Glutamic Acid for GABA Production — The Excitatory-to-Inhibitory Switch
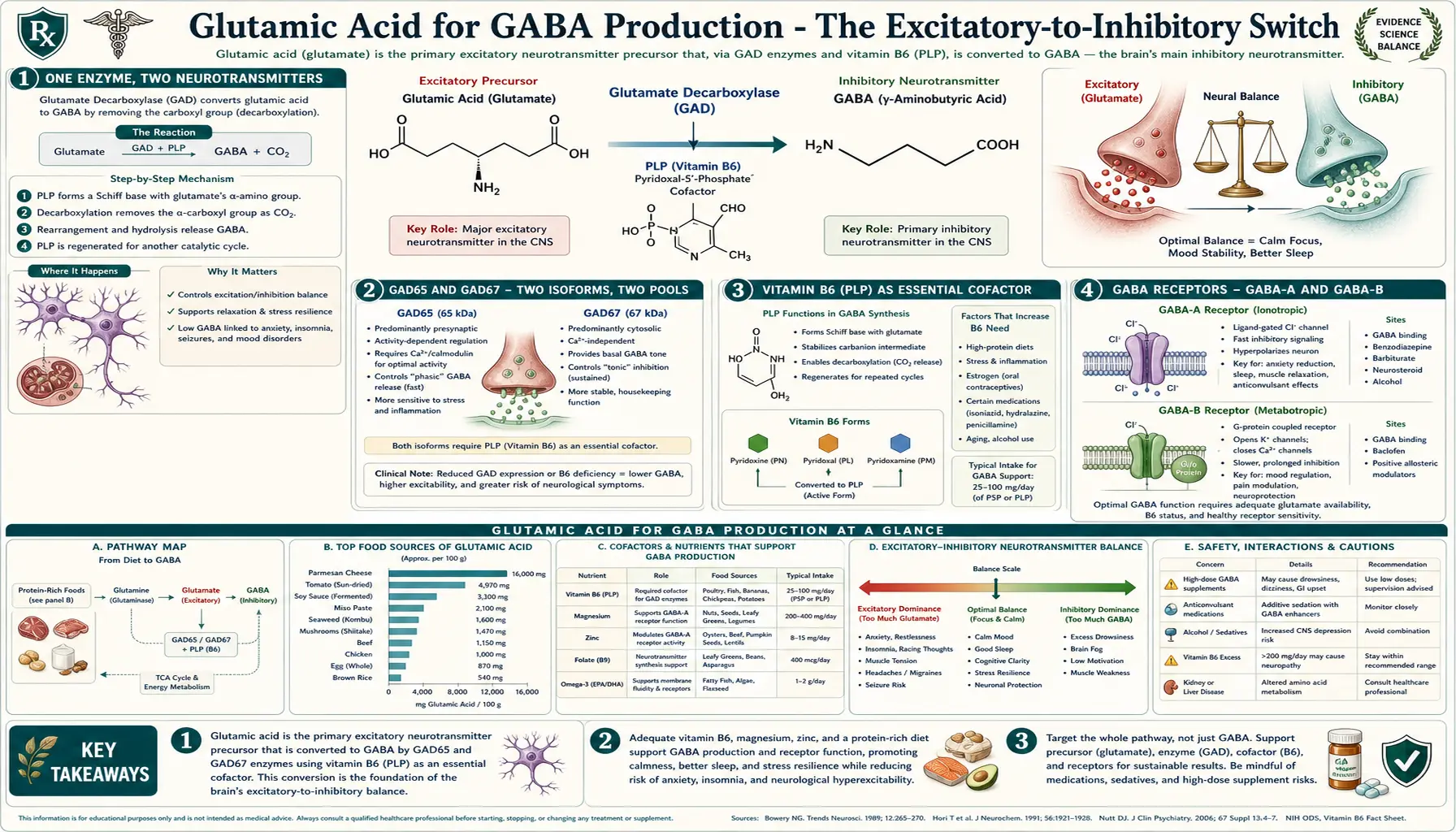
One enzyme — glutamic acid decarboxylase (GAD) — converts the brain's major excitatory neurotransmitter into its major inhibitory neurotransmitter in a single step. By removing a single carboxyl group from glutamate, GAD produces gamma-aminobutyric acid (GABA), which then binds GABA-A and GABA-B receptors throughout the central nervous system to dampen neuronal firing. The reaction is absolutely dependent on pyridoxal 5'-phosphate (PLP), the active form of vitamin B6, as a covalently bound cofactor — making B6 status one of the most direct nutritional determinants of brain excitatory-inhibitory balance. Two GAD isoforms exist: GAD65, concentrated in synaptic terminals and responsible for the rapidly available GABA pool that supports phasic inhibition, and GAD67, distributed throughout the neuronal cytoplasm and responsible for the bulk tonic GABA pool. Both isoforms are targets of autoantibodies in two important autoimmune diseases: stiff-person syndrome (where high-titer anti-GAD65 antibodies are essentially pathognomonic) and a substantial minority of type 1 diabetes (where anti-GAD65 antibodies serve as one of the canonical pre-clinical autoimmune markers, since pancreatic beta cells also express GAD65). This deep dive walks through the chemistry of the GAD reaction, the B6 cofactor mechanism, the regional distribution of GABAergic inhibition, the natural and pharmacological GABA-A modulators (alcohol, benzodiazepines, barbiturates, anesthetics), and the autoimmune disorders that target GAD itself.
Table of Contents
- One Enzyme, Two Neurotransmitters
- GAD65 and GAD67 — Two Isoforms, Two Pools
- Vitamin B6 (PLP) as Essential Cofactor
- GABA Receptors — GABA-A and GABA-B
- Tonic vs Phasic Inhibition
- GABA-A Modulators (Benzos, Barbiturates, Alcohol, Anesthetics)
- Anti-GAD Autoimmunity — Stiff-Person Syndrome and T1DM
- Nutritional Strategies to Support GABA Synthesis
- Does Oral GABA Cross the Blood-Brain Barrier?
- Clinical Applications: Anxiety, Insomnia, Seizures
- Key Research Papers
- Connections
- Featured Videos
One Enzyme, Two Neurotransmitters
The economy of the GABA-synthesizing reaction is one of biology's most elegant pieces of design. The same molecule — glutamate — that 90% of the brain's excitatory synapses use as their messenger is converted, in a single enzymatic step, into the principal inhibitory neurotransmitter. The reaction:
glutamic acid → GABA + CO2
Glutamate has two carboxyl groups (alpha and gamma); GAD removes the alpha-carboxyl, releasing CO2 and leaving GABA, which retains the gamma-carboxyl as part of its name (gamma-aminobutyric acid). The same neuron, the same metabolic precursor pool, the same vesicular machinery — the only thing that distinguishes a glutamatergic excitatory neuron from a GABAergic inhibitory neuron is whether the cell expresses GAD or not. Neurons that express GAD load their synaptic vesicles with GABA (using the vesicular GABA transporter VGAT); neurons that lack GAD load with glutamate (using VGLUT1/2/3).
This binary choice happens during neuronal development. In the cerebral cortex, GABAergic interneurons (about 20% of all cortical neurons) migrate from the medial and caudal ganglionic eminences in the ventral forebrain to populate the dorsal cortex, where they take up residence among the much more numerous glutamatergic pyramidal neurons. The two cell types coexist in a roughly 1:4 ratio in the mature cortex and engage in tightly choreographed back-and-forth signaling that produces the cortex's rich repertoire of oscillations (theta, gamma, beta, alpha rhythms) and the precise spike timing needed for sensory processing and cognition.
Without GAD activity, the entire inhibitory side of the network collapses, and runaway excitation produces seizures. Indeed, the very first inborn error of metabolism shown to cause seizures responsive to vitamin therapy was pyridoxine-dependent epilepsy — a condition where insufficient PLP availability impairs GAD function and produces neonatal seizures that resolve dramatically when high-dose pyridoxine is administered.
GAD65 and GAD67 — Two Isoforms, Two Pools
Mammals express two genes encoding glutamic acid decarboxylase, named for their approximate molecular weights:
- GAD65 (gene: GAD2, chromosome 10p11) is concentrated in nerve terminals, anchored to synaptic vesicle membranes via palmitoylation of its N-terminus. GAD65 binds PLP loosely and reversibly, allowing rapid activation when PLP is available. It is responsible for the synaptic pool of GABA — the rapidly mobilizable, vesicle-loaded GABA that gets released in response to action potentials and mediates fast phasic inhibition.
- GAD67 (gene: GAD1, chromosome 2q31) is distributed throughout the neuronal cytoplasm and binds PLP tightly. It produces the bulk of total brain GABA, supplying the tonic cytoplasmic pool that supports baseline GABAergic tone and is also a metabolic substrate for the GABA shunt (a small-flux side branch of the citric acid cycle).
The two isoforms have markedly different developmental patterns. GAD67 is expressed early and provides the GABA needed for the developing nervous system (where GABA is actually depolarizing and trophic in immature neurons due to a high intracellular chloride concentration that reverses at synaptic maturation). GAD65 expression rises later and reaches adult levels around the time of synapse pruning and circuit refinement, suggesting a role in experience-dependent plasticity. Mice lacking GAD67 die at birth from severe cleft palate (jaw muscle GAD67 is needed for proper palate fusion) and absent breathing. Mice lacking GAD65 are viable but have reduced anxiety thresholds, increased seizure susceptibility, and abnormal fear conditioning.
Importantly, GAD65 is the dominant target of anti-GAD autoantibodies in stiff-person syndrome and a major target in type 1 diabetes, as discussed below.
Vitamin B6 (PLP) as Essential Cofactor
The chemistry that allows GAD to decarboxylate glutamate is the same chemistry that underpins essentially every amino acid transamination, decarboxylation, racemization, and elimination reaction in biology: the pyridoxal 5'-phosphate (PLP) Schiff-base mechanism. PLP is the active phosphorylated form of vitamin B6 (pyridoxine, pyridoxal, or pyridoxamine in food). Inside the enzyme's active site, the aldehyde of PLP forms a covalent Schiff base (an internal aldimine) with a specific lysine residue. When glutamate enters the active site, its alpha-amino group displaces the lysine, forming an external aldimine between PLP and the substrate. PLP then acts as an electron sink, stabilizing the carbanion intermediate that forms when the alpha-carboxyl departs as CO2. The product GABA is released, and the enzyme regenerates the lysine-PLP internal aldimine to begin the next catalytic cycle.
This dependence on PLP is the molecular reason why vitamin B6 status directly determines GABA synthesis capacity. The relationships are clinical:
- Pyridoxine-dependent epilepsy (PDE) is an autosomal recessive condition caused by mutations in the antiquitin gene (ALDH7A1), which functions in the lysine catabolism pathway. Mutations cause accumulation of alpha-aminoadipic semialdehyde, which spontaneously cyclizes to piperidine-6-carboxylate and irreversibly traps PLP. Affected newborns present with refractory seizures that respond dramatically to high-dose pyridoxine within minutes — one of the most striking responses in all of pediatric neurology.
- The anti-tuberculosis drug isoniazid is a PLP antagonist (it forms a hydrazone with PLP, depleting the free pool) and causes pyridoxine-responsive peripheral neuropathy and, at high doses, seizures. Co-administration of pyridoxine is standard.
- The mushroom Gyromitra esculenta contains gyromitrin, which is hydrolyzed in vivo to monomethylhydrazine — another PLP antagonist that causes seizures responsive to high-dose pyridoxine.
- Chronic alcohol abuse depletes PLP via multiple mechanisms and contributes to alcohol withdrawal seizures, which often respond partially to thiamine and pyridoxine repletion alongside benzodiazepines.
- Marginal B6 deficiency (common in elderly populations, pregnancy, and those on certain medications including isoniazid, cycloserine, hydralazine, and L-DOPA) reduces overall GAD activity and may contribute to subclinical anxiety, sleep disturbance, and reduced seizure threshold.
The clinically meaningful B6 intake range for adults is approximately 1.3-2.0 mg/day from food and supplements combined, with upper limit of 100 mg/day to avoid sensory neuropathy from sustained high-dose pyridoxine. Most therapeutic protocols for GABA support use 25-50 mg/day of pyridoxal-5-phosphate (the activated form) or pyridoxine HCl. See the Vitamin B6 page for more on forms, dosing, and the neuropathy risk at chronic high doses.
GABA Receptors — GABA-A and GABA-B
GABA signals through two structurally and functionally distinct receptor families, analogous to the ionotropic vs. metabotropic split on the glutamate side:
- GABA-A receptors are pentameric ligand-gated chloride channels assembled from combinations of alpha (1-6), beta (1-3), gamma (1-3), delta, epsilon, theta, pi, and rho subunits. The dominant central nervous system subtype is alpha1-beta2-gamma2 (in a 2:2:1 stoichiometry). GABA binding opens the channel, allowing chloride influx that hyperpolarizes the postsynaptic neuron and reduces its excitability. GABA-A receptors are the targets of essentially all clinical sedative-hypnotic drugs: benzodiazepines, barbiturates, alcohol, propofol, etomidate, and the volatile and intravenous anesthetics all act here, each through distinct binding sites on the receptor.
- GABA-B receptors are seven-transmembrane G-protein coupled receptors coupled to Gi/Go. They produce slower, longer-lasting inhibition through three mechanisms: (1) opening of inwardly-rectifying potassium (GIRK) channels postsynaptically, hyperpolarizing the cell; (2) closing of voltage-gated calcium channels presynaptically, reducing neurotransmitter release; and (3) inhibition of adenylate cyclase, reducing intracellular cAMP. The clinical GABA-B agonist baclofen is used for spasticity in multiple sclerosis, spinal cord injury, and cerebral palsy, and is sometimes used off-label for alcohol use disorder.
The relative balance between GABA-A and GABA-B contributions varies by region. Hippocampal pyramidal cells receive substantial GABA-B input that contributes to the slow afterhyperpolarization and the regulation of theta-rhythm oscillations. Cortical layer 1 has dense GABA-B-mediated inhibition that gates ascending thalamic input. Striatal medium spiny neurons receive prominent GABA-B-mediated presynaptic inhibition.
The pharmacological GABA-A site that allows benzodiazepines (diazepam, lorazepam, alprazolam, clonazepam, etc.) to enhance the receptor is at the interface between alpha and gamma subunits and is present only on receptors containing certain alpha subunits (alpha1, alpha2, alpha3, alpha5 are benzodiazepine-sensitive; alpha4 and alpha6 are insensitive). This subunit selectivity explains why some experimental Z-drugs targeting only alpha1 (zolpidem) produce primarily hypnosis without the anxiolytic, anticonvulsant, and myorelaxant effects of broader-spectrum benzodiazepines.
Tonic vs Phasic Inhibition
GABAergic inhibition in the brain operates in two temporally distinct modes:
- Phasic inhibition is mediated by synaptic GABA-A receptors (typically alpha1-beta-gamma2 containing) and produces brief, large-amplitude inhibitory postsynaptic currents in response to vesicular GABA release. Phasic IPSCs decay over milliseconds and provide the rapid moment-to-moment shaping of neuronal firing patterns.
- Tonic inhibition is mediated by extrasynaptic GABA-A receptors (typically containing alpha4, alpha5, alpha6, or delta subunits) that have very high affinity for GABA and are persistently activated by the low ambient concentration of GABA in the extracellular space (estimated at 0.1-1 micromolar). Tonic inhibition produces a small, persistent chloride current that sets the resting input resistance of the cell and the gain of synaptic responses.
The therapeutic implications matter. Benzodiazepines preferentially enhance phasic inhibition (they require the gamma2 subunit, present at synapses). The hypnotic gaboxadol (a selective delta-containing extrasynaptic receptor agonist) enhances tonic inhibition. Neurosteroids like allopregnanolone (an endogenous metabolite of progesterone) and the synthetic neurosteroid brexanolone (FDA-approved for postpartum depression in 2019) preferentially potentiate delta-containing extrasynaptic GABA-A receptors. Ethanol enhances both synaptic and extrasynaptic GABA-A receptors but with different concentration-response relationships, contributing to its complex behavioral profile.
The mechanism of tonic inhibition explains why the elimination of just one or two key GAD-expressing interneuron populations can dramatically alter the excitability of an entire cortical region — the ambient GABA tone supporting tonic inhibition depends on the small fraction of GABA that escapes from synaptic release and is not immediately reuptaken by GAT-1/GAT-3 transporters.
GABA-A Modulators (Benzos, Barbiturates, Alcohol, Anesthetics)
The GABA-A receptor is one of the most pharmacologically modulated proteins in clinical medicine. The major drug classes acting at this receptor:
- Benzodiazepines (diazepam, lorazepam, alprazolam, clonazepam, midazolam, oxazepam, temazepam, triazolam, etc.) bind the benzodiazepine site at the alpha-gamma interface and increase the frequency of GABA-A channel openings when GABA is bound. Because they require GABA for activity, they have a ceiling effect and are relatively safe in overdose unless combined with other CNS depressants. Reversal agent: flumazenil.
- Barbiturates (phenobarbital, pentobarbital, thiopental, butalbital) bind a distinct site on GABA-A receptors and increase the duration of channel opening. At higher concentrations they directly open the channel without GABA, removing the ceiling effect — the reason barbiturates are far more dangerous in overdose than benzodiazepines. Largely replaced by safer alternatives but still used for refractory status epilepticus, induction of anesthesia (thiopental, methohexital), and migraine prophylaxis (butalbital combinations).
- Z-drugs (zolpidem, zaleplon, eszopiclone) bind the benzodiazepine site but with selectivity for alpha1-containing receptors, producing primarily hypnotic effects with less anxiolytic and myorelaxant action. Tolerance and dependence still occur with chronic use.
- Alcohol (ethanol) potentiates GABA-A receptors at intoxicating concentrations (5-50 mM blood alcohol), particularly the extrasynaptic delta-containing subtypes. This GABA-A potentiation accounts for much of alcohol's sedative and anxiolytic effects; alcohol also has NMDA antagonist effects that contribute to its dissociative qualities and the rebound hyperexcitability of withdrawal.
- Volatile and intravenous anesthetics — isoflurane, sevoflurane, desflurane, propofol, etomidate — all potentiate GABA-A receptors as a major (though not sole) mechanism of producing general anesthesia. Each agent has a distinctive binding profile.
- Neurosteroids — allopregnanolone, pregnanolone, tetrahydrodeoxycorticosterone (THDOC) — are endogenous progesterone and deoxycorticosterone metabolites that powerfully potentiate GABA-A receptors at low nanomolar concentrations. The synthetic version brexanolone was FDA-approved in 2019 for postpartum depression. The oral neurosteroid zuranolone (Zurzuvae) was approved in 2023, also for postpartum depression.
- Gaboxadol (THIP) is an experimental delta-subunit-selective extrasynaptic GABA-A agonist that was developed for insomnia and explored for fragile X syndrome.
This pharmacological abundance reflects the central role of GABA-A inhibition in setting overall brain state. The Goldilocks principle applies: too little GABA tone produces anxiety, insomnia, and seizures; too much produces sedation, ataxia, and coma. Most of clinical sedative-hypnotic practice is the art of finding the right GABA-A modulator for the right patient at the right dose.
Anti-GAD Autoimmunity — Stiff-Person Syndrome and T1DM
Anti-GAD65 autoantibodies are clinically significant in two very different diseases:
Stiff-person syndrome (SPS) is a rare autoimmune neurological disorder characterized by progressive muscle stiffness, painful spasms, exaggerated startle responses, and a tendency to develop a hyperlordotic posture. The high-titer presence of anti-GAD65 antibodies (often >100-fold the levels seen in T1DM) is essentially pathognomonic — present in 60-80% of cases. The remaining cases include antibodies against amphiphysin (often paraneoplastic, associated with breast cancer), glycine receptor (the rare PERM variant: progressive encephalomyelitis with rigidity and myoclonus), or other targets. The pathophysiology involves antibody-mediated inhibition of GAD activity and impaired GABAergic inhibition, producing the characteristic stiffness and spasms. Treatment includes high-dose benzodiazepines (diazepam 60-100 mg/day or higher), baclofen, IVIG, plasmapheresis, and rituximab in refractory cases. Celine Dion publicly disclosed her SPS diagnosis in 2022, raising awareness of this previously obscure condition.
Type 1 diabetes mellitus (T1DM) is autoimmune destruction of pancreatic beta cells, and anti-GAD65 antibodies are one of the four classic islet autoantibodies used to identify pre-clinical and clinical T1DM (alongside anti-insulin, anti-IA2, and anti-ZnT8 antibodies). The reason beta cells are vulnerable to anti-GAD autoimmunity is that pancreatic beta cells express GAD65 (originally a surprise — GABA was assumed to be a CNS-only neurotransmitter). Beta cells produce GABA as part of their islet paracrine signaling, where GABA dampens glucagon secretion from neighboring alpha cells. The shared antigen explains why GAD-targeted immune tolerization (the Diamyd diabetes vaccine) was developed as an attempted T1DM intervention, though clinical results have been modest.
Anti-GAD antibodies (typically at lower titers than in SPS) are also found in some cases of cerebellar ataxia, limbic encephalitis, and pharmacoresistant temporal lobe epilepsy. The mechanistic understanding of how anti-GAD antibodies produce disease is incomplete — some of the antibody effect may be on cell-surface GAD65, but GAD is largely intracellular, so the relationship between autoantibody titer and clinical phenotype is still being worked out.
Nutritional Strategies to Support GABA Synthesis
From a clinical naturopathic perspective, supporting endogenous GABA synthesis from the glutamate pool involves attending to several modifiable factors:
- Vitamin B6 (PLP) — the absolute cofactor. Adequate B6 intake is the single most important nutritional determinant of GAD activity. For routine support, 25-50 mg/day of pyridoxal-5-phosphate (P5P) or pyridoxine HCl. Avoid sustained doses above 100 mg/day to prevent pyridoxine-induced sensory neuropathy.
- Magnesium — allosterically potentiates GABA-A receptor function and is the natural NMDA channel blocker (see the Neurotransmission page). Magnesium glycinate or magnesium L-threonate at 300-600 mg/day elemental magnesium is the typical dose. Magnesium L-threonate has some evidence for superior brain penetration but is more expensive.
- Zinc — modulates GABA-A receptor function, particularly the gamma2-containing subtypes. Maintain adequate intake (15-30 mg/day).
- L-theanine — an amino acid analog of glutamate found in tea (Camellia sinensis), reaches the brain and modestly enhances GABA, dopamine, and serotonin while producing alpha-wave EEG activity. Typical dose 100-400 mg.
- Taurine — a sulfonic amino acid that is itself a weak GABA-A receptor agonist and supports GABAergic tone. Typical dose 500-3000 mg/day. See the Taurine page.
- Glycine — an inhibitory neurotransmitter in its own right (spinal cord and brainstem) and an NMDA co-agonist (forebrain — making the role complex). Typical dose 3-10 g at bedtime for sleep support.
- Botanical GABAergic agents — valerian root, passionflower, lemon balm, skullcap, ashwagandha, kava (with hepatotoxicity caveats), and chamomile all have varying degrees of GABAergic activity. They work through multiple mechanisms including direct GABA-A allosteric modulation and reuptake inhibition.
- Reduce excitatory load — chronic stress, caffeine, alcohol withdrawal, sleep deprivation, and inflammatory states all increase excitatory tone and create disproportionate demand on the GABA system. Lifestyle measures that reduce chronic sympathetic activation (sleep, regular exercise, meditation, breath work) support net inhibitory tone.
For patients with anxiety, insomnia, restless legs syndrome, migraine, or seizure disorders, a thorough assessment of B6 and magnesium status is a reasonable first step in any naturopathic plan. See the Anxiety and Epilepsy pages for condition-specific management.
Does Oral GABA Cross the Blood-Brain Barrier?
One of the most persistent questions in supplement marketing is whether oral GABA actually reaches the brain. The answer, despite decades of confident claims by supplement manufacturers, is: poorly, if at all, through the blood-brain barrier directly. GABA is a small, polar zwitterion. It does not have a dedicated transporter at the blood-brain barrier, and passive diffusion is limited. Multiple studies using radioactive tracers and microdialysis have found that systemically administered GABA produces minimal increases in brain GABA concentrations.
However, the absence of direct BBB penetration does not necessarily mean oral GABA has no effect. Two indirect mechanisms have been proposed:
- Enteric nervous system effects — GABA receptors are expressed on enteric neurons, vagal afferents, and gut endocrine cells. Oral GABA may signal through these peripheral pathways to influence parasympathetic tone and stress reactivity via the vagus nerve. EEG studies have shown that oral GABA (around 100 mg) can produce measurable changes in brain alpha-wave activity within an hour, possibly through these enteric routes.
- BBB permeability in pathological states — in conditions involving BBB disruption (severe inflammation, sepsis, traumatic brain injury, advanced multiple sclerosis), GABA may penetrate the brain more readily. The clinical relevance for routine supplement use is unclear.
The pragmatic conclusion is that oral GABA at typical supplement doses (100-750 mg) may produce mild anxiolytic effects in some users, but the mechanism is unlikely to be direct brain delivery. For patients seeking GABAergic effects through supplementation, a strategy emphasizing the synthesis precursors (glutamic acid, B6, magnesium) and indirect modulators (L-theanine, taurine, botanicals) is more mechanistically sound than oral GABA itself.
Clinical Applications: Anxiety, Insomnia, Seizures
The clinical consequences of inadequate GABA synthesis (or excessive glutamate signaling unmatched by inhibitory counterbalance) span psychiatry and neurology:
- Generalized anxiety disorder — benzodiazepines work, demonstrating that GABA-A potentiation alleviates anxiety. Long-term benzodiazepine use carries dependence, cognitive impairment, and increased dementia risk concerns. Naturopathic approach: address B6, magnesium, sleep hygiene, exercise, stress management; consider L-theanine, taurine, ashwagandha, valerian. Refer for evidence-based therapy (CBT) and pharmacology when severe.
- Insomnia — GABA-A modulators (benzodiazepines, Z-drugs) dominate prescription sleep aids but have tolerance, rebound, and cognitive concerns. Naturopathic approach: sleep hygiene, light exposure timing, magnesium, glycine 3 g at bedtime, melatonin, valerian, L-theanine. See Fatigue page for related sleep recommendations.
- Migraine — glutamatergic hyperexcitability is implicated; magnesium 400 mg/day, riboflavin 400 mg/day, and CoQ10 have some preventive evidence. Anti-CGRP monoclonal antibodies have transformed migraine prophylaxis pharmacology, but the GABA/glutamate balance remains relevant.
- Epilepsy — most antiepileptic drugs work at least partly through GABA enhancement (valproate, vigabatrin, benzodiazepines, barbiturates, tiagabine) or glutamate reduction (lamotrigine, topiramate, perampanel). Nutritional ketosis (ketogenic diet) is an effective intervention for refractory pediatric epilepsy and works partly through enhanced GABA synthesis. Pyridoxine repletion is standard in any neonatal seizure work-up.
- Restless legs syndrome / periodic limb movement disorder — iron deficiency is the primary correctable cause; GABAergic medications (gabapentin, pregabalin) and dopaminergic agents are the mainstays of pharmacological treatment.
- Tinnitus — central gain hypotheses implicate reduced GABAergic inhibition in auditory cortex; GABAergic agents have modest clinical effects.
The takeaway: the glutamate-to-GABA conversion is one of the most clinically consequential single biochemical steps in the body. Supporting it through adequate B6 and magnesium status is one of the most underappreciated nutritional interventions in neuropsychiatric care.
Key Research Papers
- Roberts E, Frankel S (1950). Gamma-aminobutyric acid in brain: its formation from glutamic acid. Journal of Biological Chemistry. — PubMed
- Erlander MG et al. (1991). Two genes encode distinct glutamate decarboxylases. Neuron. — PubMed
- Asada H et al. (1997). Cleft palate and decreased brain gamma-aminobutyric acid in mice lacking the 67-kDa isoform of glutamic acid decarboxylase. PNAS. — PubMed
- Solimena M et al. (1988). Autoantibodies to glutamic acid decarboxylase in a patient with stiff-man syndrome, epilepsy, and type I diabetes mellitus. NEJM. — PubMed
- Baekkeskov S et al. (1990). Identification of the 64K autoantigen in insulin-dependent diabetes as the GABA-synthesizing enzyme glutamic acid decarboxylase. Nature. — PubMed
- Mills PB et al. (2006). Mutations in antiquitin in individuals with pyridoxine-dependent seizures. Nature Medicine. — PubMed
- Sigel E, Steinmann ME (2012). Structure, function, and modulation of GABA(A) receptors. Journal of Biological Chemistry. — PubMed
- Meldrum BS (1989). GABAergic mechanisms in the pathogenesis and treatment of epilepsy. British Journal of Clinical Pharmacology. — PubMed
- Meltzer-Brody S et al. (2018). Brexanolone injection in post-partum depression: two multicentre, double-blind, randomised, placebo-controlled, phase 3 trials. The Lancet. — PubMed
- Boonstra E et al. (2015). Neurotransmitters as food supplements: the effects of GABA on brain and behavior. Frontiers in Psychology. — PubMed
- Murakami T et al. (2009). The effects of the orally administered gamma-aminobutyric acid (GABA) on the rat humoral immune response. European Journal of Pharmacology. — PubMed
- Dalakas MC (2009). Stiff-person syndrome and related disorders — diagnosis, mechanisms and therapies. Nature Reviews Neurology. — PubMed
PubMed Topic Searches
- PubMed: GAD and pyridoxal phosphate
- PubMed: Anti-GAD antibodies and SPS
- PubMed: GAD65 and T1DM autoantibodies
- PubMed: Pyridoxine-dependent epilepsy
- PubMed: GABA-A modulators
Connections
- Glutamic Acid Benefits Hub
- Glutamic Acid Overview
- Neurotransmission & Excitatory Signaling
- Nitrogen Metabolism
- Glutamate & MSG
- Vitamin B6 (PLP Cofactor)
- Magnesium
- Taurine (GABA-A Co-Agonist)
- Glycine
- Glutamine
- Anxiety
- Epilepsy
- Fatigue & Sleep
- Stress Management
- Gut-Brain Axis