Vitamin B4 (Adenine), Modern Status and Food Sources
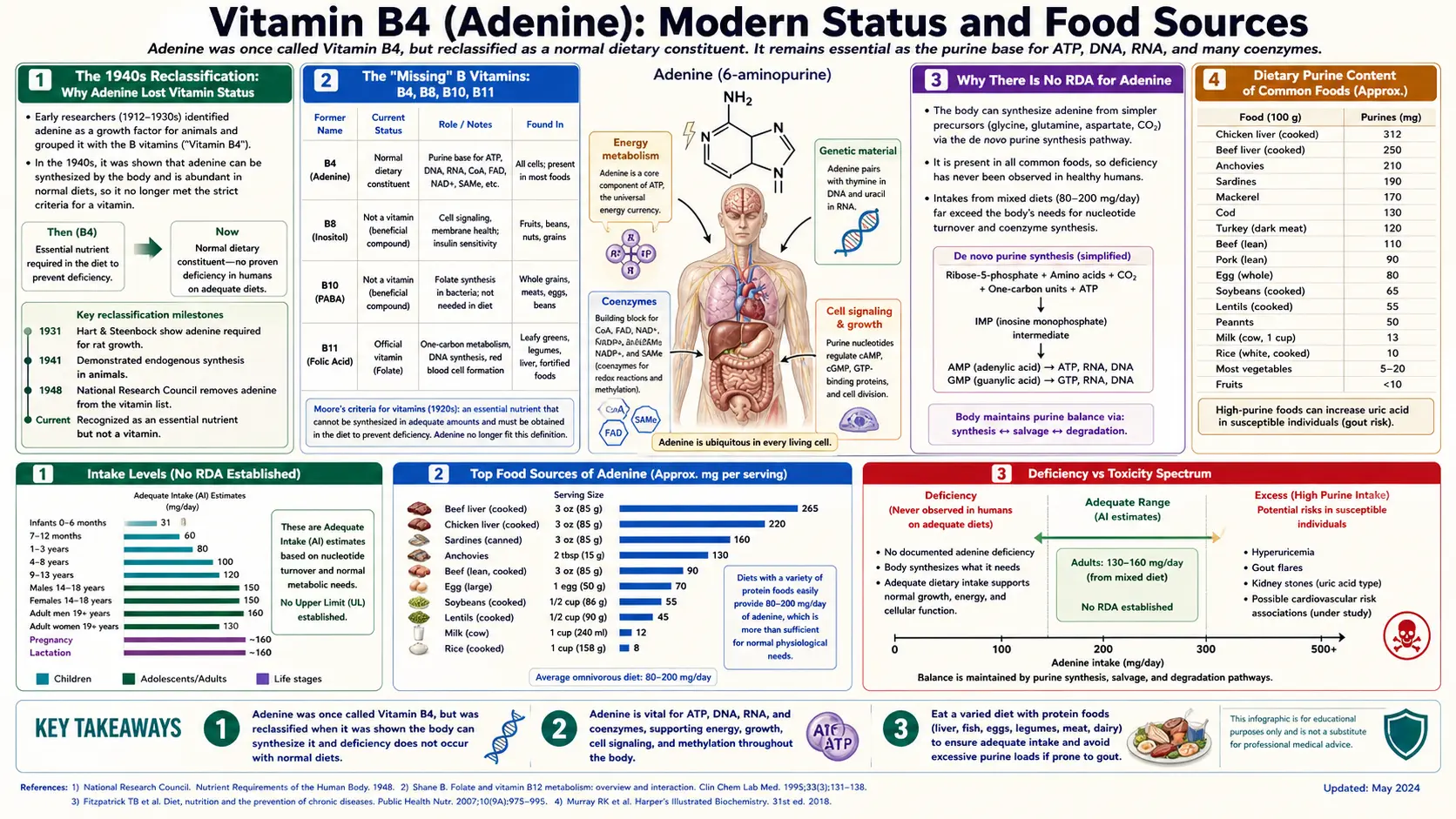
Adenine was reclassified out of the vitamin canon in the 1940s and 1950s when biochemists confirmed that human cells synthesize it in abundance from amino acid precursors through the de novo purine pathway. There is no Dietary Reference Intake, Recommended Dietary Allowance, or Adequate Intake for adenine in any modern nutritional guideline. Yet the "Vitamin B4" label persists in older European literature, in some commercial multivitamins, and in folk-nutrition discourse — and dietary purine content (of which adenine is roughly half) does have real clinical relevance in specific populations: gout patients, tumor lysis syndrome prophylaxis, patients with inborn errors of purine metabolism, and premature infants on total parenteral nutrition. This deep-dive covers the history of declassification, the food sources highest in purines, the clinical scenarios where diet matters, and the curious case of CPDA-1 blood preservation solution — one of the few medical settings where adenine is added intentionally to a clinical product.
Table of Contents
- The 1940s Reclassification: Why Adenine Lost Vitamin Status
- The "Missing" B Vitamins: B4, B8, B10, B11
- Why There Is No RDA for Adenine
- Dietary Purine Content of Common Foods
- High-Purine Foods: Organ Meats, Sardines, Yeast
- The Gout Diet: When Dietary Purines Matter
- Fructose, Alcohol, and Uric Acid
- TPN, Infant Formula, and Conditional Essentiality
- CPDA-1 Blood Preservation: Adenine as Pharmaceutical
- European and Russian "Vitamin B4" Supplements
- Key Research Papers
- Connections
- Featured Videos
The 1940s Reclassification: Why Adenine Lost Vitamin Status
The history of nutrition science contains several molecules that were briefly classified as vitamins and later reclassified out. Adenine is one of the cleanest examples. The original observation came from Wilhelm Reiss and colleagues in the 1920s and 1930s: rats fed purified diets stripped of nucleic acid developed leukopenia, growth failure, and impaired wound healing. The obvious inference was that some nucleic-acid-related factor was an essential dietary nutrient. Adenine, already structurally characterized by Emil Fischer in 1897, was assigned the placeholder "B4" in the still-expanding B-complex sequence.
Three lines of evidence dismantled the classification across the 1940s. First, John Buchanan and colleagues at MIT mapped the de novo purine biosynthesis pathway and demonstrated that mammalian cells synthesize purine bases from PRPP, glutamine, glycine, aspartate, and one-carbon units from folate. The synthetic capacity is robust and ramps up as needed.
Second, the original animal-deficiency observations were re-examined. The "leukopenia" and "growth failure" in Reiss's rats were re-attributed largely to folate deficiency (folate had not yet been recognized when the original observations were made), to amino-acid imbalance in the purified diets (glycine, glutamine, and aspartate are needed as ring-building precursors), and to other co-deficiencies in the unsupplemented test diets.
Third, the formal definition of "vitamin" tightened after World War II to require that the body cannot synthesize sufficient quantities of the molecule to meet metabolic demand. Adenine failed that test definitively in healthy humans, and by 1950 it had been removed from the official vitamin list in the U.S., U.K., and most European nutrition authorities.
The reclassification was reinforced by the discovery of the purine salvage pathway in the 1950s. Salvage enzymes (APRT, HGPRT) recycle approximately 90% of the daily purine turnover from breakdown products, dramatically reducing dependence on either de novo synthesis or dietary intake.
The "Missing" B Vitamins: B4, B8, B10, B11
The B-complex vitamin numbering has several gaps. The currently recognized B vitamins are B1 (thiamine), B2 (riboflavin), B3 (niacin), B5 (pantothenic acid), B6 (pyridoxine), B7 (biotin), B9 (folate), and B12 (cobalamin). The gaps at B4, B8, B10, and B11 represent compounds that were once provisionally classified as B vitamins but were later either reclassified as non-essential, recognized as duplicates of compounds already named, or shown to be biologically inactive.
- B4 = adenine — non-essential because human cells synthesize it de novo from PRPP and amino acids, plus the salvage pathway is robust. Sometimes the historical "B4" label was also applied to choline, which has had a tangled nomenclature history but is now classified as an essential nutrient with its own non-B-numbered name.
- B8 = inositol — non-essential because human cells synthesize it from glucose-6-phosphate. Inositol is metabolically important (phosphatidylinositol signaling, inositol phosphates as second messengers), but it does not meet the formal vitamin definition. Inositol supplements remain in use for polycystic ovary syndrome and as adjuncts in mood disorder, but the FDA does not regulate them as vitamins.
- B10 = para-aminobenzoic acid (PABA) — not a vitamin for humans, but a precursor in the bacterial folate biosynthesis pathway. PABA is the target of the sulfonamide antibiotics (sulfa drugs), which compete with PABA for binding to dihydropteroate synthase. PABA also appears in some sunscreens as a UV-A absorber.
- B11 = pteryl-hepta-glutamic acid (a form of folate) — reclassified because it duplicates B9. Some literature also uses "B11" for salicylic acid, but that label has no biological basis.
The gap pattern is a fossil record. Early 20th-century nutrition science generated a continuous stream of "candidate vitamins" based on partial-purification studies of nutritional factors. Most candidates failed the rigorous standards eventually adopted — either because the body synthesized them, because they were already-known compounds under a new name, or because the original deficiency observations were confounded by other unrecognized deficiencies. The numbering survives in the gaps.
Why There Is No RDA for Adenine
The U.S. Institute of Medicine (now National Academy of Medicine), the European Food Safety Authority (EFSA), and the WHO/FAO joint Codex Alimentarius all establish Dietary Reference Intakes (DRIs) only for nutrients that meet the formal definition of essentiality: the body cannot synthesize sufficient quantities to meet metabolic demand, and dietary intake below some threshold produces a recognizable deficiency syndrome in otherwise healthy people.
Adenine fails both criteria. The de novo purine biosynthesis pathway, combined with the salvage pathway, produces sufficient adenine and guanine in healthy adults regardless of dietary intake. No deficiency syndrome has ever been demonstrated in humans on a purine-restricted diet, even after prolonged restriction. (The closest analog is the experimental "purine-free" diet used to study uric acid metabolism in gout research, which produces only modest reductions in serum uric acid without any clinical sign of cellular dysfunction.)
Consequently, there is no RDA, AI, EAR, or UL for adenine. No country's nutrition labeling regulations require adenine content to be declared on food packaging. The compound does not appear in the USDA Nutrient Database in its own right, although total purine content is sometimes provided in supplementary databases used for gout dietary counseling.
The closest there is to an "intake recommendation" for adenine is the implicit purine-restriction guidance given to gout patients: limit organ meats, sardines/anchovies, beer, and high-fructose corn syrup. Even this guidance is not a positive intake target — it is a maximum-tolerated intake to avoid worsening hyperuricemia.
Dietary Purine Content of Common Foods
Dietary purine content is usually reported as total purines (adenine + hypoxanthine + guanine + xanthine) in milligrams per 100 grams of food, because the four bases all converge on uric acid through the same catabolic pathway and have similar uric-acid-raising effects per mole.
A rough categorization used in gout dietary counseling:
- Very high purine (>300 mg / 100 g): organ meats (liver, kidney, sweetbreads, brain), anchovies, sardines, mackerel, herring, mussels, scallops, certain shellfish, yeast extracts (Marmite, Vegemite), meat broths and gravies, game meats.
- Moderate-high purine (150–300 mg / 100 g): most other fish (tuna, salmon, trout), poultry skin, lentils, dried beans, peas, spinach, mushrooms, asparagus, cauliflower.
- Moderate purine (50–150 mg / 100 g): most muscle meats (beef, pork, lamb), other vegetables, whole grains.
- Low purine (<50 mg / 100 g): dairy products (milk, cheese, yogurt), eggs, most fruits, refined grains (white rice, white bread, pasta), low-fat baked goods, nuts.
The pattern is roughly that protein-dense animal tissues and rapidly-proliferating plant tissues (legumes, leafy greens, mushrooms, asparagus tips) have the highest purine content, while dairy, eggs, fruits, and refined grains are lowest. The reason is biological: cells with the highest nucleic acid concentration per gram have the highest purine content. Organ meats are particularly rich because the organ tissue itself was metabolically active, with high NAD, NADP, FAD, and ATP concentrations.
Important nuance: dietary purines from vegetable sources appear to raise serum uric acid less than equivalent purine loads from animal sources, possibly due to slower absorption kinetics and the alkalinizing effect of vegetable diets. Multiple cohort studies (notably the Health Professionals Follow-up Study, Choi et al. 2004 NEJM) have shown that vegetable purines do not increase gout risk while animal purines (particularly red meat and seafood) do.
High-Purine Foods: Organ Meats, Sardines, Yeast
Organ meats (liver, kidney, sweetbreads, brain, heart) are the highest-purine foods in the diet, often containing 500–1000 mg of purines per 100 g. Beef liver also happens to be the most nutrient-dense food on Earth by most other metrics (Vitamin A, B12, copper, choline, folate), so the trade-off between micronutrient density and purine load is a real one for gout patients. The traditional 1–2 servings per week of beef liver recommended on ancestral-eating regimes is well within the dietary purine tolerance of most non-gout individuals.
Sardines and anchovies are exceptionally high in purines (350–500 mg / 100 g) because they are small whole fish eaten with bones, organs, and reproductive tissue intact. They are also exceptional sources of omega-3 fatty acids, calcium (from the bones), vitamin D, and selenium. Gout patients are often counseled to limit sardines to once a week or less; non-gout patients have no reason to limit them.
Yeast extracts (Marmite, Vegemite, Brewer's yeast tablets) are concentrated yeast products with purine content typically 1000+ mg per 100 g. The serving size for table use is small (typically 5 grams), so the per-meal purine load is modest, but heavy users can exceed dietary purine recommendations for gout. Yeast extracts are also exceptional sources of B vitamins (especially B1, B2, B3, and B9) and are used in some traditional populations as fortified nutritional supplements.
Game meats (venison, elk, wild boar, rabbit) often have higher purine content than equivalent cuts of domesticated meat because game animals have more lean muscle and less intramuscular fat per unit weight — the muscle tissue itself is more cellularly dense.
Mushrooms are surprisingly high in purines (especially morels, porcini, and shiitake) because fungal cells maintain high RNA and DNA turnover.
Asparagus, spinach, and cauliflower are the highest-purine common vegetables but, per the vegetable-purine epidemiology cited above, do not appear to raise gout risk meaningfully.
The Gout Diet: When Dietary Purines Matter
For most people, dietary purine intake has only a modest effect on serum uric acid — perhaps 1–2 mg/dL between a very high-purine and very low-purine diet. Endogenous synthesis dwarfs dietary input in absolute terms.
In gout patients, that 1–2 mg/dL marginal effect matters because uric acid solubility has a hard threshold around 6.8 mg/dL at body temperature and physiologic pH. Above that threshold, monosodium urate crystals begin to form in synovial fluid and tendons. Bringing a patient from 7.5 mg/dL down to 6.5 mg/dL can substantially reduce flare frequency.
The 2020 American College of Rheumatology Guideline for the Management of Gout (Fitzgerald et al.) recommends:
- Limit alcohol (particularly beer, which contains both purines and ethanol that competes with uric acid for renal excretion), purine-rich animal foods (organ meats, sardines/anchovies), and high-fructose corn syrup.
- Encourage low-fat dairy products (which have a uric-acid-lowering effect through unclear mechanisms), cherries (whose anthocyanins may have a modest anti-inflammatory and uric-acid-lowering effect), and adequate hydration.
- Do not restrict vegetable purines, plant proteins, or whole grains — their epidemiologic association with gout is null or protective.
The guideline emphasizes that diet alone is generally insufficient for patients with established gout requiring urate-lowering therapy. Allopurinol or febuxostat reliably lower serum uric acid by 30–50%, far more than any dietary intervention. Diet should be considered adjunctive, not primary therapy.
Fructose, Alcohol, and Uric Acid
Two dietary factors raise serum uric acid more dramatically than purine intake per se: fructose and alcohol.
Fructose metabolism in the liver is unusual: fructose is rapidly phosphorylated by fructokinase to fructose-1-phosphate, consuming ATP without the normal feedback control of glucose phosphorylation. The ATP depletion increases AMP, which is then degraded down the purine catabolism pathway to uric acid. A single 500 mL bottle of high-fructose-corn-syrup soda can raise serum uric acid by 0.5–1.0 mg/dL within an hour. Chronic high fructose intake is now recognized as one of the strongest dietary risk factors for both gout incidence and gout flare frequency.
Alcohol raises uric acid by two mechanisms. First, ethanol metabolism in the liver elevates lactate, which competes with uric acid for renal tubular secretion via the URAT1 and OAT transporters — the body literally cannot excrete uric acid as fast while it is excreting lactate. Second, beer and certain spirits contain significant purine content (especially beer, which has 5–10 mg purines per 100 mL). The result is that beer is among the strongest dietary triggers for gout flares, more than equivalent purine loads from food.
The Choi cohort studies have consistently shown that men consuming more than two beers per day have roughly 2.5-fold the gout incidence of non-drinkers; the equivalent risk for spirits is roughly 1.5-fold; for wine it is essentially neutral. The wine-vs-beer difference probably reflects the purine content rather than ethanol per se.
TPN, Infant Formula, and Conditional Essentiality
While adenine is not essential for healthy adults, several clinical populations have elevated nucleotide demand that may exceed endogenous synthetic capacity. The concept is conditional essentiality: a nutrient that is not strictly required under normal physiological conditions becomes required when demand exceeds synthesis under stress.
Premature infants have rapidly growing tissues (especially gut, brain, immune system) and limited de novo purine synthesis capacity in the immature liver. Standard infant formulas have included nucleotide supplementation since the 1990s on this rationale — typically a blend of AMP, GMP, CMP, UMP at concentrations matching the nucleotide content of human breast milk. Trials have shown modest benefits including improved gut maturation, enhanced immune response to vaccination, and reduced diarrhea incidence in formula-fed preterm infants.
Total parenteral nutrition (TPN) patients receive intravenous nutrition because their gut is non-functional (post-bowel resection, gut ischemia, severe pancreatitis, etc.). Standard TPN solutions do not include nucleotides, on the rationale that endogenous synthesis is sufficient. However, several studies have demonstrated that nucleotide supplementation improves gut barrier function, reduces bacterial translocation, and accelerates recovery in critically ill TPN patients.
Critical illness, sepsis, and major trauma dramatically increase tissue purine demand because of accelerated cell turnover in immune system, gut crypts, and wound-healing tissues. Some critical care literature argues for nucleotide supplementation as part of "immunonutrition" protocols, alongside glutamine, arginine, and omega-3 fatty acids. The evidence is mixed.
Specific inborn errors of metabolism — adenosine deaminase deficiency (ADA-SCID), HGPRT deficiency (Lesch-Nyhan), APRT deficiency — each have specific dietary or pharmacologic management. ADA-SCID is typically treated with PEG-ADA enzyme replacement, hematopoietic stem cell transplant, or gene therapy rather than dietary intervention. APRT deficiency is managed with allopurinol (to prevent 2,8-dihydroxyadenine stones) and a low-purine diet. Lesch-Nyhan is managed with allopurinol for hyperuricemia, but the neurological phenotype is unaffected by dietary manipulation.
CPDA-1 Blood Preservation: Adenine as Pharmaceutical
One curious modern application of adenine is in stored blood products. Donated red blood cells stored for transfusion gradually lose ATP through ongoing metabolism in the storage bag, and the depletion of ATP compromises membrane integrity, deformability, and 2,3-bisphosphoglycerate (which regulates hemoglobin oxygen affinity). After several weeks, ATP-depleted red cells become spherocytic, fragile, and poorly functional after transfusion.
The solution, developed in the 1960s and 1970s, was to add adenine to the storage solution. Citrate-Phosphate-Dextrose-Adenine (CPDA-1) is the standard anticoagulant/preservative solution for whole-blood storage in many blood banks. The adenine concentration is roughly 0.25 mM — enough to maintain salvage-pathway flux through APRT, preserving ATP synthesis throughout the 35-day storage life. Without adenine, red cells retain meaningful function for only about 14–21 days; with CPDA-1, the shelf life extends to 35 days.
Additive solutions (AS-1, AS-3, AS-5, SAGM in Europe) used with packed red cells extend the shelf life further (to 42 days) through additional supplementation of mannitol, glucose, and adenine. These additive solutions are the reason modern blood banking can maintain a sufficient inventory of compatible red cell units for elective surgery.
This is one of very few clinical contexts where pure adenine is added to a pharmaceutical product. The dose is small (a typical 500 mL whole blood unit in CPDA-1 contains roughly 35 mg adenine), and the recipient's endogenous purine catabolism handles it without consequence.
European and Russian "Vitamin B4" Supplements
The "Vitamin B4" label persists in several niches of the supplement marketplace, particularly in European, Russian, and Eastern European literature. These commercial preparations typically contain one of three things:
- Adenine itself, marketed for vague "energy" or "anti-fatigue" benefits. There is no controlled evidence that oral adenine supplementation produces any clinical benefit in healthy adults — the body has no shortage of adenine, and supplementation does not increase tissue ATP or NAD pools meaningfully.
- Choline, which in some older European pharmacopoeias was assigned the "B4" label before being separated out as its own nutrient. Choline is a genuine essential nutrient (DRI of 425–550 mg/day, EFSA AI of 400 mg/day) that supports phosphatidylcholine, acetylcholine, and one-carbon metabolism. If a "Vitamin B4" product is actually choline, it may have nutritional value — but the labeling is misleading.
- Adenosine monophosphate (AMP) or adenosine triphosphate (ATP), marketed for "cellular energy" benefits. Oral ATP is rapidly hydrolyzed in the gut to free adenine, ribose, and phosphate before absorption — the cell wall of intestinal enterocytes is impermeable to ATP, so the marketing claim of "boosting cellular ATP" by oral ATP supplementation is mechanistically implausible.
None of the major regulatory bodies (FDA, EFSA, MHRA, Health Canada) recognize adenine as a vitamin or as an essential nutrient. Supplements labeled "Vitamin B4" exist in a legal gray zone and are typically sold under general supplement regulations rather than vitamin-specific frameworks.
The historical fingerprint of the "B4" label is also visible in older medical literature from the 1930s and 1940s, in some Eastern European clinical nutrition writing through the 1980s, and in folk-nutrition discourse that has not kept up with the 1940s reclassification. When patients ask about "Vitamin B4," it is generally appropriate to explain that the term is historical and that there is no modern nutritional requirement for adenine supplementation.
Key Research Papers
- Choi HK et al., purine-rich foods and the risk of gout in men (NEJM 2004) — PubMed: Choi NEJM 2004
- FitzGerald JD, 2020 American College of Rheumatology guideline for management of gout — PubMed: ACR Gout 2020
- Choi HK and Curhan G, soft drinks, fructose consumption, and the risk of gout — PubMed: Choi fructose & gout
- Choi HK, alcohol intake and risk of incident gout — PubMed: Choi alcohol & gout
- Carver JD, infant formula nucleotide supplementation and immune function — PubMed: Carver infant nucleotides
- Grimble GK, nucleotides in clinical nutrition and gut function — PubMed: Grimble clinical nucleotides
- Hess JR, CPDA-1 and additive solutions for red cell storage — PubMed: CPDA-1 storage
- Hogman CF, red cell preservation and the role of adenine — PubMed: Hogman red cell adenine
- Kaneko K, total purine and purine base content of foods (Japanese database) — PubMed: Kaneko purine database
- Lammer EJ, retinoic acid teratogenicity (cross-reference for vitamin definition rigor) — PubMed: Lammer 1985
- Zeisel SH, choline as the once-misclassified B vitamin, now essential nutrient — PubMed: Zeisel choline
- Yamamoto T, hypoxanthine and adenine recycling in human erythrocytes — PubMed: Erythrocyte purine recycling
Connections
- Vitamin B4 Benefits (Hub)
- Vitamin B4 (Main Page)
- Purine Metabolism
- Cellular Energy and ATP
- DNA and RNA Synthesis
- Choline (historical alt "B4")
- Inositol (historical "B8")
- Vitamin B9 (Folate)
- Vitamin B12
- Gout
- Uric Acid Test
- Organ Meats
- Sardines
- Lentils
- All Vitamins