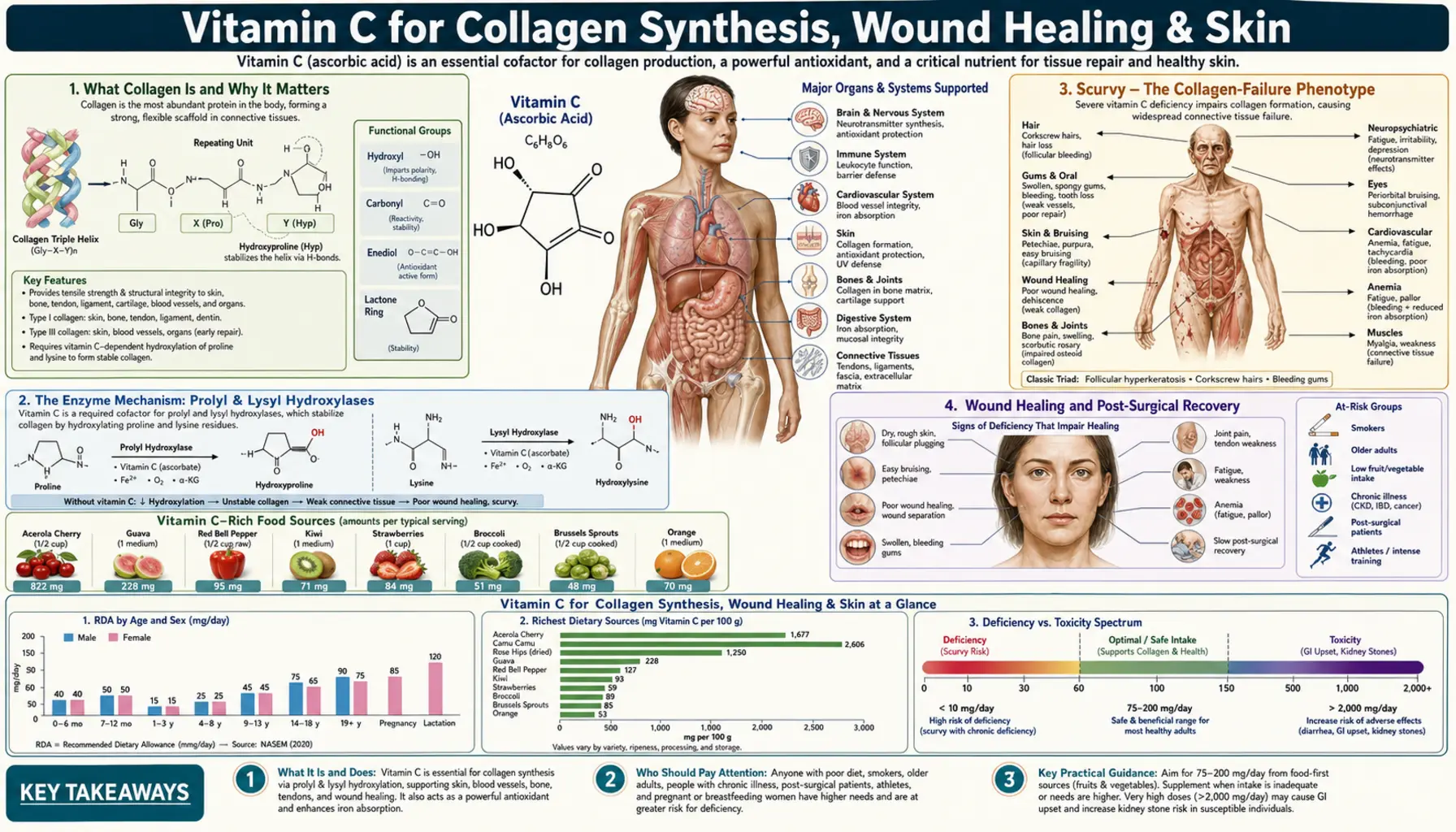
Vitamin C for Collagen Synthesis, Wound Healing & Skin
Scurvy is not "vitamin C deficiency" in the abstract — it is a structural collapse of collagen. Without ascorbate, prolyl 4-hydroxylase and lysyl hydroxylase cannot keep their iron centers in the reduced Fe²+ state, the proline and lysine residues in newly synthesized procollagen cannot be hydroxylated, the triple helix cannot stabilize, and the body literally falls apart at the seams: gums bleed, old scars reopen, wounds will not heal, capillaries leak, teeth loosen, and finally death follows from hemorrhage or infection. This deep-dive walks through the mechanism in detail, the post-surgical and wound-healing dosing, the Shaw 2017 tendon-loading protocol, topical L-ascorbic acid for photoaging, and the vitamin C + vitamin E pairing for skin.
Interactive Visualization Vitamin C, Collagen & Why Sailors Fell Apart Zip three protein chains into the strongest rope in biology — then take the vitamin C away and watch the helix unravel, and old healed scars split back open. Launch →
Table of Contents
- What Collagen Is and Why It Matters
- The Enzyme Mechanism: Prolyl & Lysyl Hydroxylases
- Scurvy — The Collagen-Failure Phenotype
- Wound Healing and Post-Surgical Recovery
- Tendon, Ligament & Cartilage — The Shaw Protocol
- Skin Elasticity and Photoaging
- Topical L-Ascorbic Acid — Formulation Reality
- The Vitamin C + Vitamin E Pairing
- Hyaluronic Acid & Elastin Support
- The Full Collagen-Building Cofactor Stack
- Cautions
- Key Research Papers
- Connections
- Featured Videos
What Collagen Is and Why It Matters
Collagen is the single most abundant protein in the human body — about 30% of total body protein, or roughly 5–10 kg in an adult. It is the load-bearing structural protein of skin (Types I and III), bone (Type I — about 90% of the organic bone matrix), cartilage (Type II), tendons and ligaments (Type I), blood vessel walls (Type IV in basement membranes, Type I and III in vessel walls), cornea (Type I), and the periodontal ligament that holds teeth in their sockets. There are at least 28 distinct collagen types in human biology, all built from the same fundamental architecture: a triple helix of three polypeptide α-chains wound around each other in a tight rope-like structure.
The triple helix is what gives collagen its tensile strength — pound for pound, collagen fibers are stronger than steel. But the triple helix cannot form unless specific proline and lysine residues in the polypeptide chains are first hydroxylated. The hydroxyl groups form hydrogen bonds across the three chains that stabilize the triple helix. Without those hydrogen bonds the helix is thermally unstable at body temperature and dissolves.
This single fact — that the triple helix requires hydroxylated proline and lysine, and the hydroxylation requires Vitamin C — is what makes ascorbate the cofactor that holds the human body together.
The Enzyme Mechanism: Prolyl & Lysyl Hydroxylases
The procollagen chain is synthesized on the rough endoplasmic reticulum. As it is being made, two enzymes work on it in parallel:
- Prolyl 4-hydroxylase (P4H) — hydroxylates proline residues at the 4-position to form 4-hydroxyproline. About half of all the proline residues in collagen are hydroxylated this way. The enzyme uses molecular oxygen and α-ketoglutarate as substrates, requires Fe²+ in its active site, and requires ascorbate to keep the iron in the reduced Fe²+ state. Without ascorbate the iron oxidizes to Fe³+, the enzyme becomes inactive, and proline hydroxylation stops.
- Lysyl hydroxylase — hydroxylates specific lysine residues. The hydroxylysines are critical for collagen cross-linking later — without them, the mature collagen fibers cannot form the covalent inter-chain bonds that give collagen its tensile strength. Same chemistry: Fe²+-dependent, α-ketoglutarate-dependent, ascorbate-dependent.
Both enzymes belong to the larger family of 2-oxoglutarate-dependent dioxygenases — the same enzyme family that includes the HIF-prolyl hydroxylases, the TET DNA demethylases, the JmjC histone demethylases, γ-butyrobetaine hydroxylase (carnitine synthesis), and many others. All of them share the same Fe²+ chemistry. All of them require ascorbate as the iron-reducing cofactor. This is the unifying mechanism that explains why Vitamin C has such broad effects across so many systems — one cofactor, one chemistry, dozens of enzymes.
What happens in deficiency: the iron oxidizes in the enzyme active site after each catalytic cycle. Without ascorbate to re-reduce it, the enzyme becomes a one-shot — it works once, then stops. Collagen synthesis grinds to a halt. The polypeptide chains continue to be made but cannot fold into stable triple helices. The defective procollagen is degraded by the cell. The connective tissues are deprived of new collagen while their existing collagen continues to turn over normally. The result is the slow structural collapse of every collagen-containing tissue — scurvy.
The Pinnell 1985 Yale J Biol Med review and the Kivirikko 1985 work in Ann NY Acad Sci remain the canonical mechanism references; the chemistry has not changed.
Scurvy — The Collagen-Failure Phenotype
Scurvy is the clinical syndrome of severe Vitamin C deficiency, and its symptom list is a near-perfect catalog of "what happens when collagen synthesis stops":
- Perifollicular hemorrhages and corkscrew hairs — defective collagen in hair follicles causes the hair shafts to coil and small capillaries around follicles to leak.
- Easy bruising and petechiae — capillary basement membrane collagen weakens; minor trauma produces large bruises; intact capillaries spontaneously leak red cells into the skin.
- Swollen, purple, bleeding gums and loose teeth — the periodontal ligament (Type I collagen) connecting tooth root to alveolar bone degenerates; teeth literally fall out.
- Old scars reopen, new wounds will not heal — this is collagen biology made visible. The body cannot replace turning-over collagen in old scar tissue, so the scar comes apart. New wounds have no new collagen to remodel into mature scar tissue.
- Joint and bone pain, pathologic fractures — the organic matrix of bone (90% Type I collagen) cannot be maintained; the bone becomes brittle.
- Hemarthrosis — bleeding into joints because synovial vessels leak.
- Fatigue, irritability, depression — partly from anemia, partly from the additional non-collagen roles of ascorbate (carnitine synthesis fails, fat oxidation impairs; dopamine-β-hydroxylase fails, norepinephrine drops).
- Death — in untreated scurvy, typically from hemorrhage, infection of unhealable wounds, or cardiac failure.
The clinical horror of scurvy is that it kills slowly, painfully, and reversibly. Two weeks of fresh citrus juice — James Lind's 1747 controlled trial on HMS Salisbury — reverses the entire syndrome. The 16th-19th century maritime death toll from scurvy is conservatively estimated at over two million sailors — more than all naval combat deaths combined — from a deficiency cured by a teaspoon of ascorbate.
Modern scurvy is rare but not absent. It occurs in elderly people living alone, alcoholics, severely picky-eating children with autism spectrum conditions, and patients on chronic restricted diets. Subclinical scurvy — deficient enough to impair wound healing or immune function but not enough to produce frank scurvy — is more common, especially in hospitalized and post-surgical patients, where ascorbate is rapidly consumed by inflammatory stress.
Wound Healing and Post-Surgical Recovery
Every phase of wound healing requires collagen synthesis, and therefore requires Vitamin C.
The healing process has three overlapping phases. Inflammation (days 0–3) clears debris and recruits cells. Proliferation (days 3–21) lays down the granulation tissue — a temporary matrix of Type III collagen interlaced with new blood vessels — that fills the wound. Remodeling (weeks to months) converts the Type III collagen of the early scar to the stronger Type I collagen of mature scar tissue, increasing tensile strength from about 20% of normal at week 3 to about 80% of normal at six months.
Plasma ascorbate falls rapidly after surgery, trauma, or burns — sometimes to scurvy-level concentrations within 48–72 hours — because the inflamed wound consumes it. The Bates 1972 work on urinary hydroxyproline excretion showed that collagen synthesis rates and ascorbate availability are tightly coupled in healing tissues. Surgical patients with low pre-operative ascorbate have measurably slower wound healing and higher wound-complication rates.
Practical perioperative dosing commonly used in integrative practice:
- 2 weeks before surgery: 1,000–2,000 mg/day in divided doses, to saturate tissue stores
- Day of surgery: Hold if surgeon is concerned about bleeding (though there is no strong evidence vitamin C increases surgical bleeding)
- 2–6 weeks post-op: 1,000–2,000 mg/day, continuing until wound is fully healed
- Combine with zinc (15–30 mg/day) and adequate protein intake (1.2–1.5 g/kg/day during healing)
For burn patients in critical care, much higher IV doses are used — some centers use up to 66 mg/kg/hour IV ascorbate (the "Tanaka protocol") during the first 24 hours of severe burn resuscitation, with evidence of reduced fluid requirements and reduced organ failure. This is an ICU intervention, not an outpatient one.
For dental procedures and skin biopsies, lower doses (500–1,000 mg/day) for the week before and 2 weeks after are reasonable. For major orthopedic surgery, plastic surgery, or any procedure involving extensive tissue planes, the higher dosing range is appropriate.
Tendon, Ligament & Cartilage — The Shaw Protocol
The Shaw 2017 study in Am J Clin Nutr is one of the most clinically useful pieces of Vitamin C research published in the last decade. Greg Shaw and colleagues at the Australian Institute of Sport asked a simple question: if you consume Vitamin C with gelatin (a collagen source providing the precursor amino acids proline, lysine, and glycine) 30–60 minutes before brief exercise that mechanically loads the target tendon, do you measurably increase collagen synthesis in that tendon?
They used a clean experimental design: engineered ligaments grown in culture, exposed to serum drawn from athletes 60 minutes after they consumed either 5g or 15g gelatin + 50 mg vitamin C. The serum from the gelatin + vitamin C condition increased collagen synthesis in the engineered ligaments measurably and dose-dependently versus placebo serum. Markers of collagen synthesis (procollagen N-terminal propeptide, P1NP) rose in the human subjects' blood as well.
The mechanism is intuitive: amino-acid availability is the substrate, mechanical loading triggers the synthesis machinery, and vitamin C is the cofactor that keeps the hydroxylase enzymes functioning. Stack all three within an hour, repeat several times per week, and tendon collagen synthesis is augmented.
Practical protocol (post-Shaw):
- 15 g unflavored gelatin (about one Knox envelope) or 15 g hydrolyzed collagen peptides dissolved in liquid
- 50–500 mg vitamin C with the gelatin
- 30–60 minutes before a brief targeted-loading exercise — for Achilles tendinopathy, a few sets of slow eccentric calf raises; for patellar tendinopathy, slow Bulgarian split squats; for rotator cuff, controlled external-rotation loading
- Repeat 2–3 times per week for at least 12 weeks to remodel collagen architecture
- Combine with a progressive loading rehabilitation program supervised by a physical therapist
The Shaw protocol has been broadly adopted in elite-sport rehabilitation for chronic tendinopathies (Achilles, patellar, hamstring, rotator cuff) and increasingly in ACL post-reconstruction rehab. The DePhillipo 2018 review in Orthop J Sports Med compiled the wider musculoskeletal-injury literature and reached similar conclusions: ascorbate is supportive at doses up to about 1 g/day for connective-tissue injury recovery.
For cartilage specifically, the picture is messier. Vitamin C supports Type II collagen synthesis in chondrocytes in vitro, but in vivo studies of vitamin C supplementation for osteoarthritis progression are mixed — one Australian cohort suggested that very high vitamin C intake might paradoxically associate with bone-marrow lesions and knee OA progression, while other studies show benefit. The current cautious recommendation: aim for adequate ascorbate (500–1,000 mg/day) rather than mega-doses for OA support.
Skin Elasticity and Photoaging
Skin contains roughly 75% of the body's collagen by mass, mostly Type I in the dermis. Dermal collagen and elastin together give skin its tensile strength and elasticity. UV exposure damages this architecture through three mechanisms: (1) direct photolytic cleavage of collagen and elastin fibers; (2) UV-induced ROS that oxidize the matrix proteins; and (3) upregulation of matrix metalloproteinase enzymes (MMP-1, MMP-9) that enzymatically degrade collagen and elastin.
Photoaging is the net result: wrinkles, sagging, loss of elasticity, mottled pigmentation, telangiectasias. Chronological aging adds a slower component — reduced fibroblast collagen synthesis with age, gradual collagen loss in postmenopausal women, accumulation of advanced glycation end-products (AGEs) that cross-link and stiffen existing collagen.
Vitamin C addresses photoaging through three complementary mechanisms:
- Supports new dermal collagen synthesis — the prolyl/lysyl hydroxylase cofactor mechanism described above. Oral and topical vitamin C both contribute, though by different routes.
- Quenches UV-induced ROS — reduces the oxidative collagen damage and the MMP-1 upregulation triggered by UV.
- Tyrosinase inhibition — reduces melanin synthesis, addressing the hyperpigmentation component of photoaging.
The Pullar, Carr, and Vissers 2017 Nutrients review compiled the dermatologic literature; the Telang 2013 Indian Dermatol Online J review summarized practical formulation choices.
For oral dosing aimed at skin: 500–1,000 mg/day, ideally paired with collagen peptides (10–15 g/day), vitamin E (15–30 mg natural d-α-tocopherol/day), zinc (15–30 mg/day), and copper (1–2 mg/day to balance the zinc). For visible skin improvement add topical L-ascorbic acid — the systemic-plus-topical combination outperforms either alone.
Topical L-Ascorbic Acid — Formulation Reality
Topical Vitamin C only works if the formulation chemistry is correct. The relevant constraints are unfortunately strict and most over-the-counter products fail at least one of them.
- Form: L-ascorbic acid is the gold standard — the form with the most published clinical evidence. Other derivatives (sodium ascorbyl phosphate, magnesium ascorbyl phosphate, tetrahexyldecyl ascorbate, ascorbyl glucoside, ascorbyl palmitate) have less data and varying intracellular conversion efficiency.
- Concentration: 10–20% L-ascorbic acid. Below 10% the percutaneous penetration is inadequate; above 20% the formulation becomes irritating without additional benefit. Most clinical trials used 15%.
- pH: Below 3.5 — ideally pH 2.5–3.0. L-ascorbic acid in its neutral / charged state at neutral pH does not cross the lipid stratum corneum. The acid is what penetrates. Buffered "gentle" topical vitamin C products at pH 5–6 do not deliver ascorbate to the dermis.
- Anhydrous formulation OR airtight packaging — L-ascorbic acid in aqueous solution oxidizes to yellow/brown within weeks unless oxygen exposure is minimized. A topical serum that has turned yellow or brown is mostly degraded and inactive. Single-use vials, airless pumps, or anhydrous (silicone/oil-based) formulations dramatically extend shelf life.
- Stabilizers: Including ferulic acid (0.5–1%) and vitamin E (1%) in the same product roughly doubles photoprotection and stabilizes the formulation. The SkinCeuticals C-E-Ferulic patent — not endorsing the brand, just noting the formulation that the dermatology literature most often cites — is the prototype of this approach.
Application: morning routine, on clean dry skin, before moisturizer and sunscreen. Wait 1–2 minutes for penetration before layering other products. Start every other day if the skin is sensitive; build to daily. Expect noticeable improvement in tone, brightness, and fine lines in 8–12 weeks of consistent use. The Humbert 2003 trial documented measurable ultrastructural collagen changes after 6 months of topical L-ascorbic acid use.
The Vitamin C + Vitamin E Pairing
Vitamin C and Vitamin E together are biologically more than the sum of their parts. The mechanism is the antioxidant network: when vitamin E (α-tocopherol) neutralizes a lipid peroxyl radical in a cell membrane, it itself becomes a tocopheroxyl radical — a stable but still reactive intermediate. Vitamin C donates an electron at the water-lipid interface to regenerate α-tocopherol back to its active form. Without vitamin C, vitamin E is consumed; with vitamin C, vitamin E is recycled.
The Lin 2003 study in J Am Acad Dermatol demonstrated this in vivo — topical vitamin C + vitamin E + ferulic acid provided substantially greater photoprotection (measured as reduced UV-induced erythema, thymine dimer formation, and sunburn-cell density) than vitamin C alone, vitamin E alone, or either pair without ferulic acid.
For oral combination, the same logic applies systemically. Vitamin C 500–1,000 mg/day + natural-source vitamin E (mixed tocopherols, 15–30 mg/day) is the canonical antioxidant baseline pairing. Avoid synthetic dl-α-tocopherol (it has only about half the biological activity of natural d-α-tocopherol and concerning long-term safety data at high doses).
Hyaluronic Acid & Elastin Support
The dermal extracellular matrix is not just collagen. Elastin gives skin its snap-back recoil after stretch. Hyaluronic acid (HA) is the glycosaminoglycan that fills the matrix with water, giving skin its plumpness. Glycosaminoglycans (chondroitin sulfate, dermatan sulfate, heparan sulfate) connect everything together.
Vitamin C supports the broader matrix in several ways. It is a cofactor for lysyl oxidase — the copper-dependent enzyme that cross-links both collagen and elastin (the cross-linking is what gives elastin its elastic properties). Vitamin C reduces oxidative damage to elastic fibers from UV exposure. Vitamin C in skin fibroblasts upregulates hyaluronic acid synthase expression and HA production.
Loss of elastin is the dominant component of the deep, etched-in wrinkles that develop in chronically sun-exposed skin (solar elastosis). Once degraded, elastin is very poorly regenerated — this is why prevention (sunscreen, antioxidants) outperforms treatment. Loss of dermal hyaluronic acid is the dominant component of the gradual flattening of skin that accompanies aging; topical HA serums and oral HA supplements can partially restore it.
Vitamin C is foundational to all of this, but it works in concert with the other matrix-supporting nutrients (copper for lysyl oxidase, sulfur amino acids for glycosaminoglycan synthesis, manganese for HA synthase, zinc for matrix protein turnover, biotin and silica for skin structural support).
The Full Collagen-Building Cofactor Stack
For comprehensive collagen support — whether for skin, wound healing, tendon recovery, or general anti-aging — the full cofactor stack is:
- Vitamin C — 500–1,000 mg/day, divided. The non-negotiable cofactor for prolyl and lysyl hydroxylases.
- Collagen peptides or gelatin — 10–15 g/day, ideally before targeted exercise (per Shaw protocol) or distributed across meals. Supplies the proline, hydroxyproline, glycine, and lysine substrate.
- Copper — 1–2 mg/day. Cofactor for lysyl oxidase, the copper-dependent enzyme that cross-links collagen and elastin. See Copper.
- Zinc — 15–30 mg/day. Cofactor for many matrix-remodeling metalloproteinases and for fibroblast function.
- Vitamin E — 15–30 mg/day natural d-α-tocopherol. Recycled by vitamin C; protects collagen and elastin from oxidative damage.
- Vitamin A (or carotenoids) — supports epithelial cell turnover and matrix remodeling.
- Silica / silicon — trace element supporting connective tissue cross-linking. Found in horsetail extract, bamboo extract, and choline-stabilized orthosilicic acid.
- Adequate protein intake — 1.0–1.5 g/kg/day; healing patients and athletes at the higher end.
- Vitamin K2 — supports calcium handling in connective tissue; the menaquinone-7 form is most studied.
The principle: collagen is not built from collagen peptides alone, nor from vitamin C alone — it is built from the integrated cooperation of substrate amino acids, mineral cofactors of the enzymes, and antioxidant defense for the newly synthesized matrix.
Cautions
- Hemochromatosis — iron-overload patients should keep vitamin C intake to RDA levels. The collagen-support stack for these patients should exclude iron-containing foods/supplements at the same meal as vitamin C.
- Calcium-oxalate kidney stones — chronic doses above 1 g/day may increase risk in predisposed individuals (Massey 2005). For wound healing or post-surgical use, short-term high-dose is acceptable; for chronic skin/anti-aging maintenance, stay under 1 g/day if there is a stone history.
- Topical irritation — L-ascorbic acid at pH <3.5 can sting or cause erythema on sensitive skin. Start every other day; if irritation persists, drop to 10% concentration; if still irritating, consider a non-acidic derivative like sodium ascorbyl phosphate (with the caveat that clinical evidence is weaker).
- Photosensitivity — topical L-ascorbic acid does not cause photosensitivity (this is a common misconception), but it is properly used in the morning rather than at night because the photoprotective benefit is wanted during sun-exposed hours.
- Pregnancy / breastfeeding — standard RDA-range vitamin C is safe and necessary; megadoses (5+ g/day) during pregnancy are not well-studied and not recommended.
- Excess oral dose ≠ more collagen — oral plasma vitamin C saturates around 200–400 mg single-dose. Dividing daily intake into multiple doses (e.g., 250 mg three times daily) is more effective than one 750 mg dose.
Key Research Papers
- Pinnell SR (1985). Regulation of collagen biosynthesis by ascorbic acid: a review. Yale J Biol Med. — PubMed
- Kivirikko KI, Myllylä R (1985). Post-translational processing of procollagens. Ann NY Acad Sci. — PubMed
- Shaw G et al. (2017). Vitamin C-enriched gelatin supplementation before intermittent activity augments collagen synthesis. Am J Clin Nutr. — PubMed
- Bates CJ et al. (1972). Hydroxyproline excretion and the assessment of vitamin C status. Br J Nutr. — PubMed
- Telang PS (2013). Vitamin C in dermatology. Indian Dermatol Online J. — PubMed
- Pullar JM, Carr AC, Vissers MCM (2017). The roles of vitamin C in skin health. Nutrients. — PubMed
- Humbert PG et al. (2003). Topical ascorbic acid on photoaged skin. Exp Dermatol. — PubMed
- Lin JY et al. (2003). UV photoprotection by combination topical antioxidants vitamin C and vitamin E. J Am Acad Dermatol. — PubMed
- DePhillipo NN et al. (2018). Efficacy of vitamin C supplementation on collagen synthesis after musculoskeletal injuries. Orthop J Sports Med. — PubMed
- Mohammed BM et al. (2016). Vitamin C: a novel regulator of neutrophil extracellular trap formation. Nutrients. — PubMed
- Tanaka H et al. (2000). Reduction of resuscitation fluid volumes in severely burned patients using ascorbic acid administration. Arch Surg. — PubMed
- Lind J (1753). A Treatise of the Scurvy. Reproduced in modern reviews. — PubMed: Lind treatise reviews
PubMed Topic Searches
- PubMed: vitamin C collagen synthesis
- PubMed: vitamin C wound healing
- PubMed: topical ascorbic acid skin
- PubMed: vitamin C tendon ligament
- PubMed: prolyl hydroxylase ascorbate
- PubMed: scurvy collagen mechanism
Connections
- Vitamin C, Collagen & Why Sailors Fell Apart — interactive animation
- Vitamin C Overview
- Vitamin C Benefits Hub
- Vitamin C for Immune Function
- IV High-Dose Vitamin C & Cancer
- Vitamin C for Iron Absorption
- Vitamin C and Collagen (legacy article)
- Collagen
- Vitamin E
- Copper
- Zinc
- Vitamin A
- Vitamin K
- Glycine
- Proline
- Lysine
- All Vitamins
- Oxidative Stress
- Alpha Lipoic Acid Benefits Hub