Hypervitaminosis A (Vitamin A Toxicity): Symptoms, Causes, and Risks
Hypervitaminosis A simply means too much vitamin A in the body — and here is the single most important thing to understand: it is almost never caused by food. It is caused by preformed vitamin A (retinol) from high-dose supplements, certain prescription acne and skin medicines, and, classically, by eating very large amounts of liver or cod-liver oil. The colorful plant form — beta-carotene in carrots, sweet potatoes, and leafy greens — is essentially safe, because your body only converts what it needs. The danger lies in retinol, because vitamin A is fat-soluble and the body cannot simply flush the excess out in urine; it stores it in the liver, where it can build up over months or years. A single enormous dose can cause an acute illness (headache, nausea, peeling skin), but the more insidious problem is chronic toxicity, which can quietly injure the liver, weaken bones, and raise pressure around the brain — and one form, taken in pregnancy, can cause serious birth defects. This hub explains what hypervitaminosis A is, why excess retinol is dangerous, why it often builds silently, what causes it, and how it is diagnosed and treated — with deep-dive pages for each major harm it can produce. Vitamin A toxicity is preventable: it is overwhelmingly a problem of supplements and medicines, not of a normal diet.
Symptom Deep-Dive Pages
Liver Damage
The liver is where vitamin A is stored, so it is the first organ harmed by chronic excess. How retinol overload activates stellate cells and drives scarring (fibrosis) toward cirrhosis — and why blood tests can look normal until late.
Bone & Joint Pain
Why too much vitamin A makes bones ache, raises fracture risk, and can cause new bone to pile up at tendon attachments (hyperostosis) — and the surprising evidence that even modestly high long-term intake may thin the skeleton.
Headache & Brain Pressure
One of the most striking effects of vitamin A excess is a rise in pressure around the brain (pseudotumor cerebri), causing severe headaches and visual changes that can threaten sight. How it mimics a brain tumor — and reverses when the source is stopped.
Birth Defects (Pregnancy)
The most serious risk of all: high-dose retinol and retinoid acne drugs (such as isotretinoin) are powerful teratogens that can cause severe birth defects. Why pregnancy demands special caution — and where the real, evidence-based limits lie.
Table of Contents
- Symptom Deep-Dive Pages
- What Is Hypervitaminosis A?
- Why Excess Vitamin A Is Dangerous
- Why Chronic Toxicity Often Builds Silently
- Common Causes of Vitamin A Toxicity
- How Hypervitaminosis A Is Diagnosed
- How Vitamin A Toxicity Is Treated
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
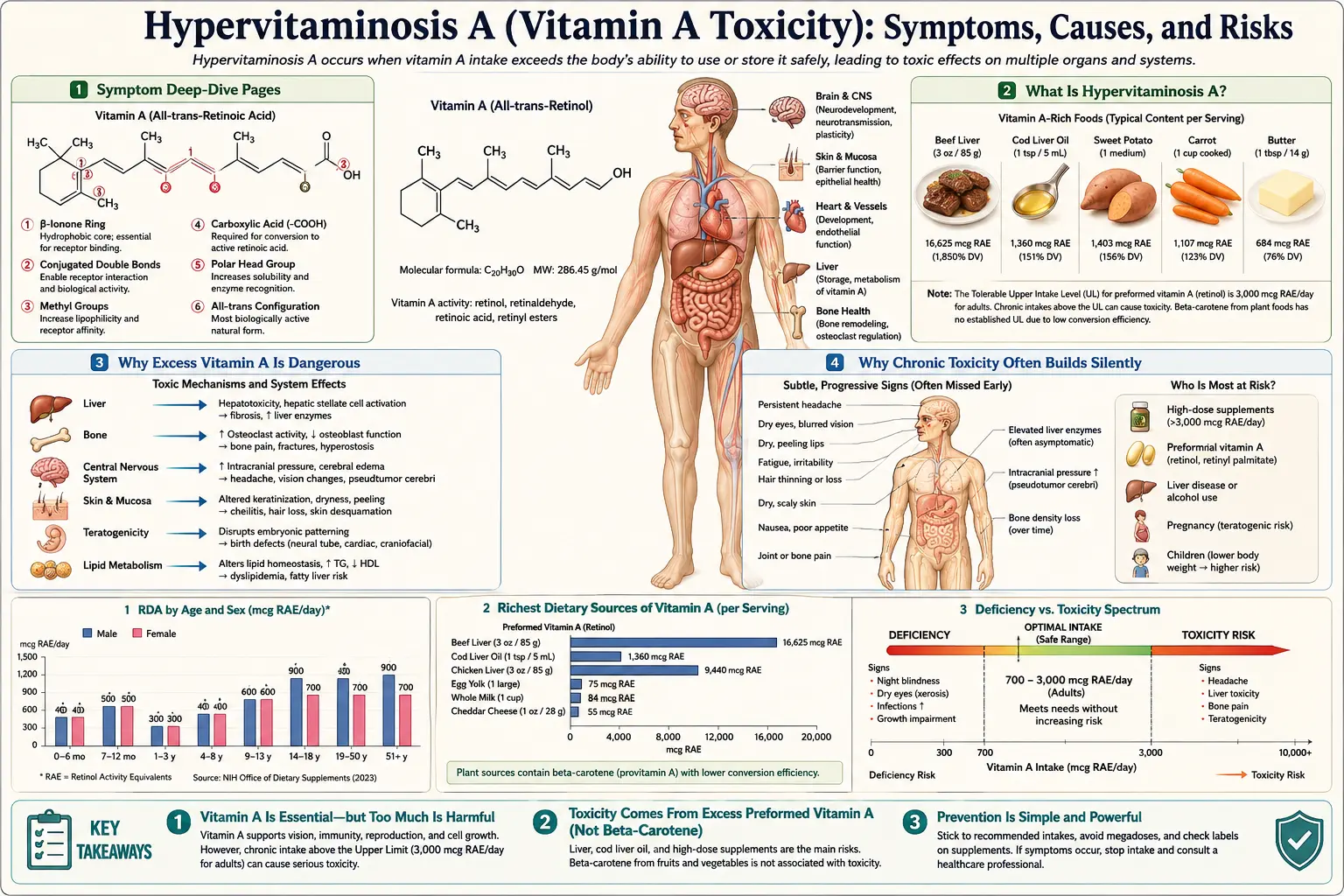
What Is Hypervitaminosis A?
Vitamin A is an essential, fat-soluble nutrient your body needs for vision, immune defense, skin, and the growth of the developing baby in pregnancy (the Vitamin A overview covers what it does and where it comes from). Hypervitaminosis A is the medical term for having too much of it in the body — an excess large enough to cause harm. Because vitamin A is fat-soluble, it is stored, mostly in the liver, rather than washed out in urine the way an excess of a water-soluble vitamin such as vitamin C would be. That single fact — it accumulates — is the root of why too much can be dangerous.
The most important distinction in this entire topic is between the two forms of vitamin A, because only one of them causes toxicity:
- Preformed vitamin A (retinol and retinyl esters) — the "ready-made" active form, found in animal foods (liver, fish oils, egg yolk, dairy), in many supplements and multivitamins, and in prescription retinoid medicines. This is the form that causes hypervitaminosis A. The body absorbs it efficiently and stores the surplus.
- Provitamin A carotenoids (mainly beta-carotene) — the plant pigments in carrots, sweet potatoes, pumpkin, spinach, and other orange, yellow, and dark-green produce. The body converts these into vitamin A only as needed, and that conversion is tightly down-regulated when stores are full. As a result, beta-carotene from food does not cause vitamin A toxicity. Eating a great deal of it can turn the skin a harmless orange-yellow (a condition called carotenemia), but this is cosmetic and reversible, not poisoning.
Hypervitaminosis A comes in two clinical pictures, distinguished by how the excess arrives:
- Acute toxicity — from a single very large dose (or a few large doses over a short time). The classic, dramatic historical example is Arctic explorers who became ill after eating polar bear or seal liver, which is extraordinarily rich in retinol. Acute toxicity causes a sudden illness — severe headache, nausea and vomiting, dizziness, blurred vision, and, a day or two later, peeling of the skin. It is uncommon and usually resolves once the source stops.
- Chronic toxicity — from taking too much, day after day, for weeks to years. This is the more common and more concerning form. It builds up gradually and can injure the liver, weaken bones, raise pressure around the brain, dry and crack the skin and lips, cause hair loss, and produce bone and joint pain. Because it accumulates, a person may feel fine for a long time before problems surface.
For scale, the official intake guidance is helpful. For most adults the Recommended Dietary Allowance (RDA) for vitamin A is about 700–900 micrograms of retinol activity equivalents (RAE) per day (older labels use International Units; roughly 2,300–3,000 IU). The Tolerable Upper Intake Level (UL) for adults — the most preformed vitamin A you should get per day from all sources combined — is 3,000 micrograms RAE (about 10,000 IU). Crucially, that UL applies to preformed vitamin A only; it does not limit beta-carotene from food. Chronic toxicity generally requires intakes well above the UL sustained over time, though — as the bone section explains — there is evidence that even intakes only modestly above the RDA, kept up for years, may carry some skeletal risk.
Why Excess Vitamin A Is Dangerous
If your body needs vitamin A, why is a surplus harmful? The answer comes down to two things: vitamin A is a powerful signaling molecule that acts almost like a hormone, and the body has no easy way to dump the excess. Understanding both makes the pattern of harm make sense.
It is stored, not excreted. Water-soluble vitamins are forgiving — take more than you need and most of the surplus leaves in the urine. Vitamin A is the opposite. As a fat-soluble vitamin it is held in the body, and the great majority is warehoused in the liver, inside specialized cells called hepatic stellate cells. These cells are essentially the body's vitamin A storehouse. When intake of retinol chronically exceeds what the body needs, these stores overflow. The excess retinol and its byproducts then become toxic to the very cells storing them and to surrounding liver tissue.
It is a potent signaling molecule. Inside the body, vitamin A is converted to retinoic acid, which binds to receptors in the cell nucleus and switches genes on and off — controlling how cells grow, specialize, and behave. This is exactly why vitamin A is essential, and exactly why too much is dangerous: flood the system with this signal and it disrupts normal cell behavior across many tissues. That is the unifying reason a single nutrient can harm such different parts of the body. The major harms, each explored on its own deep-dive page, are:
- Liver injury. Because the liver is the storage depot, it bears the brunt. Overloaded stellate cells become "activated," transform into scar-producing myofibroblasts, and lay down fibrous tissue. Over time this can progress from a fatty, enlarged liver to fibrosis and even cirrhosis, sometimes with portal hypertension. The liver is often the first organ damaged by chronic excess. See Liver Damage and the broader Liver Disease and Cirrhosis pages.
- Bone and joint harm. Retinoic acid pushes bone-dissolving cells (osteoclasts) to be more active and reins in bone-building cells (osteoblasts), tilting the balance toward bone loss. The result can be bone pain, a higher risk of fracture, and, with heavy chronic exposure, excess bony growth at tendon and ligament attachments (hyperostosis). See Bone & Joint Pain.
- Raised pressure around the brain. Vitamin A excess is a recognized cause of pseudotumor cerebri (idiopathic intracranial hypertension) — a rise in the pressure of the fluid surrounding the brain. It produces severe headaches, vision disturbances, and swelling of the optic nerve that, untreated, can damage sight. See Headache & Brain Pressure.
- Harm to a developing baby. Because retinoic acid orchestrates the genes that pattern an embryo, an excess at the wrong time is a powerful teratogen — it can cause serious birth defects of the face, heart, and brain. This is the most serious risk of all and the reason high-dose vitamin A and retinoid acne drugs are strictly avoided in pregnancy. See Birth Defects (Pregnancy).
Alongside these major harms are the more visible, less dangerous signs of chronic excess: dry, rough, peeling skin; cracked lips; hair loss; brittle nails; and a generally unwell, achy feeling. These are uncomfortable but reversible warnings that intake is too high.
Why Chronic Toxicity Often Builds Silently
One of the most important features of vitamin A toxicity — and one of the easiest to miss — is that the chronic form can build up quietly over months or years before causing obvious illness. Acute toxicity announces itself with a dramatic, sudden illness. Chronic toxicity does the opposite: it accumulates in the liver, often outpacing any symptoms, so a person can be steadily building dangerous stores while feeling more or less normal.
Why is it so quiet? Because the liver is a large, patient reservoir. It can absorb a substantial surplus of retinol into its stellate cells before stores are overwhelmed and damage begins. During that build-up phase there may be no symptoms at all, or only vague ones — mild fatigue, occasional headache, some dry skin — that are easy to attribute to anything else. By the time clearer signs appear (an enlarging liver, bone pain, persistent headaches), the excess may have been accumulating for a long time.
This makes the laboratory picture genuinely tricky, and it is worth understanding why a blood test can be falsely reassuring. The blood level of vitamin A (serum retinol) is tightly controlled and does not reliably reflect how much is stored in the liver. The body holds serum retinol within a narrow range across a wide span of liver stores, so someone can have a substantially overloaded liver while their blood retinol still reads normal or only mildly high. In other words, a "normal vitamin A level" on a routine blood test does not rule out chronic toxicity. This is one of the clearest examples in nutrition of a test that can mislead if interpreted naively, and it is why doctors lean on the history (how much vitamin A, from what sources, for how long) at least as much as on the number.
The practical consequence is that prevention and a careful intake history matter more than waiting for a symptom or a lab result. People most likely to drift into chronic excess without realizing it include:
- Those taking high-dose vitamin A supplements or several products that each contain it (a multivitamin, a separate vitamin A pill, cod-liver oil, and a fortified food can quietly add up).
- People who eat liver very frequently — beef, chicken, pork, or especially cod liver — given how concentrated retinol is in liver.
- Anyone using retinoid medicines (for acne or psoriasis), which are chemical relatives of vitamin A and add to the body's total retinoid load.
- People with liver disease, whose damaged liver may handle and store vitamin A abnormally, and in whom toxicity can develop at lower intakes.
The take-home message mirrors the rest of this topic: feeling fine does not prove your intake is safe. For vitamin A, the way to stay out of trouble is to keep preformed intake sensible from the start — not to rely on your body to sound an alarm.
Common Causes of Vitamin A Toxicity
Vitamin A toxicity is, in almost every case, a problem of preformed retinol arriving faster than the body needs — and the sources are usually identifiable. Here are the causes worth knowing, roughly in order of how often they matter today.
- High-dose supplements — the leading modern cause. Standalone vitamin A capsules, high-potency multivitamins, and "immune" or "eye health" formulas can deliver many times the RDA. Toxicity becomes a real risk when supplemental preformed vitamin A is taken at high doses for a long time, and especially when several products that each contain vitamin A are combined. Reading labels for the amount of preformed vitamin A (retinol/retinyl palmitate or acetate), not just total vitamin A, is the single most useful habit for avoiding excess.
- Cod-liver oil and fish-liver oils. These traditional supplements are rich in preformed vitamin A. Taken at modest doses they are reasonable, but large or doubled-up doses — sometimes taken for omega-3s or vitamin D without realizing how much vitamin A comes along — can push intake over the line. See Cod Liver.
- Eating liver very frequently. Liver is the most vitamin-A-dense food there is; a single serving of beef or cod liver can far exceed a day's RDA. Liver is a superb, nutritious food eaten occasionally, but eaten daily it can contribute to chronic excess. See Beef Liver and Chicken Liver. (This is the modern echo of the polar-bear-liver poisoning that historically defined acute toxicity.)
- Prescription retinoid medicines. Drugs such as isotretinoin (for severe acne), acitretin (for psoriasis), and bexarotene are chemical relatives of vitamin A. They have their own real benefits and risks and are not "vitamin A" per se, but they add to the body's retinoid signaling and can produce overlapping effects — dry skin and lips, bone changes, raised brain pressure, and, critically, the same severe risk to a pregnancy. They must be managed by the prescriber, never combined casually with high-dose vitamin A.
- Liver disease — lowering the threshold. A damaged liver stores and processes vitamin A abnormally, so people with existing liver disease can develop toxicity at intakes a healthy liver would tolerate. In this setting even ordinary supplement doses warrant medical guidance.
- What does not cause it: beta-carotene from food. It bears repeating because it is the most common misunderstanding. Carrots, sweet potatoes, squash, spinach, and other carotenoid-rich produce do not cause vitamin A toxicity, because the body converts beta-carotene to vitamin A only as needed. The worst that heavy intake does is tint the skin orange (carotenemia), which is harmless and fades. (Separately, high-dose beta-carotene supplements have their own caution in smokers regarding lung-cancer risk — but that is a distinct issue from vitamin A toxicity.) See Sweet Potatoes and Spinach.
As with most nutrient problems, these causes often combine. A person taking a daily multivitamin and a separate vitamin A capsule and cod-liver oil, who also enjoys liver once a week, may be well over the UL from the sum of reasonable-sounding parts — none of which alone would have done it.
How Hypervitaminosis A Is Diagnosed
Diagnosing vitamin A toxicity is, more than almost any other nutrient problem, a matter of putting the story together with the body's signs — not simply ordering one blood test. That is because, as explained above, the blood level can be misleading. A careful diagnosis usually rests on three legs.
- The intake history — the most important clue. A doctor will ask in detail about every source of preformed vitamin A: supplements (including multivitamins and "stacked" products), cod-liver oil, how often liver is eaten, and any retinoid medicines. A pattern of high preformed intake sustained over time, together with fitting symptoms, often makes the diagnosis before any lab is drawn. Bringing the actual bottles and labels to the appointment is genuinely useful.
- The clinical signs. The body offers visible and reportable evidence — dry, peeling skin and cracked lips, hair loss, bone or joint pain, headaches with visual changes, an enlarged or tender liver. The pattern of these together points toward toxicity, and they guide which deep-dive harm (liver, bone, brain) needs attention.
- Targeted testing — chosen to fit the picture. Tests are used to confirm harm and rule out other causes, rather than to "measure toxicity" with a single number:
- Serum retinol. A blood vitamin A level can be checked, and it may be elevated — but a normal level does not exclude chronic toxicity, because blood levels stay within a narrow range across a wide span of liver stores. Fasting retinyl ester levels (a different fraction) are a somewhat better signal of excess and may be measured in specialized settings. The key point is that the number is interpreted cautiously, never in isolation.
- Liver function tests. Because the liver is the main target, blood tests of liver enzymes and function are often the most useful labs. See the Liver Function Tests page; imaging or, rarely, a liver biopsy may be used when significant liver injury is suspected.
- Imaging or eye examination as needed. X-rays can show the excess bone growth (hyperostosis) of chronic toxicity, and when raised brain pressure is suspected, an eye examination (looking for optic-nerve swelling) and brain imaging help confirm pseudotumor cerebri and exclude an actual mass.
A reassuring corollary of how toxicity develops is how it is confirmed: when symptoms and signs clearly improve after the vitamin A source is stopped, that response itself supports the diagnosis. In short, the history points to it, the signs corroborate it, targeted tests confirm the harm, and improvement on withdrawal seals it.
How Vitamin A Toxicity Is Treated
The good news about hypervitaminosis A is that its cornerstone treatment is simple and, for most people, highly effective: stop the source of excess vitamin A. Because the toxicity comes from too much retinol coming in, removing that input lets the body gradually clear the surplus and lets affected tissues recover.
- Stop all preformed vitamin A. This means discontinuing vitamin A supplements, cod-liver oil, and high-vitamin-A foods such as liver, and reviewing every multivitamin and "stacked" product for hidden preformed vitamin A. Beta-carotene from ordinary fruit and vegetables does not need to be restricted. Retinoid medicines should never be stopped or changed on your own — that is a decision for the prescriber, who will weigh the skin condition against the toxicity.
- Expect gradual, not instant, recovery. Because vitamin A is stored in the liver and released slowly, levels and symptoms come down over weeks to months rather than days. For many people, especially those caught before serious organ damage, the milder effects — headaches, skin changes, hair loss, bone pain — resolve substantially once intake stops and stores normalize. Acute toxicity from a single big dose typically settles on its own once no more is taken.
- Treat the specific harm. Where toxicity has caused real organ effects, those are managed in their own right:
- Raised brain pressure (pseudotumor cerebri) may need medicines to reduce cerebrospinal-fluid pressure and close monitoring of vision, because the threat to sight is the priority; it usually improves once vitamin A is withdrawn. (Details on the Headache & Brain Pressure page.)
- Liver injury is managed by stopping the offending intake, monitoring liver tests, and treating complications; established scarring (fibrosis or cirrhosis) may not fully reverse, which is exactly why prevention and early recognition matter. (See Liver Damage.)
- Bone pain and skeletal changes generally ease after withdrawal, and care focuses on pain relief and supporting bone health. (See Bone & Joint Pain.)
- Supportive care. In an acute, very large overdose, treatment is supportive — managing dehydration from vomiting, relieving symptoms, and observation. There is no routine antidote; the body's own clearance, once intake stops, does the work.
- Prevent recurrence. Because toxicity is so preventable, the lasting part of treatment is education: knowing which products and foods carry preformed vitamin A, respecting the adult UL of about 3,000 micrograms RAE (10,000 IU) per day from all preformed sources, and being especially careful in pregnancy and in liver disease. A clinician or dietitian can help rebuild a safe, balanced intake.
The reassuring bottom line is that, recognized in time, most vitamin A toxicity reverses when the source is stopped. The aim of understanding it is to stop the excess before it does lasting damage to the liver, bones, or, above all, a developing baby.
When to Seek Care / Red Flags
Because chronic vitamin A toxicity builds slowly, the most useful "red flag" is often a situation rather than a symptom: if you are taking high-dose vitamin A, doubling up on supplements that each contain it, eating liver very often, or using a retinoid medicine, that pattern alone is worth reviewing with a clinician — before symptoms appear. That said, certain signs mean you should be evaluated promptly, and a few are urgent. Seek prompt medical care if you have any of the following:
- Severe or persistent headache with visual changes — blurred or double vision, brief blackouts of vision, or a pulsing noise in the ears. These can signal raised pressure around the brain, which can threaten sight and needs urgent assessment.
- Signs of liver trouble — yellowing of the skin or eyes (jaundice), pain or swelling in the upper-right abdomen, unusual bruising, or dark urine.
- Severe bone or joint pain — especially aching that is new, persistent, and not explained by injury, or any fracture from a minor knock.
- Acute illness after a very large dose — sudden severe headache, repeated vomiting, dizziness, and (after a day or two) peeling skin, particularly after eating a large amount of liver or taking a big dose of a vitamin A product.
- Pregnancy or planning pregnancy while exposed to high vitamin A or a retinoid — this is the most important caution on the page. If you are pregnant, could be pregnant, or are trying to conceive and are taking high-dose vitamin A, cod-liver oil, or any retinoid acne or psoriasis medicine, contact your clinician right away. (Full details on the Birth Defects (Pregnancy) page.)
People at higher risk — those on high-dose or stacked supplements, frequent liver eaters, anyone using retinoid medicines, and people with liver disease — should have a low threshold for getting checked, because in these settings excess can accumulate without warning. When in doubt, bring your supplement bottles to a clinician and review the numbers together; for related symptoms see Headache and the broader Liver Disease page.
Key Research Papers
- Penniston KL, Tanumihardjo SA (2006). The acute and chronic toxic effects of vitamin A. American Journal of Clinical Nutrition;83(2):191-201. — DOI: 10.1093/ajcn/83.2.191
- Olson JM, Ameer MA, Goyal A (2025). Vitamin A Toxicity. StatPearls [NCBI Bookshelf, NBK532916]. — NCBI Bookshelf
- Geubel AP, De Galocsy C, Alves N, et al. (1991). Liver damage caused by therapeutic vitamin A administration: estimate of dose-related toxicity in 41 cases. Gastroenterology;100(6):1701-1709. — PubMed
- Vitamin A toxicity and hepatic pathology: a comprehensive review (2025). World Journal of Hepatology;17(8):article 107738. — DOI: 10.4254/wjh.v17.i8.107738
- Michaelsson K, Lithell H, Vessby B, Melhus H (2003). Serum Retinol Levels and the Risk of Fracture. New England Journal of Medicine;348(4):287-294. — DOI: 10.1056/NEJMoa021171
- Promislow JHE, Goodman-Gruen D, Slymen DJ, Barrett-Connor E (2002). Retinol Intake and Bone Mineral Density in the Elderly: The Rancho Bernardo Study. Journal of Bone and Mineral Research;17(8):1349-1358. — DOI: 10.1359/jbmr.2002.17.8.1349
- Jacobson DM, Berg R, Wall M, et al. (1999). Serum vitamin A concentration is elevated in idiopathic intracranial hypertension. Neurology;53(5):1114-1118. — DOI: 10.1212/WNL.53.5.1114
- Feldman MH, Schlezinger NS (1970). Benign Intracranial Hypertension Associated With Hypervitaminosis A. Archives of Neurology;22(1):1-7. — DOI: 10.1001/archneur.1970.00480190005001
- Rothman KJ, Moore LL, Singer MR, et al. (1995). Teratogenicity of High Vitamin A Intake. New England Journal of Medicine;333(21):1369-1373. — DOI: 10.1056/NEJM199511233332101
- Lammer EJ, Chen DT, Hoar RM, et al. (1985). Retinoic Acid Embryopathy. New England Journal of Medicine;313(14):837-841. — DOI: 10.1056/NEJM198510033131401
- National Institutes of Health, Office of Dietary Supplements. Vitamin A and Carotenoids — Health Professional Fact Sheet (intake, Upper Limit, and toxicity). — NIH Office of Dietary Supplements
PubMed Topic Searches
- PubMed — Hypervitaminosis A: toxicity, symptoms, and diagnosis
- PubMed — Vitamin A hepatotoxicity, stellate cells, and fibrosis
- PubMed — Retinol intake, bone mineral density, and fracture risk
- PubMed — Vitamin A, pseudotumor cerebri, and intracranial hypertension
- PubMed — Vitamin A teratogenicity, retinoids, and birth defects
Connections
- Vitamin A Toxicity: Liver Damage
- Vitamin A Toxicity: Bone & Joint Pain
- Vitamin A Toxicity: Headache & Brain Pressure
- Vitamin A Toxicity: Birth Defects (Pregnancy)
- Vitamin A Overview
- Vitamin A Deficiency Hub
- Vitamin A Benefits Hub
- Vitamin A Food Sources
- Liver Function Tests
- Liver Disease
- Cirrhosis
- Headache
- Beef Liver
- Cod Liver
- Sweet Potatoes