IV High-Dose Vitamin C & Cancer
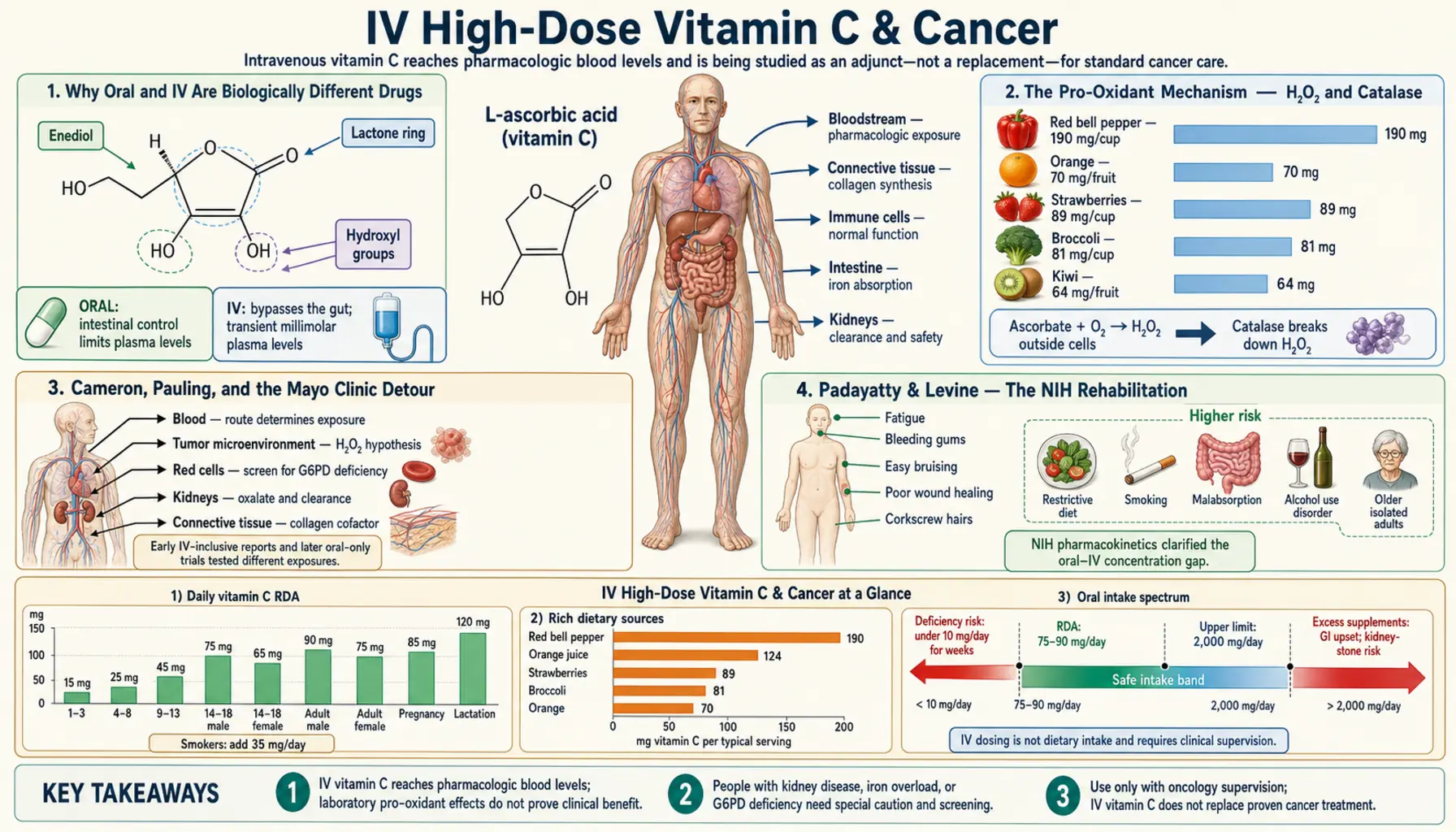
High-dose intravenous Vitamin C is, biochemically, a different drug from the same molecule taken orally. Oral dosing saturates plasma ascorbate around 100–200 µM; IV infusion at 50–100 g pushes plasma above 20,000 µM (over 20 mM) — a 100-fold concentration jump that activates a completely different mechanism: pro-oxidant generation of extracellular hydrogen peroxide selectively toxic to cancer cells that have lost normal catalase activity. This is the Riordan Clinic / Padayatty NIH / University of Kansas integrative-oncology protocol. This deep-dive walks through the historical arc from Cameron and Pauling through the Mayo Clinic rebuttals to the Levine pharmacokinetic rehabilitation, the mechanism work by Chen and Schoenfeld, the G6PD screening requirement, and an honest accounting of what the evidence shows and what it doesn't.
Interactive Visualization Vitamin C, Collagen & Why Sailors Fell Apart Zip three protein chains into the strongest rope in biology — then take the vitamin C away and watch the helix unravel, and old healed scars split back open. Launch →
Table of Contents
- Why Oral and IV Are Biologically Different Drugs
- The Pro-Oxidant Mechanism — H&sub2;O&sub2; and Catalase
- Cameron, Pauling, and the Mayo Clinic Detour
- Padayatty & Levine — The NIH Rehabilitation
- Chen, Schoenfeld & the Mechanism Work
- The Riordan Clinic Protocol
- Modern Trials: University of Kansas, Cornell, Iowa
- What the Evidence Shows — And What It Doesn't
- G6PD Screening — The Essential Safety Step
- Integration With Conventional Oncology
- Cautions & Contraindications
- Patient FAQ
- Key Research Papers
- Connections
- Featured Videos
Why Oral and IV Are Biologically Different Drugs
The single most important fact about IV Vitamin C is the pharmacokinetic one: oral dosing simply cannot achieve the plasma concentrations that make IV interesting for cancer. The Levine 1996 PNAS paper and the Padayatty 2004 Annals of Internal Medicine follow-up established the curve definitively.
Oral dosing saturates. As single-dose intake rises above 200 mg, fractional absorption drops sharply. Renal tubular reabsorption of filtered ascorbate also saturates — the excess spills into urine. The result: oral plasma steady-state caps at approximately 80–220 µM no matter how much you take. Even bowel-tolerance megadoses (10–30 g/day) plateau around 220 µM plasma. The body's homeostatic systems are tuned to keep plasma vitamin C in the low-micromolar range.
IV infusion bypasses every absorption and renal homeostasis barrier. A 50 g IV infusion over 60–90 minutes pushes plasma to 13,000–20,000 µM (13–20 mM). A 100 g infusion can reach 30,000 µM. These concentrations are 100–200-fold higher than the upper limit oral dosing can achieve, and they persist for several hours before renal clearance brings them back down.
At these pharmacological concentrations the chemistry of ascorbate in extracellular fluid changes. Ascorbate auto-oxidizes in the presence of trace metals (released from injured or dying tissue) generating hydrogen peroxide (H&sub2;O&sub2;) in the extracellular space at micromolar concentrations. The H&sub2;O&sub2; is the active agent, not the ascorbate itself. The Chen 2005 and Chen 2008 PNAS papers measured tumor extracellular H&sub2;O&sub2; concentrations during IV ascorbate infusion in mouse xenografts and confirmed the mechanism directly.
This is why every oral-dose clinical trial that fails to show anti-cancer benefit is irrelevant to the IV-dose question. They are different drugs. Treating them as the same drug is the conceptual error that delayed serious clinical investigation by about 30 years.
The Pro-Oxidant Mechanism — H&sub2;O&sub2; and Catalase
Why would extracellular H&sub2;O&sub2; selectively kill cancer cells? The answer is catalase deficiency.
Catalase is the enzyme that converts H&sub2;O&sub2; to water and oxygen, neutralizing it. Normal cells have high catalase activity in peroxisomes and adequate glutathione peroxidase backup in cytoplasm and mitochondria. When extracellular H&sub2;O&sub2; appears, normal cells absorb it and detoxify it quickly — net result, no damage.
Many cancer cells have low catalase activity. The reasons vary: metabolic reprogramming during oncogenic transformation downregulates peroxisomal enzymes; rapid proliferation outstrips antioxidant gene expression; some oncogenes (KRAS, BRAF, MYC) actively suppress catalase. Whatever the cause, low catalase means the cancer cell cannot detoxify the incoming H&sub2;O&sub2;. The H&sub2;O&sub2; reacts with intracellular iron (cancer cells often have elevated labile iron pools too) via Fenton chemistry to generate hydroxyl radical — the most damaging ROS in biology — which fragments DNA, peroxidizes lipids, and kills the cell.
The Schoenfeld 2017 Cancer Cell paper extended the picture: non-small-cell lung cancer and glioblastoma cells are particularly susceptible because they have both low catalase and elevated labile iron, making them doubly vulnerable to the H&sub2;O&sub2;-iron-hydroxyl-radical cascade. This work led directly to the ongoing trials of pharmacological ascorbate as a radiosensitizer in NSCLC and GBM at the University of Iowa.
The Yun 2015 Science paper added another wrinkle for KRAS- and BRAF-mutant colorectal cancers: dehydroascorbate (the oxidized form of vitamin C) is taken up by these cells through GLUT1 (which they overexpress because of their altered glucose metabolism), then reduced back to ascorbate inside the cell. The intracellular ascorbate then oxidizes again, depleting cellular NADPH and glutathione, and selectively killing the mutant cells.
So there is no single anti-cancer mechanism for high-dose ascorbate. There are at least three (extracellular H&sub2;O&sub2; / Fenton chemistry; intracellular DHA uptake via GLUT1 + redox depletion in KRAS/BRAF mutants; HIF-1α degradation via prolyl hydroxylase activity) and the relative importance varies by tumor type.
Cameron, Pauling, and the Mayo Clinic Detour
The modern story starts with Scottish surgeon Ewan Cameron and Linus Pauling. In a 1976 PNAS paper, they reported that terminally ill cancer patients given 10 g/day of vitamin C (initially IV for 10 days, then oral indefinitely) lived four times longer on average than matched historical controls. Some patients experienced apparent remissions. The paper was electrifying.
The Mayo Clinic mounted what was supposed to be a definitive refutation. Charles Moertel and colleagues ran two randomized trials (1979 NEJM and 1985 NEJM) in advanced colorectal cancer patients, comparing 10 g/day oral vitamin C to placebo. Both trials found no benefit. The oncology establishment concluded the matter was settled and "vitamin C does not work for cancer" became the consensus.
The conceptual error: the Mayo trials used oral dosing. Cameron and Pauling had used IV dosing initially before transitioning to oral. The IV phase was producing the plasma concentrations that mattered; the subsequent oral was maintenance. By eliminating the IV induction, the Mayo design tested a different intervention — one that, in retrospect, could not possibly have worked because oral plasma levels cannot reach the pro-oxidant pharmacological range.
Levine and colleagues at NIH spent years documenting the pharmacokinetic difference. By the late 1990s and early 2000s, the Padayatty 2004 paper made the case rigorously: any future trial of vitamin C in cancer must use IV dosing to achieve pharmacological plasma levels. The Mayo trials had effectively tested whether a homeopathic dose of a chemotherapy drug worked — an unfair test. The path to serious IV trials reopened.
The 25 years between the Mayo trials (1979/1985) and the Padayatty rehabilitation (2004) is sometimes called "the lost generation" in integrative-oncology vitamin C research. The Riordan Clinic in Wichita, Kansas, kept the IV clinical practice alive throughout this period, treating thousands of patients and accumulating the case-series experience that later trials would build on.
Padayatty & Levine — The NIH Rehabilitation
Sebastian Padayatty and Mark Levine at the NIH's National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) did the conceptual rehabilitation in three landmark papers:
- Padayatty 2004 (Ann Intern Med) — established the oral vs IV pharmacokinetic difference quantitatively. Showed that even at 1.25 g IV, plasma reached 885 µM — already six times higher than any oral dose achieves. At 50 g IV, plasma reached 13,500 µM.
- Padayatty 2006 (CMAJ) — reported three well-documented case studies of patients with advanced cancers (renal, bladder, B-cell lymphoma) treated with IV ascorbate (15–65 g, 1–3×/week) who had apparent durable remissions. Case reports are not RCT evidence but they re-established the clinical plausibility that had been dismissed for decades.
- Padayatty 2010 (PLoS ONE) — surveyed CAM practitioners administering IV ascorbate and documented the safety profile. With proper G6PD screening and patient selection, IV doses up to 100 g were essentially free of serious adverse events. This established that the procedure was safe enough to justify formal clinical trials.
The combined effect was to make IV vitamin C respectable again in academic oncology. By 2010 the University of Kansas Medical Center, University of Iowa, Thomas Jefferson, and Weill Cornell had ongoing trials. The framing had shifted from "alternative medicine" to "investigational drug at pharmacological dose."
Chen, Schoenfeld & the Mechanism Work
The pre-clinical mechanism work that anchored the clinical revival came mostly from Mark Levine's NIH lab and from Joseph Cullen and Garry Buettner at the University of Iowa.
Qi Chen's two PNAS papers (2005 and 2008) showed that pharmacological ascorbate generates extracellular H&sub2;O&sub2; in tumor tissue at concentrations capable of killing cancer cells but not normal cells. The 2008 paper used mouse xenograft models of ovarian, pancreatic, and glioblastoma tumors and demonstrated tumor growth reduction with IV ascorbate alone.
Welsh 2013 (Cancer Chemother Pharmacol) ran a phase I trial of IV pharmacological ascorbate combined with gemcitabine in metastatic pancreatic cancer. The combination was well-tolerated and the response rate appeared higher than gemcitabine alone, leading to the Polireddy 2017 follow-up and to the larger ongoing pancreatic trials.
Schoenfeld 2017 (Cancer Cell) elucidated why NSCLC and GBM are particularly sensitive: low catalase plus high labile iron creates the Fenton-chemistry vulnerability described above. This paper led to ongoing radiosensitization trials in those two cancer types — IV ascorbate during radiotherapy to selectively amplify radiation-induced ROS damage in the tumor while sparing normal tissue (which has normal catalase).
Yun 2015 (Science) opened a separate mechanistic chapter for KRAS- and BRAF-mutant colorectal cancers: GLUT1-mediated dehydroascorbate uptake leading to intracellular redox collapse. This is being pursued in colorectal cancer specifically, where the KRAS-mutant subset has historically been the hardest to treat with targeted therapy.
The Cieslak and Cullen 2015 review consolidated the pancreatic cancer mechanism work; Polireddy 2017 demonstrated metastasis inhibition in pancreatic xenografts; multiple other groups have published parallel work in lymphoma, melanoma, and hepatocellular carcinoma.
The Riordan Clinic Protocol
The Riordan Clinic (founded by Hugh Riordan in 1975 in Wichita, Kansas) is the longest-running clinical center treating cancer with IV ascorbate. Hugh Riordan was a contemporary of Pauling and Cameron; the clinic continued under his son Mikael after his death and remains the canonical reference for IV vitamin C clinical practice.
The Riordan Intravenous Vitamin C (RIVC) protocol, published in their 2005 paper and refined over thousands of patient-treatment-sessions:
- Initial test dose: 15 g IV ascorbate (as buffered sodium ascorbate) infused over 60–90 minutes — verifies tolerance and measures post-infusion plasma ascorbate
- Standard escalation: Increase to 25 g, then 50 g, then 75 g per infusion as tolerated, monitoring plasma ascorbate to confirm reaching pharmacological levels (typically >7,000 µM / 7 mM)
- Maintenance frequency: 2–3 infusions per week during active treatment phase
- Duration: Months, often years; continued indefinitely in patients with response
- Concurrent oral: 4–10 g/day oral ascorbate to maintain baseline tissue ascorbate between infusions
- Adjunctive nutrients: Magnesium (to support cardiovascular tolerance of infusion volume), B-complex, glutathione, alpha lipoic acid as indicated; protocols vary by clinic
- Pre-treatment requirements: G6PD enzyme assay (rule out deficiency); CBC and CMP (rule out renal failure or marked hypovolemia); review of all current chemotherapy / radiation timing
The Riordan protocol is the de-facto standard that most North American integrative oncology IV vitamin C clinics use. Specific dosing and frequency vary, but the basic architecture — pharmacological dosing aimed at >5–20 mM plasma, 2–3 weekly, indefinite duration, G6PD-screened patients — is consistent across practitioners.
Cost in the US in 2026: typically $150–$400 per infusion at private integrative oncology clinics. Most insurance does not cover it. A treatment year is often $20,000–$50,000 out of pocket. The financial burden is a real constraint and is one reason oral high-dose remains the more accessible option even though it is biochemically inferior for the cancer indication.
Modern Trials: University of Kansas, Cornell, Iowa
The University of Kansas Medical Center integrative oncology program (Jeanne Drisko and colleagues) has been a major academic center for IV vitamin C trials. Their ovarian cancer phase II trial showed reduced chemotherapy toxicity and improved quality of life when IV ascorbate was added to carboplatin + paclitaxel, with a trend toward improved progression-free survival. The pancreatic cancer trials at Kansas, Iowa, and Cornell have explored ascorbate as chemosensitizer or radiosensitizer rather than monotherapy.
The University of Iowa Free Radical Cancer Biology program (Garry Buettner, Joseph Cullen, Bryan Allen) has focused on IV ascorbate as a radiosensitizer. Their NSCLC and GBM phase I/II trials have shown the combination is well-tolerated and have suggested radiosensitization benefit, with phase III trials ongoing.
Memorial Sloan Kettering, MD Anderson, and other major NCI-designated cancer centers have run smaller pilot trials, with mixed but generally encouraging results. The current research direction is increasingly toward IV ascorbate as combination therapy (sensitizer for chemo or radiation; toxicity-reducer for chemo) rather than as monotherapy.
Pancreatic cancer is the most-studied tumor type. Lung cancer (especially NSCLC) is the most-studied with radiation combinations. Glioblastoma is studied at Iowa specifically. Ovarian cancer has the Kansas data. Hematologic malignancies (especially KRAS-mutant lymphomas and TET2-mutant myeloid malignancies, per Cimmino 2017) are an emerging area.
What the Evidence Shows — And What It Doesn't
An honest accounting in 2026:
What the evidence DOES show
- IV ascorbate at 50–100 g per infusion reliably achieves plasma concentrations (5–20 mM) that activate the pro-oxidant H&sub2;O&sub2; mechanism in pre-clinical models
- The procedure is safe in G6PD-screened, properly hydrated, normal-renal-function patients — serious adverse events are uncommon
- Multiple cancer cell lines and xenograft models show meaningful in-vivo growth inhibition from pharmacological ascorbate alone
- IV ascorbate appears to reduce chemotherapy toxicity (especially fatigue and nausea) when added to standard chemotherapy regimens, improving quality of life
- The radiosensitization signal in NSCLC and GBM is mechanistically coherent and supported by phase I/II data
- Subset analyses suggest particular benefit in KRAS/BRAF-mutant colorectal cancer and pancreatic cancer
- Case series of durable remissions in advanced cancers (especially lymphomas) are real and credibly documented, though uncontrolled
What the evidence DOES NOT yet show
- No definitive phase III randomized controlled trial has demonstrated improved overall survival from IV ascorbate monotherapy or combination therapy in any cancer type. The trials underway may change this in the next 3–5 years.
- The optimal dose, infusion frequency, and treatment duration are not standardized — clinical practice varies widely and may be sub-optimal in either direction
- Which cancers respond and which do not is not fully characterized — current selection is partly based on mechanism (KRAS/BRAF mutants; low-catalase tumors) and partly on tradition (Riordan-era pancreatic and ovarian emphasis)
- Whether IV ascorbate combined with specific newer targeted therapies (immune checkpoint inhibitors, CAR-T, CDK4/6 inhibitors) helps, hurts, or is neutral is largely unknown
- Cost-effectiveness has not been formally analyzed in any health-system context
How to think about it as a patient
IV vitamin C is one of the most-studied integrative oncology interventions and has the strongest mechanistic case of any "complementary" cancer treatment. But it is not a cure for cancer, and any clinic that markets it as one is overselling. A reasonable position: IV vitamin C is plausibly beneficial as an add-on to standard oncologic care, especially for chemotherapy toxicity reduction and quality of life, with the cancer-killing benefit speculative-to-probable depending on tumor type. The decision to pursue it should involve the treating oncologist, account for cost and time burden, and not displace standard treatment.
G6PD Screening — The Essential Safety Step
Glucose-6-phosphate dehydrogenase (G6PD) deficiency is an X-linked enzyme deficiency affecting roughly 400 million people worldwide, with highest prevalence in people of African, Mediterranean, Middle Eastern, and Southeast Asian descent. G6PD is the rate-limiting enzyme in the pentose phosphate pathway that generates NADPH, which keeps glutathione reduced. G6PD-deficient red blood cells cannot regenerate glutathione fast enough to detoxify acute oxidative stress.
High-dose IV ascorbate generates extracellular H&sub2;O&sub2;. In G6PD-deficient patients, this H&sub2;O&sub2; can overwhelm red cell glutathione defenses and cause acute hemolysis — a potentially life-threatening medical emergency. Several cases of fatal hemolysis from IV vitamin C in unrecognized G6PD deficiency have been published.
The screening test is a simple quantitative G6PD enzyme assay on a blood sample. It costs around $30–100 and is widely available. No reputable IV vitamin C clinic infuses without G6PD testing. Any clinic that skips this step is reckless.
In G6PD-deficient patients, IV ascorbate is contraindicated. Oral high-dose vitamin C is generally considered safe even in G6PD deficiency (oral plasma concentrations stay too low to generate problematic H&sub2;O&sub2; loads), though caution at bowel-tolerance levels is reasonable.
Integration With Conventional Oncology
Older concerns that vitamin C would "interfere with chemotherapy by blocking the oxidative damage chemo depends on" have largely been resolved in the negative direction. The Welsh 2013 pancreatic cancer phase I work and subsequent combination studies have shown that IV ascorbate generally either does not interfere or actively sensitizes chemotherapy. Some specific drug combinations are favorable:
- Gemcitabine (pancreatic, NSCLC) — multiple positive combination signals
- Carboplatin + paclitaxel (ovarian) — Kansas trials showed reduced toxicity, possible improved PFS
- Radiation therapy (NSCLC, GBM) — mechanistically rational radiosensitization
- 5-FU / FOLFIRINOX — emerging combinations in colorectal and pancreatic
Combinations that may warrant more caution:
- Bortezomib (Velcade) in multiple myeloma — some in-vitro data suggests high vitamin C might reduce bortezomib efficacy by direct chemical reduction of the boronic acid. Most clinicians separate IV ascorbate from bortezomib dosing by at least 24 hours.
- Methotrexate — vitamin C may slightly enhance methotrexate clearance; timing separation is reasonable.
For timing relative to chemotherapy infusions: most protocols give IV ascorbate either on chemo-free days or 2–4 hours after the chemotherapy infusion completes. This avoids any theoretical direct chemical interaction in the bloodstream during infusion.
For radiation therapy combinations, IV ascorbate is typically given within hours before each radiation session to amplify the radiation-induced ROS damage in the tumor.
The treating oncologist must be in the loop. Surprising the oncology team with a parallel IV protocol they don't know about creates avoidable conflict and can result in mis-interpretation of imaging and lab changes. Coordination is essential.
Cautions & Contraindications
- G6PD deficiency — absolute contraindication for IV high-dose (see above). Screen all patients before starting.
- Renal failure — ascorbate is cleared renally; impaired clearance allows prolonged elevation and risks oxalate-stone formation. CKD stage 4–5 patients should not receive IV high-dose without nephrology coordination.
- Hemochromatosis or iron overload — ascorbate mobilizes iron and could worsen iron-mediated tissue damage. Discuss with hematology before starting.
- Active oxalate kidney stones — high-dose vitamin C increases urinary oxalate; relative contraindication. Ensure aggressive hydration if used.
- Severe heart failure — the infusion volume (typically 250–500 mL of fluid per infusion) can precipitate fluid overload in compromised cardiac status. Adjust volume or skip.
- Pregnancy — IV high-dose vitamin C in pregnancy is not well-studied and should generally be avoided.
- Concurrent bortezomib — separate by >24 hours.
- Glucose-meter interference — many glucometers (the ones using glucose dehydrogenase chemistry strips) read falsely elevated glucose when plasma ascorbate is very high. Diabetic patients on insulin should be aware to avoid over-correcting falsely "high" readings for several hours post-infusion.
Patient FAQ
Q: How much does IV vitamin C cost?
$150–$400 per infusion at most US integrative oncology clinics; typically 2–3 infusions per week. Annual cost $15,000–$60,000 out of pocket in most cases. Insurance rarely covers it.
Q: Should I do this instead of chemotherapy?
No. The strongest evidence supports IV vitamin C as an adjunct to standard oncologic care, not a replacement. Patients who use it as a substitute for evidence-based treatment have worse outcomes.
Q: Will my oncologist support this?
Increasingly, yes — especially at academic centers with integrative oncology programs. If your oncologist is dismissive, ask for a referral to an integrative oncologist or to one of the academic centers running trials (Kansas, Iowa, Memorial Sloan Kettering).
Q: How quickly will it work?
For quality-of-life and chemotherapy toxicity reduction: often within 1–3 weeks. For tumor response: this is highly variable and depends on tumor type, stage, and what else is being done. Some patients show measurable tumor markers improvement within 2–3 months; some show no measurable benefit; some show stabilization without shrinkage.
Q: Is there an oral alternative?
For the pharmacological pro-oxidant cancer mechanism, no — oral cannot reach the required plasma concentrations. For general supportive care during cancer treatment (immune support, fatigue, antioxidant defense), high-dose oral (4–10 g/day in divided doses, or to bowel tolerance) is a reasonable lower-cost alternative that captures the non-pharmacological benefits.
Q: What about liposomal vitamin C?
Liposomal oral vitamin C does achieve higher plasma levels than conventional oral (Davis 2016) but still does not reach the multi-millimolar pharmacological range. It is a useful step between conventional oral and IV but does not replace IV for cancer indications.
Key Research Papers
- Cameron E, Pauling L (1976). Supplemental ascorbate in the supportive treatment of cancer. PNAS. — PubMed
- Moertel CG et al. (1985). High-dose vitamin C versus placebo in the treatment of patients with advanced cancer who have had no prior chemotherapy. NEJM. — PubMed
- Padayatty SJ et al. (2004). Vitamin C pharmacokinetics: implications for oral and intravenous use. Ann Intern Med. — PubMed
- Padayatty SJ et al. (2006). Intravenously administered vitamin C as cancer therapy: three cases. CMAJ. — PubMed
- Chen Q et al. (2005). Pharmacologic ascorbic acid concentrations selectively kill cancer cells. PNAS. — PubMed
- Chen Q et al. (2008). Pharmacologic doses of ascorbate act as a prooxidant in tumor xenografts. PNAS. — PubMed
- Schoenfeld JD et al. (2017). O&sub2;&sup-; and H&sub2;O&sub2;-mediated disruption of Fe metabolism causes the differential susceptibility of NSCLC and GBM cancer cells to pharmacological ascorbate. Cancer Cell. — PubMed
- Yun J et al. (2015). Vitamin C selectively kills KRAS and BRAF mutant colorectal cancer cells. Science. — PubMed
- Welsh JL et al. (2013). Pharmacological ascorbate with gemcitabine for the control of metastatic and node-positive pancreatic cancer. Cancer Chemother Pharmacol. — PubMed
- Riordan HD et al. (2005). A pilot clinical study of continuous intravenous ascorbate in terminal cancer patients. PR Health Sci J. — PubMed
- Hoffer LJ et al. (2008). Phase I clinical trial of i.v. ascorbic acid in advanced malignancy. Ann Oncol. — PubMed
- Padayatty SJ et al. (2010). Vitamin C: intravenous use by CAM practitioners and adverse effects. PLoS ONE. — PubMed
- Cimmino L et al. (2017). Restoration of TET2 function blocks aberrant self-renewal and leukemia progression by ascorbate. Cell. — PubMed
- Polireddy K et al. (2017). High-dose parenteral ascorbate inhibited pancreatic cancer growth and metastasis. Sci Rep. — PubMed
PubMed Topic Searches
- PubMed: intravenous vitamin C cancer
- PubMed: pharmacological ascorbate cancer
- PubMed: high-dose vitamin C pancreatic cancer
- PubMed: ascorbate radiosensitization NSCLC GBM
- PubMed: G6PD deficiency IV vitamin C hemolysis
- PubMed: Riordan IVC protocol cancer
Connections
- Vitamin C, Collagen & Why Sailors Fell Apart — interactive animation
- Vitamin C Overview
- Vitamin C Benefits Hub
- Vitamin C for Immune Function
- Vitamin C for Collagen Synthesis
- Vitamin C for Iron Absorption
- Cancer
- Alpha Lipoic Acid Benefits Hub
- Glutathione
- NAC
- Gerson Therapy
- Fenbendazole
- Oxidative Stress
- Magnesium
- Iron
- G6PD Enzyme Assay
- Ferritin
- All Vitamins
- All Antioxidants