Choline Toxicity (High-Dose Choline): Low Blood Pressure and Sweating
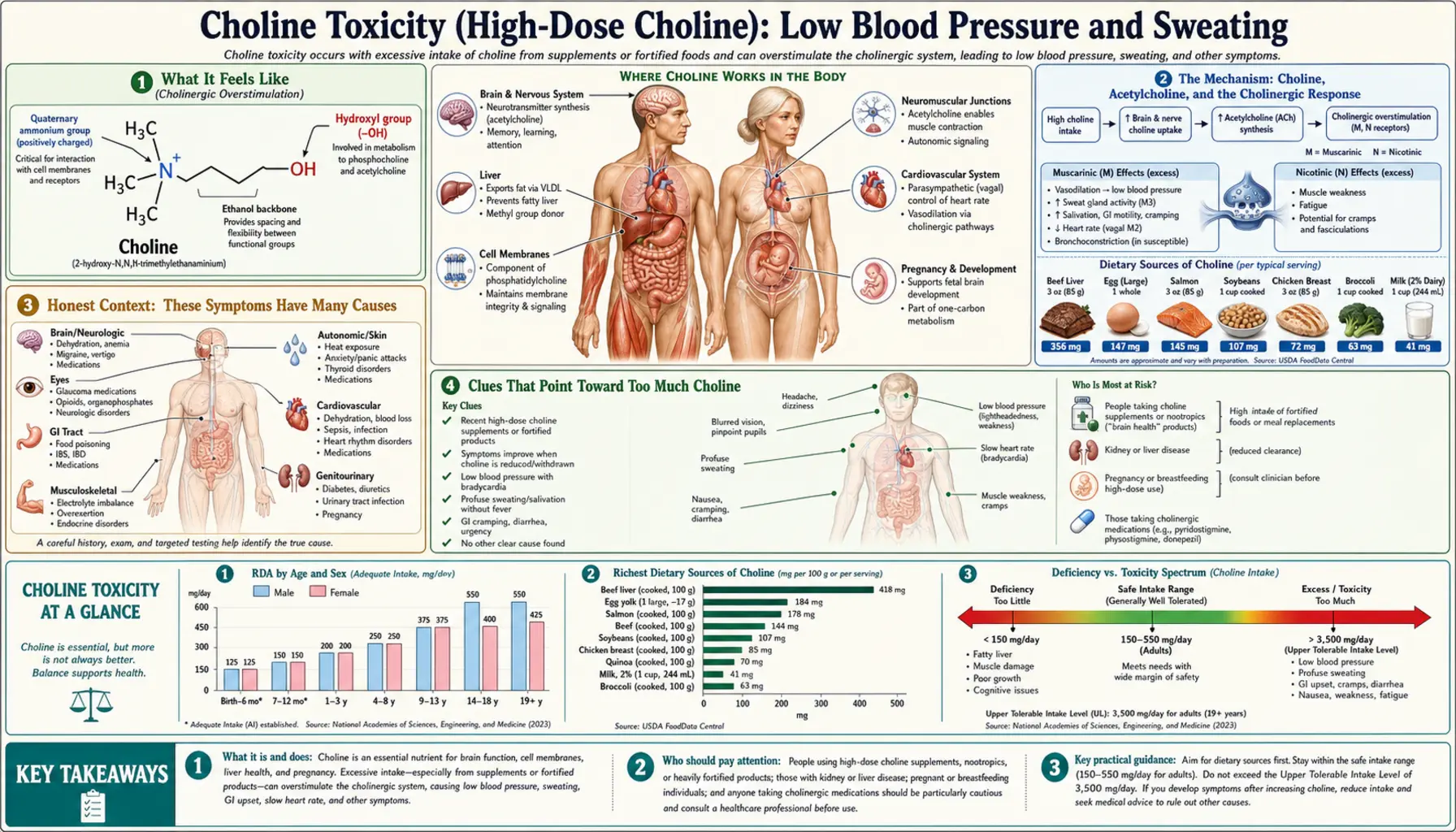
At very high supplement doses — gram for gram, well above the 3.5 grams a day set as the safe upper limit for adults — choline can occasionally produce a cluster of cholinergic effects: a drop in blood pressure that leaves you light-headed or faint (hypotension), a flush of sweating, and watery salivation. The biology behind this is real: choline is the raw material your body uses to build acetylcholine, the chemical messenger that, among many jobs, tells blood vessels to relax and sweat and saliva glands to switch on. But two honest points dominate this page. First, this is uncommon, it is tied to gram-level supplement doses rather than to choline from eggs, meat, or fish, and food simply cannot deliver enough to cause it. Second, low blood pressure and sweating have a long list of far more likely explanations — dehydration, medications, standing up too fast, anxiety, low blood sugar, infection — so these symptoms are almost never a sign of too much choline. This page explains how the symptom feels, the acetylcholine mechanism behind it, why it is so rarely the real cause, and when light-headedness or sweating means you should be checked.
Table of Contents
- What It Feels Like
- The Mechanism: Choline, Acetylcholine, and the Cholinergic Response
- Honest Context: These Symptoms Have Many Causes
- Clues That Point Toward Too Much Choline
- What Causes a Choline Excess Big Enough to Matter
- How Much Is Too Much? The 3.5-Gram Upper Limit
- Getting Checked
- What to Do: Stopping the Source and Managing Symptoms
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What It Feels Like
When a very large dose of supplemental choline does tip someone into cholinergic effects, the experience usually arrives as a small group of symptoms together rather than any single one in isolation — and that grouping is itself a clue, because the body's “rest-and-digest” nerve signaling tends to switch on across several organs at once. People describe some combination of the following:
- Light-headedness or feeling faint. This is the felt version of hypotension — blood pressure dipping low enough that, especially when you stand, not quite enough blood reaches the brain for a moment. It can feel like the room tilting, a graying of vision, a need to sit down, or simply “woozy.”
- Sweating. A clammy, cool sweat that comes on without exertion or heat — the palms, forehead, or whole body may feel damp. Because sweat glands are switched on by the same cholinergic signal, this often appears alongside the light-headedness rather than on its own.
- Increased salivation. A watery mouth, more saliva than usual, sometimes enough to notice or to make you swallow repeatedly. On its own it is trivial; as part of the cluster it fits the pattern.
- A “wired but unwell” feeling. Some people also report mild nausea, a slightly slowed or fluttery pulse, or a flushed, vaguely sick sensation. These overlap with the separate, far more common complaints covered on the digestive upset from high-dose choline page.
Two qualities matter for telling this apart from everyday faintness. First, it is dose-linked and timed: it follows a large supplement dose (often deliberately high-dose choline, lecithin, CDP-choline/citicoline, or alpha-GPC stacked together) by perhaps half an hour to a couple of hours, and it eases as the dose wears off. Second, the sweating-plus-salivation combination is unusual for ordinary causes of low blood pressure; a simple drop in pressure from dehydration or standing quickly does not usually make you drool. None of this is proof — but a tight time-link to a big choline dose, with several cholinergic signs at once, is what would make choline a plausible suspect rather than a coincidence.
The Mechanism: Choline, Acetylcholine, and the Cholinergic Response
To understand why too much choline could lower blood pressure and turn on sweat and saliva, it helps to know what choline is for. Choline is an essential nutrient with several jobs — it builds the phosphatidylcholine in every cell membrane, it ferries fat out of the liver, and it donates methyl groups to the body's chemistry. But one of its most important roles is as the direct raw material for acetylcholine, one of the body's master chemical messengers.
Acetylcholine is the neurotransmitter of the parasympathetic nervous system — the “rest-and-digest” branch that quietly runs the background housekeeping of the body. When acetylcholine is released and lands on muscarinic receptors on the surface of target tissues, it produces a recognizable set of effects: it widens blood vessels (which lowers blood pressure), slows the heart, and switches on the secreting glands — the sweat glands, the salivary glands, the tear glands, and the glands of the gut. This is why the classic teaching mnemonic for an over-active cholinergic state includes salivation, sweating, and a falling blood pressure. The pharmacology of these muscarinic receptors — and exactly which receptor subtype drives sweating, glandular secretion, and the vascular and cardiac slowing — has been mapped in detail in receptor and knockout-mouse studies.
An analogy. Think of acetylcholine as the body's “settle down and tend the house” signal. Normally it is released in measured pulses exactly where it is needed and then mopped up within milliseconds by an enzyme (acetylcholinesterase), so its effects are precise and brief. The cholinergic symptoms here are like the housekeeping signal being turned up a notch too far across the whole house at once — the vessels relax (pressure drops), the glands open (sweat and saliva flow), and the heart eases off. It is the same signal that runs the body every day, just dialed up.
Where does extra choline fit in? Choline supplies the precursor pool for acetylcholine, and providing more choline can, under some conditions, increase acetylcholine synthesis and release — this is precisely why choline precursors have been studied as treatments in conditions of low acetylcholine. So in principle, flooding the body with gram-level choline could nudge cholinergic signaling upward and produce, in a susceptible person, a mild version of the muscarinic picture: a touch of hypotension, sweating, and salivation. It is worth being candid about the limits of this story, though. The brain tightly regulates how much choline crosses into it and how much acetylcholine it makes, so the link between an oral dose and a body-wide cholinergic surge is neither simple nor guaranteed — which is part of why these symptoms are uncommon even among people taking large doses. The mechanism is biologically plausible and consistent with what acetylcholine does; it is not a reliable, dose-for-dose effect.
Honest Context: These Symptoms Have Many Causes
This is the most important section on the page. Low blood pressure and sweating are extremely common and almost never caused by choline. If you feel faint or break out in a cold sweat, the overwhelming odds are that something other than a vitamin is responsible. Before choline ever enters the conversation, the usual suspects deserve to be ruled out, because several of them are genuinely dangerous and several are trivially fixable:
- Dehydration and heat. Too little fluid — from hot weather, exercise, vomiting, diarrhea, or simply not drinking enough — lowers blood volume and pressure and drives sweating. This is probably the single most common explanation.
- Standing up too quickly (orthostatic hypotension). A brief head-rush on rising is ordinary; if it is frequent or causes fainting it can reflect dehydration, medications, or autonomic nerve problems.
- Medications. Many drugs lower blood pressure on purpose or as a side effect — blood-pressure medicines, diuretics (“water pills”), nitrates, alpha-blockers for the prostate, some antidepressants, and others. Sweating is also a known side effect of several antidepressants and other drugs.
- Low blood sugar (hypoglycemia). A falling glucose level classically causes sweating, shakiness, light-headedness, and a racing heart — especially in people who take insulin or certain diabetes pills.
- Infection and fever. An infection can cause both sweating and a drop in blood pressure; a sharply falling pressure with fever (sepsis) is an emergency.
- The heart and a slow pulse. A heart that is beating too slowly or pumping weakly can lower blood pressure and cause faintness and sweating. See arrhythmia and related cardiac causes.
- A simple faint (vasovagal syncope). Pain, fright, the sight of blood, prolonged standing, or straining can trigger a reflex that suddenly drops both the heart rate and blood pressure — classically with a wave of sweating and nausea just beforehand.
- Anxiety and panic. A surge of adrenaline produces sweating, light-headedness, and a pounding heart that can feel alarmingly physical.
- Hormonal and other causes. Thyroid problems, blood loss or anemia, the menopause transition (hot flushes with sweating), and adrenal insufficiency can all cause some mixture of these symptoms.
The take-home message is one of perspective: a vitamin is near the bottom of this list, not the top. Choline becomes a reasonable thing to consider only after the common causes have been thought through and there is a clear, timed link to a very large supplement dose. Treating choline as the explanation while ignoring dehydration, a new medication, low blood sugar, or a cardiac cause would be a mistake.
Clues That Point Toward Too Much Choline
Given how non-specific the symptoms are, what would actually raise suspicion that choline is involved? It comes down to a pattern, not any single feature:
- A clear dose-and-time link. Symptoms that reliably begin in the half-hour-to-two-hours after a large choline-containing dose, ease as it wears off, and return when the dose is repeated — that reproducibility is the strongest clue.
- An unusually high intake. Choline becomes plausible only at gram-level intake — deliberately high-dose choline bitartrate, large lecithin servings, or cognitive-enhancement stacks combining citicoline (CDP-choline) and alpha-GPC, sometimes several together. Ordinary food and standard multivitamins do not reach this territory.
- The cholinergic cluster, together. Light-headedness plus sweating plus a watery mouth, appearing as a set, fits cholinergic over-activity better than any one symptom alone. Sweating with salivation is a particularly suggestive pairing because ordinary low blood pressure does not usually make you drool.
- A companion fishy odor. At high choline intakes some people develop a fishy body odor as gut bacteria turn the excess into trimethylamine. If a fishy smell and the cholinergic symptoms appear together after big doses, choline overload moves higher up the list.
- Everything else checks out. When you are well hydrated, your medications are unchanged, your blood sugar is normal, and there is no fever or infection — and yet the symptoms still track with the supplement — choline becomes a more reasonable candidate.
Even with all of these present, the right move is not to self-diagnose but to stop the high-dose supplement and see whether the symptoms resolve, ideally with a clinician aware of the full picture. A symptom that disappears when the megadose stops and predictably returns when it restarts is far more convincing than any single feeling in the moment.
What Causes a Choline Excess Big Enough to Matter
It is worth being precise about where a problematic choline load could realistically come from, because it is not the diet. The body's total usual choline intake in the United States averages only a few hundred milligrams a day — well under half a gram — and most people fall short of the recommended adequate intake rather than over it. Whole foods rich in choline (eggs, liver and other organ meats, beef, poultry, fish, soybeans) deliver choline in the tens-to-low-hundreds of milligrams per serving. You would have to eat an implausible quantity of even the richest food to approach the gram-level intakes associated with symptoms; food is not a realistic route to choline toxicity.
The realistic routes are all supplemental:
- High-dose choline supplements. Choline bitartrate, choline chloride, and similar products are sold in doses that, if taken in quantity or stacked, can reach grams per day.
- Lecithin / phosphatidylcholine. Lecithin and phosphatidylcholine supplements were studied historically at large doses (for memory and liver indications), and the high-dose trials are where most reports of choline-related side effects — cholinergic symptoms, gut upset, and the fishy odor — originate.
- Cognitive-enhancement “nootropic” stacks. Citicoline (CDP-choline) and alpha-GPC are choline-delivering compounds popular for memory and focus. People sometimes combine several choline sources at once without tallying the total, which is how an unintentionally large daily load can build up.
- Older clinical and parenteral exposures. Very high choline or lecithin doses have also been used in research and in some intravenous nutrition settings, again at intakes far above anything achievable from eating.
The unifying thread is simple: an intake large enough to matter is essentially always self-administered as a supplement, often by someone deliberately seeking the highest dose they can. The practical implication for the cause is equally simple — the lever you can pull is the supplement bottle, not your plate.
How Much Is Too Much? The 3.5-Gram Upper Limit
There is a published safety ceiling for choline, and it is the single most useful number on this page. In 1998 the U.S. Institute of Medicine set a Tolerable Upper Intake Level (UL) of 3.5 grams (3,500 mg) of choline per day for adults — the highest daily intake judged unlikely to cause harm in the general population. The European Food Safety Authority later reviewed the same question and, while it considered the data insufficient to set a numeric upper limit of its own, it likewise framed adverse effects as a concern only at intakes far above normal dietary levels.
Crucially, the symptom that defined the choline UL was low blood pressure (hypotension) — together with a fishy body odor and sweating — observed at high supplemental doses. In other words, the very symptom this page describes is the one the safety committee used as its marker of “too much.” The UL was then set with a safety margin below the doses where those effects appeared, so most reported hypotension occurred at intakes above 3.5 grams a day — many times higher than anyone gets from food, and above what most supplement labels suggest as a single dose.
For perspective, the adequate intake targets are far lower: about 550 mg/day for men and 425 mg/day for women (more in pregnancy and lactation). So the upper limit sits roughly six to eight times above the amount you are actually trying to get. The gap between “enough” and “too much” is wide, which is reassuring — reaching the danger zone takes deliberate, gram-level supplementation, not a good diet and not a normal supplement habit.
Getting Checked
There is no routine blood test for “choline toxicity,” and you would not order one to explain light-headedness and sweating. The evaluation is the standard, sensible work-up for those symptoms, with the supplement history folded in:
- A careful history — including the supplement shelf. The most valuable step is also the simplest: telling the clinician exactly what you take, in what doses, and how the symptoms relate in time to those doses. Many people forget to mention lecithin, citicoline, or alpha-GPC because they think of them as harmless — but the timing is the whole diagnosis here.
- Blood pressure, lying and standing. Measuring blood pressure after lying down and again after standing (orthostatic vital signs) confirms whether pressure is genuinely dropping and by how much — the objective counterpart to feeling faint.
- Basic bloodwork to find the common causes. A blood-sugar check (for hypoglycemia), a Comprehensive Metabolic Panel (hydration, kidney function, electrolytes), a count for anemia, and thyroid tests are aimed squarely at the far more likely explanations described above.
- A look at the heart when warranted. If the pulse is slow or irregular or fainting has occurred, an electrocardiogram (ECG) checks the heart's rhythm and rate — see arrhythmia.
- The decisive test: stop and watch. Because there is no specific lab marker, the real confirmation is a careful trial of stopping the high-dose supplement and seeing whether the symptoms resolve — and, only if appropriate and supervised, whether they recur on resuming. A clear stop-it-improves, restart-it-returns pattern is far stronger evidence than any single measurement.
The point of the work-up is not to prove choline guilty but to make sure a dangerous or easily treatable cause is not being missed while a supplement is blamed. Diagnosis here is mostly about good history-taking and ruling things out, not a fancy test.
What to Do: Stopping the Source and Managing Symptoms
If high-dose choline really is the culprit, the treatment is refreshingly straightforward, because choline is water-soluble and the body clears an excess on its own once you stop feeding it in:
- Stop or sharply cut the supplement. The single most effective step is to discontinue the high-dose choline, lecithin, citicoline, or alpha-GPC — or at minimum drop to a much lower dose. Because choline is cleared by the body, the cholinergic symptoms typically settle within hours to a day or so after the excess intake stops.
- Tally your total intake. If you take several products, add up how much choline they deliver together. The fix is often simply recognizing that two or three “reasonable” doses were stacking into a gram-level total.
- Support yourself through a low-pressure episode. If you feel faint, sit or lie down and raise your legs until it passes; rise slowly afterward; and rehydrate with fluids (and a little salt, if appropriate for you) to restore blood volume. Cool down and change out of damp clothing if sweating has soaked you.
- Reintroduce cautiously, if at all. If there is a genuine reason to take choline, restart at the lowest effective dose — ideally guided by the adequate-intake targets (around 425–550 mg/day) rather than the gram-level doses marketed for cognition — and stay well under the 3.5 g/day upper limit.
- Address the real cause if it turns out not to be choline. If stopping the supplement does not resolve the symptoms, the cause lies elsewhere — revisit medications, hydration, blood sugar, the heart, and the other explanations above with a clinician.
There is no antidote and none is needed for the mild cholinergic effects of oral choline; removing the source and letting the body clear it is the treatment. (A true cholinergic crisis — from nerve-agent or organophosphate-pesticide poisoning, not from a vitamin — is a different, life-threatening emergency treated with atropine and other measures; that is not what high-dose dietary choline causes.)
When to Seek Care / Red Flags
Because low blood pressure and sweating can also signal something serious, the symptoms themselves — not their presumed cause — should drive how urgently you act. Seek emergency care for any of the following, whether or not you take choline:
- Fainting or near-fainting — actually losing consciousness, or feeling you are about to, particularly with chest pain, breathlessness, or an irregular heartbeat.
- Cold, clammy sweating with a racing or very slow pulse, confusion, or a feeling of impending doom — this combination can accompany a heart problem, a dangerous infection, or a severe allergic reaction.
- Sweating and faintness in someone with diabetes — treat for possible low blood sugar (fast-acting carbohydrate) and seek help if it does not resolve quickly.
- Blood pressure that stays low with fever, severe abdominal pain, vomiting, or signs of bleeding — a falling pressure in these settings can indicate sepsis or blood loss and needs urgent assessment.
- Drenching night sweats, unexplained weight loss, or sweating with palpitations and tremor — patterns that warrant evaluation for thyroid, hormonal, or other systemic causes.
For the milder, dose-linked cholinergic symptoms specifically — light-headedness, sweating, and salivation that clearly follow a large choline supplement — the right step is non-urgent but real: stop the high-dose product and discuss it with a clinician or pharmacist, bringing every supplement bottle with you. The reassuring truth is that the choline-related version of these symptoms is mild and reversible; the reason to take the symptoms seriously at all is that the other causes on this page are not always mild, and a vitamin should never be blamed before they are considered.
Key Research Papers
- Institute of Medicine, Food and Nutrition Board (1998). Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline (Choline chapter; sets the 3.5 g/day UL). National Academies Press, Washington, DC. — DOI: 10.17226/6015
- EFSA Panel on Dietetic Products, Nutrition and Allergies (2016). Dietary Reference Values for choline. EFSA Journal;14(8):4484. — DOI: 10.2903/j.efsa.2016.4484
- Zeisel SH, da Costa KA (2009). Choline: an essential nutrient for public health. Nutrition Reviews;67(11):615-623. — DOI: 10.1111/j.1753-4887.2009.00246.x
- Zeisel SH, da Costa KA (2006). Choline: Critical Role During Fetal Development and Dietary Requirements in Adults. Annual Review of Nutrition;26:229-250. — DOI: 10.1146/annurev.nutr.26.061505.111156
- Zeisel SH (1994). Choline and Human Nutrition. Annual Review of Nutrition;14:269-296. — DOI: 10.1146/annurev.nu.14.070194.001413
- Wess J, Eglen RM, Gautam D (2007). Muscarinic acetylcholine receptors: mutant mice provide new insights for drug development. Nature Reviews Drug Discovery;6(9):721-733. — DOI: 10.1038/nrd2379
- Wess J (2004). Muscarinic Acetylcholine Receptor Knockout Mice: Novel Phenotypes and Clinical Implications. Annual Review of Pharmacology and Toxicology;44:423-450. — DOI: 10.1146/annurev.pharmtox.44.101802.121622
- Mehedint MG, Zeisel SH (2013). Choline's role in maintaining liver function: new evidence for epigenetic mechanisms. Current Opinion in Clinical Nutrition and Metabolic Care;16(3):339-345. — DOI: 10.1097/MCO.0b013e3283600d46
- Wallace TC, Fulgoni VL (2016). Assessment of Total Choline Intakes in the United States. Journal of the American College of Nutrition;35(2):108-112. — DOI: 10.1080/07315724.2015.1080127
- Wiedeman AM, Barr SI, Green TJ, et al. (2018). Dietary Choline Intake: Current State of Knowledge Across the Life Cycle. Nutrients;10(10):1513. — DOI: 10.3390/nu10101513
- Lemos BS, Medina-Vera I, Blesso CN, Fernandez ML (2018). Effects of Egg Consumption and Choline Supplementation on Plasma Choline and Trimethylamine-N-Oxide in a Young Population. Journal of the American College of Nutrition;37(8):716-723. — DOI: 10.1080/07315724.2018.1466213
- Mackay DS, et al. Trimethylaminuria and the metabolism of dietary choline to trimethylamine (fishy odor at high choline intakes). PubMed literature search. — PubMed
PubMed Topic Searches
- PubMed — Choline supplementation, hypotension, and adverse effects
- PubMed — Choline tolerable upper intake level and safety
- PubMed — Muscarinic effects: sweating, salivation, vasodilation
- PubMed — High-dose lecithin / phosphatidylcholine cholinergic side effects
- PubMed — Citicoline / alpha-GPC choline precursor tolerability
Connections
- All Vitamins
- Choline Toxicity Hub
- Choline Toxicity and Fishy Body Odor
- Choline Toxicity and Digestive Upset
- Choline Deficiency Hub
- Choline Overview
- Choline, Cognition & Acetylcholine
- Choline, Cardiovascular Health & TMAO
- Lecithin
- Phosphatidylcholine
- Food Sources of Choline
- Eggs
- Arrhythmia
- Comprehensive Metabolic Panel