Riboflavin (Vitamin B2) as the Glutathione Reductase Cofactor
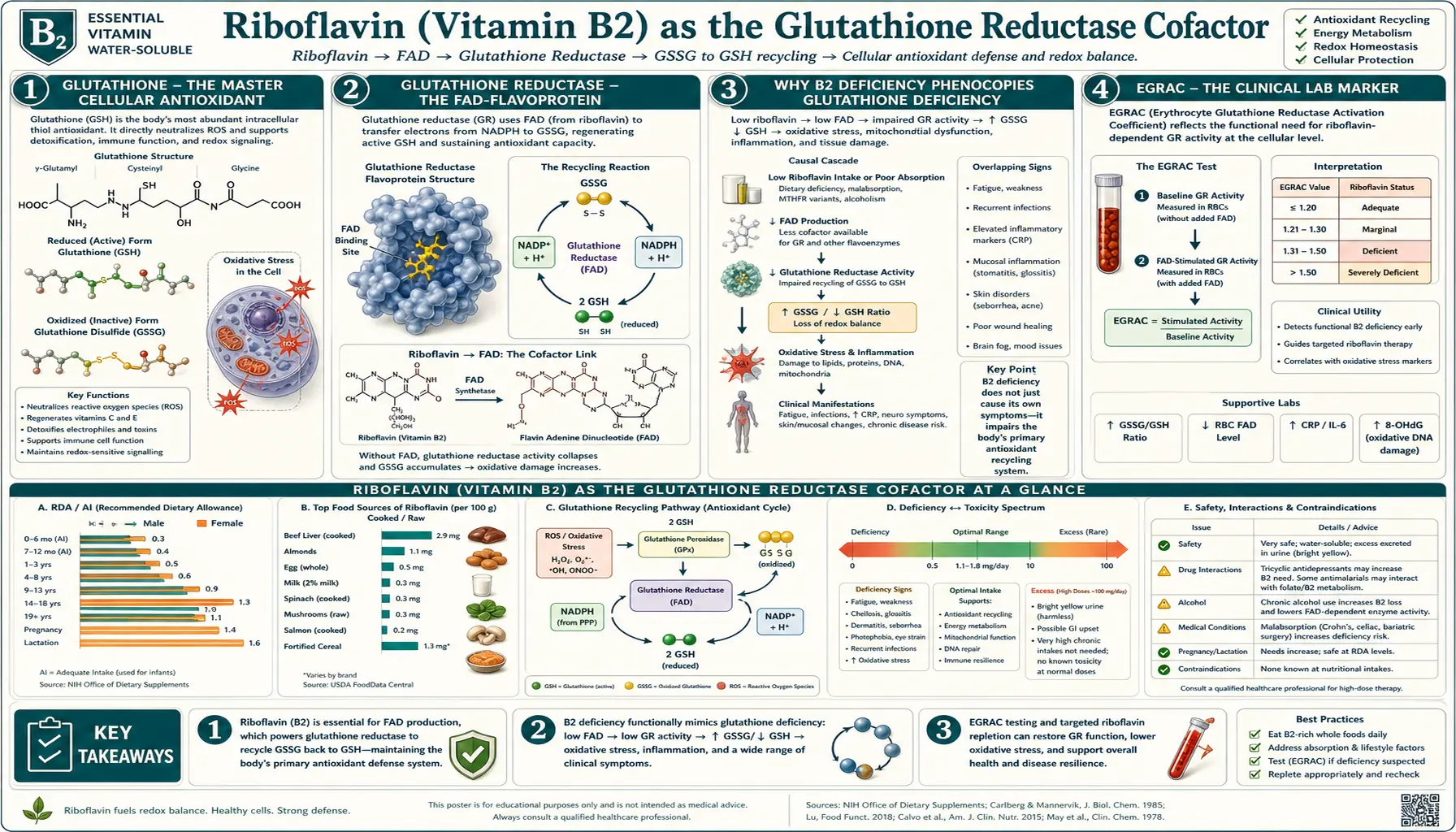
Glutathione is the body's master intracellular antioxidant. It is only effective in its reduced form (GSH). After scavenging a reactive oxygen species, GSH becomes oxidized glutathione disulfide (GSSG), which must be regenerated to GSH to keep working. The enzyme that performs this regeneration is glutathione reductase (GR) — and GR is a FAD-flavoprotein that absolutely requires riboflavin. Without adequate B2, the entire glutathione antioxidant system fails. Riboflavin deficiency phenocopies glutathione deficiency at the cellular level. The clinical relevance reaches from red blood cell stability and eye lens cataract prevention to liver detoxification and the rationale behind the GlyNAC anti-aging protocol. This deep-dive covers the GR mechanism, the EGRAC clinical lab marker, the cataract and ocular evidence, and how riboflavin slots into the broader glutathione-replenishment toolkit alongside NAC, glycine, selenium, and sulfur.
Table of Contents
- Glutathione — the Master Cellular Antioxidant
- Glutathione Reductase — the FAD-Flavoprotein
- Why B2 Deficiency Phenocopies Glutathione Deficiency
- EGRAC — the Clinical Lab Marker
- The Eye Lens, GSH, and Cataract Prevention
- Red Blood Cell Stability and Oxidative Hemolysis
- Liver Detoxification and Glutathione Conjugation
- The GlyNAC Protocol and Where Riboflavin Fits
- Selenium, Sulfur, and the Broader Redox Network
- Practical Protocol — Riboflavin for Redox Support
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Glutathione — the Master Cellular Antioxidant
Glutathione is a tripeptide of glutamate, cysteine, and glycine (γ-Glu-Cys-Gly), synthesized inside every cell in two ATP-dependent steps by glutamate-cysteine ligase (GCL, the rate-limiting enzyme) and glutathione synthetase. Cellular concentrations are in the millimolar range — among the highest of any small molecule in the cell — reflecting the central role it plays in redox defense.
Glutathione's antioxidant work depends on the thiol (–SH) group of its cysteine residue. When GSH encounters a reactive oxygen species (hydrogen peroxide, lipid peroxide, hydroxyl radical, or a reactive electrophile), the cysteine thiol donates an electron to neutralize it. The resulting glutathione radical pairs with a second glutathione radical to form glutathione disulfide (GSSG), in which two glutathione molecules are linked through their cysteine sulfurs.
GSSG is biologically inactive as an antioxidant — the working thiols are tied up. For the antioxidant system to keep functioning, GSSG must be reduced back to two molecules of GSH. This regeneration is performed by glutathione reductase.
The healthy cellular ratio is approximately GSH:GSSG = 100:1 in well-perfused tissue under normal conditions. The ratio is one of the most sensitive markers of cellular oxidative stress — when GSH:GSSG drops to 10:1 or below, the cell is in serious redox crisis, and signaling cascades that trigger apoptosis (caspase activation, JNK phosphorylation) begin.
Maintaining the high GSH:GSSG ratio is therefore a continuous, energy-intensive task. The cell does this in two ways:
- De novo synthesis of new glutathione from amino acid precursors (glutamate + cysteine + glycine) — the substrate-supply pathway addressed by the GlyNAC protocol
- Regeneration of existing GSSG back to GSH by glutathione reductase — the riboflavin-dependent pathway
Both pathways must function for cellular redox balance. Substrate supply without regeneration fails; regeneration without substrate supply fails. Riboflavin is the limiting factor for the regeneration arm.
Glutathione Reductase — the FAD-Flavoprotein
Glutathione reductase (GR; gene GSR) is a homodimeric flavoenzyme of the pyridine-nucleotide-disulfide oxidoreductase family (which also includes thioredoxin reductase, lipoamide dehydrogenase, and trypanothione reductase). Each subunit binds:
- One FAD molecule — non-covalently but tightly bound
- One NADPH-binding site
- One GSSG-binding site with a redox-active cysteine disulfide
The reaction GR catalyzes:
GSSG + NADPH + H+ → 2 GSH + NADP+
Mechanism: NADPH (the high-energy electron donor produced by the pentose phosphate pathway) docks on one face of the FAD and transfers a hydride. The reduced FADH2 then reduces the active-site cysteine disulfide, which in turn reduces the bound GSSG, yielding two free GSH. The enzyme returns to its oxidized state and begins another cycle.
The key feature for our purposes: no FAD, no GR activity. Riboflavin status is the upstream determinant of how much functional glutathione reductase a cell can deploy. In riboflavin deficiency, GR is synthesized as the apoenzyme (without bound FAD) and is catalytically inert. Adding riboflavin restores GR activity proportionally to flavin loading.
GR is expressed in essentially every tissue but is particularly abundant in liver, red blood cells, and the eye lens — the three tissues that face the highest oxidative loads and that demonstrate the clearest clinical consequences of B2 deficiency.
Why B2 Deficiency Phenocopies Glutathione Deficiency
A patient with adequate glutathione synthesis but inadequate riboflavin will, paradoxically, present with the clinical features of glutathione deficiency:
- Elevated oxidative stress markers — F2-isoprostanes, 8-hydroxydeoxyguanosine, malondialdehyde all rise
- Low GSH:GSSG ratio on cellular measurement — even when total glutathione is normal, the equilibrium has shifted to the oxidized side because GR cannot regenerate it
- Reduced erythrocyte resistance to oxidative challenge — clinically detectable as hemolysis in response to oxidative stressors
- Increased lens opacity and cataract risk — because the lens depends on GSH and lacks its own glutathione synthesis after maturation
- Reduced Phase II liver conjugation capacity — because Phase II depends on GSH for glutathione-S-transferase reactions
- Impaired methylmercury, acetaminophen, and reactive electrophile detoxification
- Lower nasal/conjunctival mucosal defense against oxidative pollutants
Bonus mechanism: methylation cycle disruption. GSH provides the cysteine substrate that the trans-sulfuration pathway uses to make taurine, sulfate, and additional GSH. Riboflavin deficiency (via low GSH:GSSG and via the parallel MTHFR cofactor failure) compounds disruption of one-carbon metabolism downstream.
The clinical implication: in any patient suspected of glutathione depletion, riboflavin status must be checked or empirically supplemented. Treating with NAC and glycine while leaving the patient with marginal B2 simply increases substrate supply for a regeneration enzyme that cannot keep up. This is the most common cause of incomplete clinical response to glutathione-precursor supplementation.
EGRAC — the Clinical Lab Marker
The most clinically useful lab measure of riboflavin functional status is the erythrocyte glutathione reductase activity coefficient (EGRAC). The assay:
- Measure baseline glutathione reductase activity in lysed red blood cells (this is the apoenzyme + holoenzyme activity that is present at the moment of sampling)
- Add exogenous FAD to a parallel aliquot and re-measure GR activity (this saturates any unliganded apoenzyme with FAD and gives the maximum possible activity)
- EGRAC = activity-with-FAD / activity-without-FAD
Interpretation:
- EGRAC < 1.20 — normal riboflavin status; almost all GR is already loaded with FAD; little additional activity is unlocked by exogenous FAD
- EGRAC 1.20-1.40 — marginal status; some unliganded apoenzyme present
- EGRAC > 1.40 — deficiency; substantial apoenzyme that becomes catalytically active when given FAD — meaning the patient was carrying unliganded enzyme because cellular flavin was insufficient
EGRAC is the gold-standard functional marker because it measures the cellular consequence of B2 status, not just blood concentration. Plasma riboflavin and urinary riboflavin can be normal in patients whose intracellular FAD loading is inadequate (because of poor uptake or recent intake variability), but EGRAC reflects the actual enzymatic deficit.
Practical caveats: EGRAC is offered only at specialized reference laboratories, not routine commercial labs. It is also unreliable in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency, which has its own effect on red blood cell GR activity. For most patients, the empirical approach is to supplement riboflavin 25-100 mg/day and observe the clinical and bright-yellow-urine response.
The Eye Lens, GSH, and Cataract Prevention
The crystalline lens of the eye has one of the highest GSH concentrations of any tissue and one of the most exquisite dependences on GR activity. Several anatomical facts make the lens uniquely vulnerable to riboflavin deficiency:
- The lens is avascular — it receives nutrients by diffusion from the aqueous humor only
- The lens cortex is metabolically active but the central nucleus is post-mitotic and cannot replace damaged proteins
- Lens crystallin proteins are extraordinarily long-lived — the same molecules synthesized in fetal life persist until death
- UV-A exposure generates continuous oxidative stress in the anterior lens
- Cataract is the accumulation of oxidized, cross-linked crystallin aggregates — the irreversible end-stage of lifelong oxidative damage
Glutathione is the lens's primary defense. The lens cortex synthesizes GSH and pumps it into the nucleus, where it scavenges reactive oxygen species generated by UV exposure. The high GSH:GSSG ratio is maintained by GR, which requires FAD, which requires riboflavin.
Multiple epidemiological studies have linked higher dietary riboflavin intake with reduced cataract risk. The mechanism is mechanistically clean: more B2 → more functional GR → higher GSH:GSSG in the lens → less crystallin oxidation → lower cataract incidence. Conversely, populations with chronic marginal riboflavin intake (parts of South Asia and Sub-Saharan Africa with low-dairy, low-meat diets) have correspondingly high age-related cataract incidence.
Bonus mechanism: corneal cross-linking (CXL) for keratoconus. In this clinical procedure, the cornea is saturated with topical riboflavin and then exposed to UV-A light. The riboflavin acts as a UV-activated photosensitizer that generates singlet oxygen and free radicals locally, which cross-link the corneal collagen and stiffen the cornea, halting keratoconus progression. This is the only currently approved disease-modifying treatment for keratoconus and a striking demonstration of how riboflavin's redox chemistry has been weaponized therapeutically.
Practical implication for cataract prevention: adequate dietary riboflavin (RDA + a safety margin = 5-25 mg/day) is the foundational nutrient. For high-risk patients (those with diabetes, chronic UV exposure, family history of early cataract, vegan diet without B-complex supplementation), modest supplementation is reasonable. Higher doses do not provide additional cataract protection beyond GR saturation.
Red Blood Cell Stability and Oxidative Hemolysis
Red blood cells are uniquely vulnerable to oxidative damage. They carry oxygen (which makes them constant sources of reactive oxygen species), they have no mitochondria (so they cannot generate NADPH via the Krebs cycle), and they cannot synthesize new proteins to replace oxidatively damaged ones. Their entire antioxidant defense rests on the pentose phosphate pathway (which generates NADPH from glucose-6-phosphate via G6PD) and the GSH-GR-NADPH loop.
- G6PD generates NADPH in the pentose phosphate pathway
- NADPH is the electron donor for GR
- GR (FAD-flavoprotein) regenerates GSH from GSSG
- GSH scavenges hydrogen peroxide and other ROS via glutathione peroxidase (a selenium-dependent enzyme)
Disruption at any node produces oxidative hemolysis. G6PD deficiency is the classic example (Heinz body hemolytic anemia in response to oxidative drugs like primaquine, fava beans, or sulfa antibiotics). Selenium deficiency reduces glutathione peroxidase activity. And riboflavin deficiency disrupts GR — producing a parallel but distinct hemolytic vulnerability.
The clinical implication: chronic riboflavin deficiency contributes to a mild normocytic, normochromic anemia that is often labeled idiopathic or attributed to chronic disease. It does not respond to iron supplementation (because the iron stores are adequate) but does respond to riboflavin repletion. In patients with G6PD deficiency, optimizing riboflavin status takes on extra importance because the remaining GR capacity must be maximized.
Riboflavin also improves the response to iron-deficiency anemia. B2 enhances iron absorption from the intestine, mobilization from ferritin stores, and incorporation into hemoglobin. Iron-deficiency anemia that does not fully respond to oral iron supplementation often improves dramatically when B2 is added — particularly in vegetarian or vegan patients with marginal dietary B2.
Liver Detoxification and Glutathione Conjugation
Hepatic Phase II detoxification depends on conjugation reactions that attach polar groups to lipid-soluble toxins, making them water-soluble for elimination. Glutathione-S-transferase (GST) is one of the major Phase II enzyme families, conjugating GSH onto a wide range of electrophilic toxins — including reactive metabolites of acetaminophen, polycyclic aromatic hydrocarbons, alkylating agents, and many drugs.
Each GST reaction consumes one GSH. In times of high toxin load, the cellular GSH pool depletes rapidly. The cell's ability to keep detoxifying depends on:
- De novo GSH synthesis from cysteine (NAC-supplementable)
- Regeneration of GSSG back to GSH by riboflavin-dependent GR
The acetaminophen overdose paradigm is the textbook case. NAC saves lives because it replenishes the cysteine substrate needed for new GSH synthesis. But background regeneration of GSSG by GR is also working continuously in the background, and adequate riboflavin status is what allows this regeneration to keep up.
For patients with chronic toxin exposure (industrial chemical workers, smokers, people with chronic alcohol use, those with high-pollution living environments), riboflavin status is a foundational determinant of detoxification capacity. The integrative medicine framing — the "tox-screen plus support" approach — routinely includes a B-complex with adequate B2 alongside NAC, glycine, milk thistle, and the cruciferous vegetables that upregulate Phase II enzyme expression.
The GlyNAC Protocol and Where Riboflavin Fits
The GlyNAC protocol (glycine + N-acetylcysteine) was developed by Rajagopal Sekhar and colleagues at Baylor College of Medicine to restore glutathione in aging adults. The Sekhar 2021/2022 trials documented that older adults have low GSH and that supplementation with N-acetylcysteine (cysteine precursor) + glycine (also a glutathione constituent) for 16-24 weeks restored GSH to youthful levels and produced measurable improvements in inflammation markers, insulin sensitivity, mitochondrial function, walking speed, and grip strength. The GlyNAC deep-dive covers the protocol in detail.
What GlyNAC addresses: substrate supply for de novo glutathione synthesis. Older adults often have inadequate cysteine intake (and reduced cysteine availability from the diet, particularly in low-protein elderly diets), so providing the rate-limiting amino acid precursors restores synthesis capacity.
What GlyNAC does not address: regeneration capacity. A patient with marginal riboflavin status whose GR is partially apoenzyme-loaded cannot fully utilize the new GSH produced by GlyNAC — the cell will continue to accumulate GSSG faster than it can regenerate it, and the cellular GSH:GSSG ratio will remain suboptimal even as total glutathione rises.
The complete protocol for elderly oxidative stress and inflammation:
- N-acetylcysteine 600-1200 mg/day — cysteine precursor for de novo GSH synthesis (Sekhar protocol)
- Glycine 1.3 g/kg/day — the other glutathione constituent that often limits synthesis in elderly (Sekhar protocol)
- Riboflavin 25-50 mg/day — FAD supply for the regeneration arm (the addition that completes the loop)
- Selenium 100-200 mcg/day — glutathione peroxidase cofactor (where GSH actually neutralizes ROS)
- Niacinamide 50-500 mg/day — NAD+/NADP+ precursor, since NADPH is the electron donor for GR
This five-component "complete glutathione" protocol addresses substrate supply (NAC + glycine), regeneration (B2 + niacinamide for NADPH), and downstream use (selenium for GPx). The bare GlyNAC protocol works because most middle-aged Western adults have adequate B2 and selenium incidentally; adding the supporting nutrients explicitly ensures the regeneration loop is intact.
Selenium, Sulfur, and the Broader Redox Network
The cellular redox network is more than just glutathione and GR. Several other components are tightly coupled to B2 status:
- Glutathione peroxidase (GPx) — uses GSH as substrate to reduce hydrogen peroxide and lipid peroxides; requires selenium as a selenocysteine residue. GPx generates the GSSG that GR then regenerates. B2 ↔ selenium synergy.
- Thioredoxin reductase — another FAD-flavoprotein in the same enzyme family as GR; regenerates thioredoxin, a parallel cellular antioxidant. Also riboflavin-dependent.
- Peroxiredoxins — thiol-based peroxidases that use thioredoxin (and hence indirectly require functional thioredoxin reductase — another flavoprotein)
- NADPH (the electron donor for GR) — comes from G6PD activity (the pentose phosphate pathway) and from NADPH-isocitrate dehydrogenase. NADPH availability is the kinetic upstream limit on GR.
- Sulfur amino acids — methionine and cysteine supply the trans-sulfuration pathway that generates the cysteine for de novo GSH synthesis. Methionine cycle integrity (which depends on B2 via MTHFR) feeds into the trans-sulfuration pathway.
The integrated picture: riboflavin status sets the ceiling for both glutathione reductase and thioredoxin reductase activity, the two FAD-flavoprotein guardians of the cellular thiol redox state. Compounding the effect, B2 deficiency (via MTHFR cofactor failure) disrupts the methionine cycle that feeds the trans-sulfuration pathway. The cumulative effect of marginal riboflavin status on cellular redox capacity is therefore larger than any single mechanism implies.
Practical Protocol — Riboflavin for Redox Support
General redox-support dose
- 25-50 mg/day as part of a B-complex — the dose that saturates the cellular flavoenzyme pool in adults without unusual requirements
- Take with food — saturable absorption benefits from slow gastric emptying
- Yellow urine within 24-48 hours confirms absorption
High-need redox-support situations
- Aging adults on GlyNAC — add 50-100 mg/day riboflavin to ensure GR regeneration keeps pace with new GSH synthesis
- Chronic oxidative-stress conditions (chronic infection, cancer survivorship, autoimmune disease, post-radiation): 100-200 mg/day
- Diabetic patients — chronic hyperglycemia produces ongoing ROS; riboflavin status supports the GR-GSH axis. 50-100 mg/day reasonable.
- Heavy metal exposure / chelation therapy — mercury, lead, cadmium all consume GSH; B2 supports the regeneration arm. 50-100 mg/day.
- Chronic alcohol or chemical exposure — supports Phase II detoxification. 25-100 mg/day.
Complete redox-network stack
- Riboflavin 50-100 mg/day — FAD for GR and thioredoxin reductase
- NAC 600-1200 mg/day — cysteine precursor for GSH synthesis
- Glycine 3-6 g/day — second amino acid substrate for GSH
- Selenium 100-200 mcg/day (selenomethionine or yeast-bound) — GPx cofactor
- Niacinamide 100-500 mg/day — NADP+ precursor for the NADPH supply
- Alpha-lipoic acid 600 mg/day — antioxidant network regeneration including vitamins C and E
- Vitamin C 500-1000 mg/day — aqueous-phase antioxidant; spares GSH
- Vitamin E 200-400 IU/day (mixed tocopherols) — lipid-phase antioxidant
Monitoring
- EGRAC if available at a specialty reference lab
- Practical surrogates: plasma F2-isoprostanes (oxidative stress marker), hs-CRP (inflammation), patient-reported fatigue and exercise tolerance
- Bright yellow urine is the cheap home marker of adequate riboflavin absorption
Cautions
- G6PD deficiency — supplementation with riboflavin is safe and beneficial, but EGRAC interpretation is confounded by altered erythrocyte enzyme activity in G6PD patients. Use clinical and exposure-based assessment rather than EGRAC.
- Light degradation — store riboflavin and B-complex supplements in dark, opaque containers; protect food sources from light exposure
- Absorption saturation — single doses above ~27 mg are inefficiently absorbed; divide larger daily totals
- No conflict with NAC, glycine, or selenium — the regeneration-arm role is fully complementary to substrate-supply and downstream-effector nutrients
- Hepatic dysfunction — severe liver disease impairs riboflavin-to-FAD conversion; use R5P (riboflavin-5′-phosphate, the active FMN form) in such cases
- Drug interactions are minimal; tetracyclines, phenothiazines, and tricyclics may slightly reduce riboflavin utilization but the clinical relevance is small at supplemental doses
- Pregnancy and lactation — standard doses are safe and required; mega-doses for therapeutic purposes should be physician-directed
Key Research Papers
- Karplus PA & Schulz GE (1989). Substrate binding and catalysis by glutathione reductase as derived from refined enzyme: substrate crystal structures at 2 Å resolution. J Mol Biol. — PubMed
- Powers HJ (2003). Riboflavin (vitamin B-2) and health. American Journal of Clinical Nutrition. — PubMed
- Sauberlich HE (1984). Implications of nutritional status on human biochemistry, physiology, and health (EGRAC discussion). Clinical Biochemistry. — PubMed
- Cumming RG et al. (2000). Diet and cataract: the Blue Mountains Eye Study (riboflavin and cataract risk). Ophthalmology. — PubMed
- Leske MC et al. (1991). Antioxidant vitamins and nuclear opacities: the Lens Opacities Case-Control Study. Ophthalmology. — PubMed
- Wollensak G et al. (2003). Riboflavin/ultraviolet-A induced collagen crosslinking for the treatment of keratoconus. American Journal of Ophthalmology. — PubMed
- Sekhar RV et al. (2021). GlyNAC supplementation in aging humans: glutathione restoration with N-acetylcysteine + glycine. Clinical and Translational Medicine. — PubMed
- Powers HJ et al. (2011). Correcting a marginal riboflavin deficiency improves hematological status in young women in the United Kingdom. American Journal of Clinical Nutrition. — PubMed
- Ashoori M & Saedisomeolia A (2014). Riboflavin (vitamin B&sub2;) and oxidative stress: a review. British Journal of Nutrition. — PubMed
- Beutler E (1969). Effect of flavin compounds on glutathione reductase activity: in vivo and in vitro studies. Journal of Clinical Investigation. — PubMed
- Lopez-Mirabal HR & Winther JR (2008). Redox characteristics of the eukaryotic cytosol. Biochim Biophys Acta. — PubMed
PubMed Topic Searches
- PubMed: glutathione reductase FAD riboflavin
- PubMed: EGRAC riboflavin status
- PubMed: riboflavin cataract lens glutathione
- PubMed: riboflavin oxidative stress GSH GSSG
- PubMed: corneal cross-linking keratoconus
Connections
- Vitamin B2 Overview
- B2 Benefits Hub
- B2 for Migraine Prevention
- B2 Mitochondrial Cofactor
- B2 for MTHFR & Methylation
- Glutathione (Hub)
- GlyNAC Protocol for Aging
- Glutathione Liver Detoxification
- NAC
- Glutathione (Pathway)
- NAC as Glutathione Precursor
- Glycine
- Selenium
- Sulfur
- Alpha Lipoic Acid
- Oxidative Stress
- Liver Cleansing
- Anemia
- Vitamin C
- Vitamin E