mg/100g
- Corn — ~110 mg/100g
- Breast milk — ~22 mg/100g (still the highest free amino acid in breast milk)
By comparison, a single sprinkle of MSG on a dish provides approximately 0.5-1 gram — less free glutamate than 100 grams of Parmesan cheese. Many traditional dishes contain naturally occurring free glutamate well in excess of what a generous MSG addition would provide: a plate of pasta with Parmesan, sun-dried tomatoes, and anchovies; a slow-simmered French onion soup with aged Gruyere; a Vietnamese pho with fish sauce. The body cannot tell the difference between free glutamate from these sources and free glutamate from MSG — they are the same molecule.
Total daily dietary glutamate (free + protein-bound) typically averages 10-20 grams per day in a mixed Western diet, of which roughly 1 gram is free glutamate and the rest is protein-bound. Asian diets traditionally include slightly more free glutamate due to higher use of fermented and dried umami ingredients. The added MSG used in commercial seasoning typically adds 0.3-0.5 grams per serving — a small marginal increase against the natural background.
Culinary Applications and Sodium Reduction
A perhaps surprising public-health application of MSG is for sodium reduction in processed foods. MSG provides intense umami flavor at a much lower sodium content than table salt: by weight, MSG contains approximately 12% sodium, compared to 39% for sodium chloride. The umami taste also has a "saltiness-enhancing" effect, allowing significant reductions in added salt while preserving palatability. Food manufacturers can reduce the sodium content of canned soups, processed meats, snacks, and seasonings by 20-40% by partial substitution of MSG for table salt without consumer detection. Several public health bodies have suggested that strategic MSG use could be part of population-level sodium reduction strategies for cardiovascular disease prevention.
Culinary applications include:
- Soup bases and stocks — a small amount of MSG (1/4 to 1/2 teaspoon per quart) deepens the savory complexity of broths and reduces the need for prolonged reduction or large salt additions.
- Roasted vegetables — a light dusting of MSG before roasting enhances the natural umami of tomatoes, mushrooms, and brassicas.
- Meat marinades and rubs — combined with salt and aromatics, MSG amplifies the savory character of grilled meats.
- Asian cuisine — the traditional and most associated application; standard in many Chinese, Japanese, Korean, Thai, and Vietnamese preparations alongside fish sauce, soy sauce, and miso.
- Savory snacks and seasonings — ranch dressing, taco seasoning, bouillon cubes, chip seasonings, and many other commercial flavor blends rely on MSG or its hidden equivalents.
Chef David Chang and many other contemporary food writers have spent the last decade publicly rehabilitating MSG in Western cuisine, arguing for its legitimate culinary value and against the lingering cultural baggage.
Labeling and "Hidden Glutamates"
U.S. FDA labeling rules require declaration of added monosodium glutamate as "monosodium glutamate" in the ingredient list. However, the rules do not require disclosure of free glutamate that is intrinsic to other ingredients, even when those ingredients are added specifically for their umami-enhancing properties. Common food ingredients that contribute significant free glutamate include:
- Hydrolyzed vegetable protein (HVP), hydrolyzed soy protein, hydrolyzed wheat protein
- Autolyzed yeast extract, yeast extract, yeast nutrient
- Textured vegetable protein (TVP)
- Soy protein isolate, whey protein concentrate
- Sodium caseinate, calcium caseinate
- Maltodextrin (some forms; sourced from hydrolyzed corn)
- Natural flavors (sometimes; not always)
- Bouillon, broth, stock concentrates (especially commercial)
- Soy sauce, fish sauce, tamari, miso, Worcestershire sauce
- Parmesan, aged cheeses, blue cheeses
- Tomato paste, sun-dried tomatoes, ketchup
- Mushroom extracts and concentrates
For consumers who are genuinely MSG-sensitive (a small minority, but real), simply avoiding products labeled "monosodium glutamate" is insufficient — they would also need to avoid the long list above. For the vast majority of consumers, these distinctions are unnecessary. From a population standpoint, the contribution of "hidden glutamates" to total dietary glutamate intake is similar to that of overt MSG — both add to a baseline of 10-20 g/day of glutamate from natural protein sources that the body handles without difficulty.
Key Research Papers
- Ikeda K (1909). On a new seasoning [translated, originally in Japanese, Journal of the Chemical Society of Tokyo]. — PubMed
- Kwok RH (1968). Chinese-restaurant syndrome. NEJM. — PubMed
- Olney JW (1969). Brain lesions, obesity, and other disturbances in mice treated with monosodium glutamate. Science. — PubMed
- Geha RS et al. (2000). Review of alleged reaction to monosodium glutamate and outcome of a multicenter double-blind placebo-controlled study. Journal of Nutrition. — PubMed
- Chaudhari N et al. (2000). A metabotropic glutamate receptor variant functions as a taste receptor. Nature Neuroscience. — PubMed
- Nelson G et al. (2002). An amino-acid taste receptor. Nature. — PubMed
- Beyreuther K et al. (2007). Consensus meeting: monosodium glutamate — an update. European Journal of Clinical Nutrition. — PubMed
- EFSA Panel on Food Additives (2017). Re-evaluation of glutamic acid (E 620), sodium glutamate (E 621), potassium glutamate (E 622), calcium glutamate (E 623), ammonium glutamate (E 624) and magnesium glutamate (E 625) as food additives. EFSA Journal. — PubMed
- Henry-Unaeze HN (2017). Update on food safety of monosodium L-glutamate (MSG). Pathophysiology. — PubMed
- Yamaguchi S, Ninomiya K (2000). Umami and food palatability. Journal of Nutrition. — PubMed
- Stanska K, Krzeski A (2016). The umami taste: from discovery to clinical use. Otolaryngologia Polska. — PubMed
- Mosby's Manual of Diagnostic and Laboratory Tests / Markel H (2018). The history of monosodium glutamate and the Chinese restaurant syndrome label. JAMA. — PubMed
PubMed Topic Searches
- PubMed: MSG safety reviews
- PubMed: Umami taste receptor
- PubMed: Glutamate and migraine
- PubMed: Enterocyte glutamate metabolism
- PubMed: MSG and sodium reduction
Connections
- Glutamic Acid Benefits Hub
- Glutamic Acid Overview
- Neurotransmission
- GABA Production
- Nitrogen Metabolism
- MSG (Toxins Index)
- Tomatoes (Natural Glutamate)
- Mushrooms (Umami + GMP)
- Parmesan Cheese
- Migraine
- Glutamine
- Magnesium
- Hypertension (Sodium Reduction)
- Gut-Brain Axis
- All Amino Acids