Hypervitaminosis A (Vitamin A Toxicity): Birth Defects (Pregnancy)
Of all the ways too much vitamin A can harm the body, the one that matters most in pregnancy is also the most preventable: in high doses, preformed vitamin A (retinol and its relatives) is a known human teratogen — a substance that can disrupt how a baby's face, heart, and brain are built in the first weeks after conception, often before a woman even knows she is pregnant. The single largest source of this risk is not food and not an ordinary multivitamin; it is the acne drug isotretinoin (and other oral retinoids), which are so reliably damaging to a developing baby that they are dispensed only under strict pregnancy-prevention programs. An honest caveat belongs up front: a normal diet and a standard prenatal vitamin do not cause this, and beta-carotene from fruits and vegetables is not the culprit. This page explains exactly where the danger lies, the biology behind it, and how to stay on the safe side of a line that is, fortunately, easy to respect.
Table of Contents
- What This Risk Looks Like
- The Mechanism: Why Excess Vitamin A Disrupts Development
- An Honest Look: Birth Defects Have Many Causes
- When Vitamin A Is the Likely Culprit
- Where the Excess Comes From
- Getting Checked & Knowing Your Numbers
- Prevention and What to Do
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
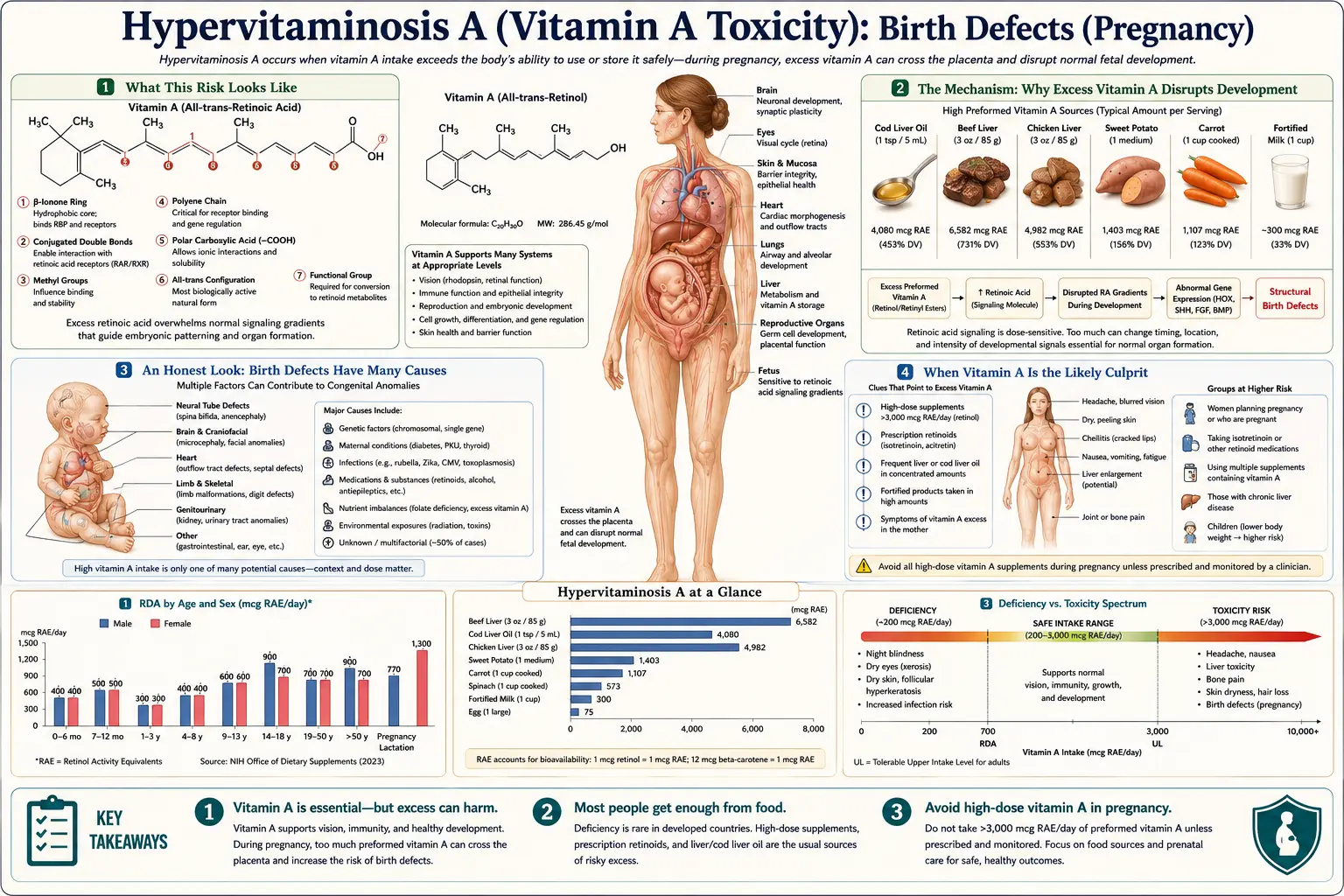
What This Risk Looks Like
This is an unusual entry among vitamin A’s toxic effects, because the person carrying the risk — the pregnant woman — usually feels nothing at all. Excess vitamin A in pregnancy does not announce itself with a headache or nausea the way an acute overdose can. The harm happens silently, inside the developing embryo, during a window so early that many pregnancies are not yet recognized. By the time anyone could “feel” that something is wrong, the critical period of organ formation has often already passed.
What the baby can experience, when high-dose preformed vitamin A interferes with early development, is a recognizable pattern that doctors call retinoic acid embryopathy. Not every exposed pregnancy is affected, but when defects do occur they tend to cluster in the structures that are being sculpted earliest:
- Craniofacial differences. Malformations of the ears (including small or absent external ears, called microtia or anotia), a small jaw, cleft palate, and other changes to the shape of the face and skull.
- Heart defects. Malformations of the heart and great vessels — the large arteries leaving the heart — which form during the same early weeks.
- Brain and nervous-system defects. Abnormal development of the brain, including hydrocephalus (fluid build-up) and malformations of the cerebellum, sometimes with later effects on learning and thinking even when the outward appearance is normal.
- Thymus and immune-tissue defects. Underdevelopment of the thymus gland, part of the immune system, which arises from the same embryonic tissue as some of the affected facial structures.
- Pregnancy loss. A markedly increased risk of miscarriage is part of the same picture.
The reason these particular structures are so vulnerable is not random, and the next section explains why. The essential point for now is that the danger is real, specific, and tied to a precise early window — which is exactly what makes prevention, rather than detection, the whole game.
The Mechanism: Why Excess Vitamin A Disrupts Development
To understand why too much vitamin A is dangerous to an embryo, it helps to know that vitamin A is not merely a nutrient the body burns for fuel — it is a master signaling molecule that helps tell embryonic cells what to become and where to go. The body converts retinol into an active form called retinoic acid, and retinoic acid acts almost like a hormone: it slips into the nucleus of a cell, binds to receptors on the DNA, and switches whole sets of developmental genes on or off.
During the first weeks after conception, retinoic acid is one of the chemical signposts that lays out the body plan — the gradient that helps establish the head-to-tail axis and guides the formation of the face, the heart’s outflow tract, the hindbrain, and the structures derived from a migrating population of embryonic cells called the neural crest. Many of the structures harmed in retinoic acid embryopathy — the outer ears, the jaw, parts of the heart, the thymus — are built by neural-crest cells, which are exquisitely sensitive to retinoic acid levels.
Here is the core problem: this signal works only within a narrow, carefully controlled range. The embryo normally regulates its own retinoic acid concentration with great precision. Flood the system with extra vitamin A and you scramble the signposts. Genes that should be off turn on; genes that should be on at one location switch on in the wrong place; neural-crest cells that should migrate and survive instead die or end up misplaced. The result is not generalized poisoning but misbuilding — organs that form imperfectly because the instructions guiding them were corrupted.
An analogy. Picture the embryo as a vast construction site working from a set of blueprints, where retinoic acid is the ink the blueprints are printed in. A faint, exact amount of ink renders the drawings perfectly. Pour a bottle of extra ink across the plans and the lines blur and bleed into one another: the foreman can no longer tell where the ear wall should rise or where the heart’s plumbing should connect. The workers keep building — they just build from smeared instructions. That is why the damage is structural and concentrated in the parts being drawn during the days the excess arrives.
This also explains the timing. The most dangerous exposure is in the first trimester, especially the third through the eighth week after conception, when these structures are actively forming. It explains the dose-dependence, too: the active drugs (isotretinoin and other oral retinoids) are retinoic acid or are rapidly converted to it, so they deliver the disruptive signal directly, which is why they are far more dangerous than the retinol in food or supplements. And it explains why beta-carotene is different (covered below): the body converts beta-carotene to vitamin A only as needed and throttles that conversion, so it does not flood the embryo the way a large dose of preformed retinol or a retinoid drug can.
An Honest Look: Birth Defects Have Many Causes
It would be misleading to leave the impression that vitamin A is a common cause of birth defects, so it is worth being plain: the great majority of birth defects have nothing to do with vitamin A. Most congenital differences arise from causes that have no connection to diet at all — and excess vitamin A, outside of retinoid drugs, is an uncommon cause.
The major contributors to birth defects include:
- Genetic and chromosomal causes — conditions such as Down syndrome and many inherited single-gene disorders, which together account for a large share of structural differences.
- Random developmental events — a great many birth defects are simply multifactorial or sporadic, with no identifiable cause despite a normal pregnancy.
- Folate (folic acid) deficiency — insufficient folate around conception raises the risk of neural-tube defects such as spina bifida, which is precisely why folic acid supplementation before and during early pregnancy is recommended.
- Other medications and substances — alcohol (fetal alcohol spectrum disorders), certain seizure medicines, some blood thinners, and a number of other drugs are established teratogens in their own right.
- Maternal infections and illnesses — infections such as rubella, and poorly controlled conditions such as diabetes, can disrupt development.
So a baby born with a heart or facial difference is, in the overwhelming majority of cases, not the result of vitamin A. The face, heart, and brain malformations linked to retinoids can also be produced by many of the causes above, and they overlap with other genetic syndromes — which is exactly why no one can read a vitamin A cause backward from the defects alone. What makes vitamin A stand out is not how often it is to blame, but how preventable it is when it is: unlike genetics or random chance, an excess-retinoid exposure is something a person and their clinician can simply avoid.
When Vitamin A Is the Likely Culprit
Because the resulting defects are not unique to vitamin A, suspicion comes almost entirely from the exposure history — what was taken, in what dose, and when. The situations that point toward a vitamin A cause are specific and, encouragingly, mostly recognizable in advance:
- An oral retinoid taken during a pregnancy. This is by far the strongest signal. Isotretinoin (a powerful oral acne medicine), acitretin (used for severe psoriasis), and oral tretinoin or related compounds are recognized teratogens. Acitretin is especially concerning because it can persist in the body for many months — even years — after the last dose, which is why pregnancy must be avoided for an extended period after stopping it.
- Very high-dose preformed vitamin A supplements. Large daily doses of retinol — well above what a standard prenatal vitamin provides — especially in the first trimester. The classic study below found increased risk above roughly 10,000 IU of preformed vitamin A per day.
- Routinely eating large amounts of liver. Liver (beef, pork, chicken, and especially cod liver and fish liver) is extraordinarily rich in preformed vitamin A — a single serving can exceed a day’s requirement many times over. Frequent liver consumption in pregnancy is the one dietary pattern that can plausibly reach a concerning intake, which is why several countries advise pregnant women to limit it.
- High-dose cod liver oil or fish liver oil supplements. Unlike ordinary fish-body oil, liver oils carry significant preformed vitamin A, and large doses can add up.
By contrast, two things are not red flags and should not cause alarm: a standard prenatal multivitamin (deliberately formulated with a modest, safe amount of vitamin A, often partly as beta-carotene), and beta-carotene from fruits and vegetables such as carrots, sweet potatoes, and spinach. As explained above, the body controls its conversion of beta-carotene, so dietary carotenoids do not pose the teratogenic risk that preformed retinol and retinoid drugs do. For the full comparison of the two forms, see Beta-Carotene vs. Preformed Vitamin A.
Where the Excess Comes From
It is worth separating the sources by how much risk they actually carry, because lumping them together causes needless worry about ordinary food and needless complacency about the truly dangerous drugs.
- Oral retinoid medications — the dominant danger. Isotretinoin is the most important. It is among the most reliably teratogenic medicines in common use: a large fraction of pregnancies exposed in the first trimester end in miscarriage or serious malformation. That extreme risk is the entire reason the drug is dispensed only through formal pregnancy-prevention programs (in the United States, the iPLEDGE program), which require pregnancy testing and two forms of contraception. Acitretin carries the added problem of a very long persistence in body fat. These drugs are effective and appropriate for the conditions they treat — the issue is strictly avoiding conception while they are in the body.
- High-dose preformed vitamin A (retinol) supplements. Stand-alone vitamin A pills, or “mega-dose” and some “eye health” or “immune” formulas, can contain far more retinol than is safe in pregnancy. This is the supplement-aisle hazard — not the prenatal vitamin, but the high-potency single-nutrient bottle.
- Liver and liver products. Because the liver is the body’s storage organ for vitamin A in every animal, eating it concentrates that store. A modest serving of liver can deliver several times the daily requirement of preformed vitamin A in one sitting; eaten often, it is the only normal food that can reach a worrisome intake. Beef liver and other organ meats are nutritional powerhouses outside of pregnancy — the caution here is specific to the first trimester.
- Cod liver oil and fish liver oils. Valued for omega-3s and vitamin D, these also carry preformed vitamin A; high doses can contribute meaningfully to total intake.
The unifying thread is preformed vitamin A in concentrated form. Ordinary mixed meals, a normal varied diet, and a standard prenatal supplement do not approach the concern; the risk lives in retinoid drugs, high-potency retinol pills, and the unusual case of frequent liver consumption.
Getting Checked & Knowing Your Numbers
An important and slightly counterintuitive truth about this topic is that there is no useful screening blood test for it in the way there is for, say, high potassium. A blood retinol level does not reliably reflect whether a damaging exposure occurred during the critical embryonic window, because the body buffers blood retinol tightly and the harm is about the dose reaching the embryo at a specific time, not a number on a routine lab. Management is therefore built around preventing exposure and, if an exposure has happened, assessing the pregnancy — not around catching a lab value.
In practice that means a few concrete things:
- Know the safe upper intake. The general tolerable upper intake level for preformed vitamin A in adults is about 3,000 micrograms RAE per day (roughly 10,000 IU), and in pregnancy the goal is to stay well under that from supplements and concentrated sources. The recommended intake during pregnancy is far lower than the upper limit — on the order of 770 micrograms RAE per day — which a normal diet and prenatal vitamin meet comfortably. Reading the form is essential: a unit listed as “retinol,” “retinyl palmitate,” or “retinyl acetate” is preformed vitamin A and counts toward the limit; “beta-carotene” does not carry the same teratogenic concern.
- Review medications and supplements before and early in pregnancy. The most valuable “test” is a careful look at the medicine cabinet and supplement shelf with a clinician or pharmacist, ideally before conception. Liver-function context can be checked with liver function tests in the broader setting of vitamin A excess, and a general Comprehensive Metabolic Panel is part of routine care — but neither is a teratogenicity test.
- If an exposure has already occurred, the pregnancy is assessed, not the blood. A clinician (often with a maternal-fetal medicine specialist) will consider the exact drug or dose and the timing, and detailed ultrasound, sometimes with fetal echocardiography, is used to evaluate the developing baby. A teratogen information service (such as MotherToBaby in the US) can give individualized counseling about a specific exposure.
Prevention and What to Do
Because the damage cannot be undone once it has occurred, almost everything that matters here is prevention — and the good news is that it is straightforward.
- If you take an oral retinoid, do not become pregnant while it is in your body. For isotretinoin this means reliable contraception throughout treatment and for at least a month after the last dose, as required by the pregnancy-prevention program; the drug clears the body relatively quickly once stopped, so pregnancy after the prescribed waiting period is not expected to carry the drug’s risk. Acitretin is different and far stricter — because it persists for many months to years, pregnancy must be avoided for a long period after stopping (commonly cited as up to three years), and alcohol is avoided because it converts acitretin to an even longer-lasting form. If you are on one of these drugs and are planning a pregnancy, talk with your prescriber before stopping contraception.
- Choose a standard prenatal vitamin, not a high-dose retinol pill. Prenatal vitamins are formulated to be safe; the thing to avoid is a separate high-potency vitamin A supplement. If a bottle lists vitamin A as retinol/retinyl esters in the thousands of IU, set it aside during pregnancy unless a clinician specifically directs otherwise.
- Limit liver and fish-liver oils during pregnancy. Enjoying liver occasionally is one thing; eating it weekly, or taking high-dose cod liver oil, can push preformed vitamin A intake into the concerning range. Many national health authorities advise pregnant women to avoid or strictly limit liver for exactly this reason. Beta-carotene-rich vegetables remain a safe and excellent way to get vitamin A activity.
- Plan ahead if pregnancy is possible. Because the vulnerable window is so early — often before a pregnancy is confirmed — anyone who could become pregnant and is taking a retinoid or a high-dose vitamin A supplement should sort this out in advance, not after a positive test.
- If an exposure has happened, do not panic — get counseling. Not every exposed pregnancy is affected, and the risk depends heavily on the specific agent, dose, and timing. A clinician or a teratogen information service can give a realistic, individualized assessment and arrange the appropriate ultrasound monitoring.
For the wider picture of what high vitamin A does to the body in general — the liver, the bones, the pressure inside the skull — see the Hypervitaminosis A hub and its companion pages on liver damage and bone and joint pain.
When to Seek Care / Red Flags
The “red flags” for this topic are not symptoms to wait for — they are situations that warrant a conversation with a clinician promptly, ideally before they become a problem:
- You are taking isotretinoin, acitretin, or another oral retinoid and there is any chance you could be pregnant — a missed period, unprotected sex, or contraception failure. This is urgent: contact your prescriber right away and arrange a pregnancy test.
- You are planning a pregnancy and currently take an oral retinoid or a high-dose vitamin A supplement. Speak with your clinician before stopping contraception, so the right waiting period and supplement adjustments can be planned.
- You took a high-dose preformed vitamin A supplement, or ate liver frequently, and have just learned you are pregnant. Bring the exact product and dose to your appointment so the intake can be assessed; in most ordinary cases the reassurance is genuine, but it should be evaluated rather than guessed at.
- You are pregnant and a routine ultrasound raises a question about the heart, face, or brain. This is rarely due to vitamin A, but it warrants specialist evaluation (maternal-fetal medicine) regardless of the cause.
The reassuring bottom line bears repeating: this is one of the few pregnancy risks that is almost entirely within your control. A normal diet and a standard prenatal vitamin are safe. The action items are simply to avoid high-dose preformed vitamin A, treat oral retinoids with the seriousness their pregnancy-prevention programs demand, and ask before, not after.
Key Research Papers
- Lammer EJ, Chen DT, Hoar RM, et al. (1985). Retinoic Acid Embryopathy. New England Journal of Medicine;313(14):837-841. — DOI: 10.1056/NEJM198510033131401
- Rothman KJ, Moore LL, Singer MR, et al. (1995). Teratogenicity of High Vitamin A Intake. New England Journal of Medicine;333(21):1369-1373. — DOI: 10.1056/NEJM199511233332101
- Collins MD, Mao GE (1999). Teratology of Retinoids. Annual Review of Pharmacology and Toxicology;39:399-430. — DOI: 10.1146/annurev.pharmtox.39.1.399
- Azaïs-Braesco V, Pascal G (2000). Vitamin A in pregnancy: requirements and safety limits. The American Journal of Clinical Nutrition;71(5):1325S-1333S. — DOI: 10.1093/ajcn/71.5.1325s
- Adams J (2010). The neurobehavioral teratology of retinoids: A 50-year history. Birth Defects Research Part A: Clinical and Molecular Teratology;88(10):895-905. — DOI: 10.1002/bdra.20721
- Bastos Maia S, Rolland Souza AS, Costa Caminha MF, et al. (2019). Vitamin A and Pregnancy: A Narrative Review. Nutrients;11(3):681. — DOI: 10.3390/nu11030681
- Pinheiro SP, Kang EM, Kim CY, et al. (2013). Concomitant use of isotretinoin and contraceptives before and after iPLEDGE in the United States. Pharmacoepidemiology and Drug Safety;22(12):1251-1257. — DOI: 10.1002/pds.3481
- Brinker A, Kornegay C, Nourjah P (2005). Trends in Adherence to a Revised Risk Management Program Designed to Decrease or Eliminate Isotretinoin-Exposed Pregnancies. Archives of Dermatology;141(5). — DOI: 10.1001/archderm.141.5.563
- National Institutes of Health, Office of Dietary Supplements. Vitamin A and Carotenoids — Health Professional Fact Sheet (intake, upper limits, and pregnancy safety). — NIH Office of Dietary Supplements
PubMed Topic Searches
- PubMed — Retinoic acid embryopathy and isotretinoin
- PubMed — Vitamin A teratogenicity and retinol intake in pregnancy
- PubMed — Retinoids, neural crest, and craniofacial development
- PubMed — Isotretinoin and the iPLEDGE pregnancy-prevention program
- PubMed — Acitretin persistence and teratogenicity
Connections
- Hypervitaminosis A Symptom Hub
- Vitamin A Toxicity and Liver Damage
- Vitamin A Toxicity and Bone & Joint Pain
- Vitamin A Toxicity and Headache & Brain Pressure
- Vitamin A Deficiency Hub
- Vitamin A Overview
- Beta-Carotene vs. Preformed Vitamin A
- Food Sources of Vitamin A
- Vitamin D3
- Vitamin E
- Beef Liver
- Cod Liver
- Sweet Potatoes
- Liver Function Tests
- Comprehensive Metabolic Panel