Dioxins: Persistent Organic Pollutants and Human Health
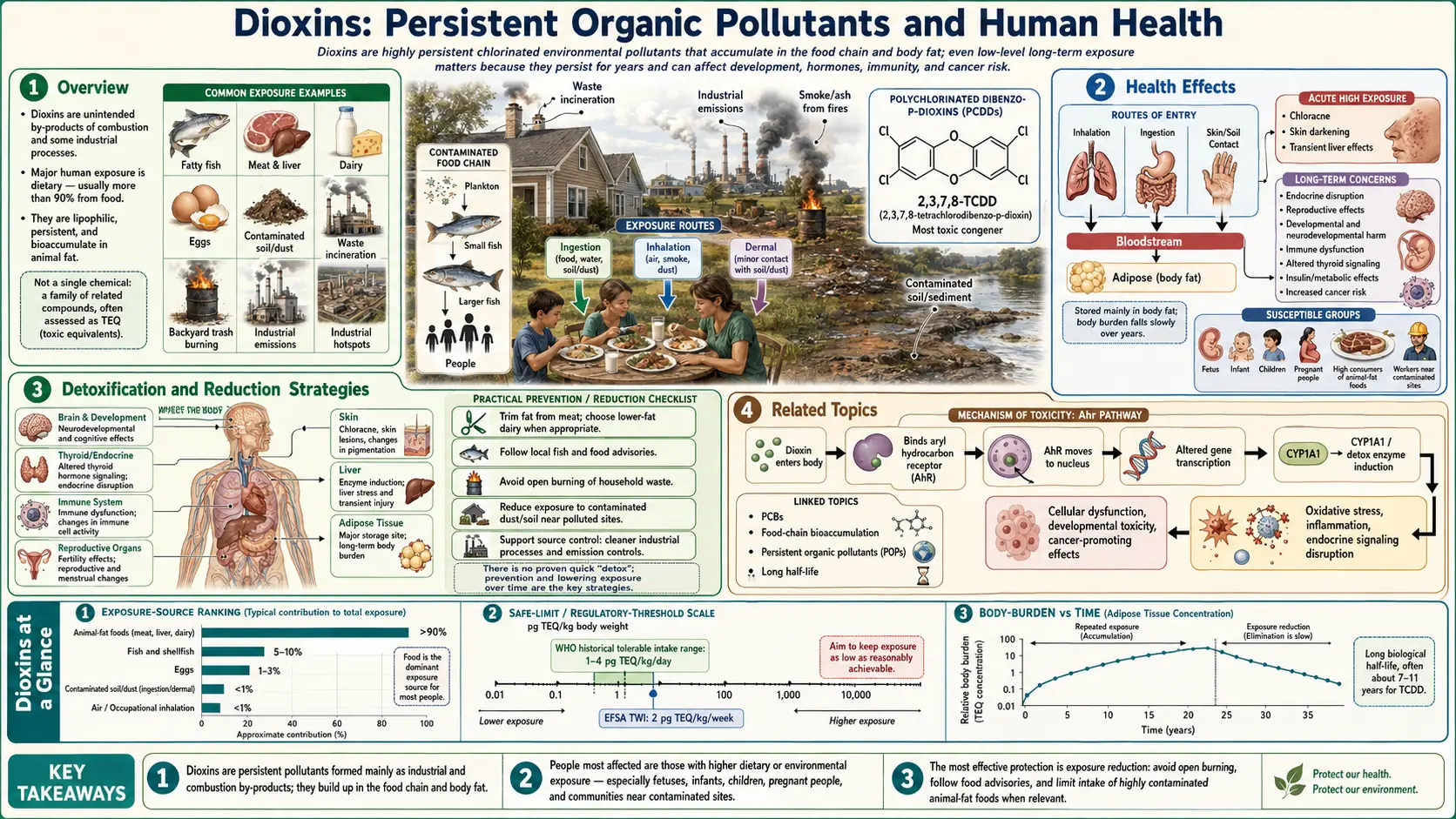


Table of Contents
- Overview
- Sources of Exposure
- Mechanism of Toxicity
- Health Effects
- Dioxins in the Food Supply
- Body Burden and Half-Life
- Detoxification and Reduction Strategies
- Regulatory Standards
- Recent Research and Advances
- Related Topics
- References
- Connections
- Featured Videos
1. Overview
Dioxins are a family of chemically related compounds that are persistent environmental pollutants (POPs). The term “dioxins” is commonly used to refer to two closely related groups: polychlorinated dibenzo-p-dioxins (PCDDs) and polychlorinated dibenzofurans (PCDFs). Together, these two families encompass 210 distinct congeners (structural variants), of which 17 are considered toxicologically significant due to their substitution pattern at the 2, 3, 7, and 8 positions.
The most studied and acutely toxic member is 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD), often called “the most toxic synthetic chemical known.” TCDD serves as the reference compound for the toxic equivalency factor (TEF) system, with a TEF value of 1.0 by definition. All other dioxin and furan congeners are assigned TEF values below 1.0 relative to TCDD, allowing mixed exposures to be expressed as a single toxic equivalency quotient (TEQ).
Dioxins are characterized by their extreme chemical stability, lipophilicity (fat solubility), and resistance to biological degradation. These properties allow them to persist in the environment for decades and accumulate through food chains — a process known as bioaccumulation and biomagnification. Dioxins are not deliberately manufactured for any commercial purpose; rather, they are unwanted byproducts of industrial thermal and chemical processes.
International recognition of dioxins as a global health threat culminated in the Stockholm Convention on Persistent Organic Pollutants, adopted in 2001 and entered into force in 2004. The Convention calls on signatory nations to reduce or eliminate releases of dioxins and other POPs from intentional and unintentional sources. As of 2025, over 180 countries have ratified the Stockholm Convention, making it one of the most widely adopted environmental treaties in history.
2. Sources of Exposure
Industrial and Combustion Sources
Dioxins are formed as unintentional byproducts whenever organic material containing carbon and chlorine is burned or processed at insufficient temperatures. The primary industrial sources include:
- Municipal and industrial waste incineration: Historically the single largest source of dioxin emissions in developed nations. Modern incinerators equipped with high-temperature afterburners (>850°C), rapid cooling systems, and activated carbon injection have reduced emissions by over 90% since the early 1990s.
- Medical waste incineration: Polyvinyl chloride (PVC) plastics in medical devices, when incinerated at low temperatures, are a significant source of PCDDs and PCDFs.
- Chlorine bleaching of wood pulp: The kraft pulp and paper industry, when using elemental chlorine for bleaching, generates dioxin-contaminated effluent. Substitution with chlorine dioxide or totally chlorine-free (TCF) processes has greatly reduced this source.
- Herbicide and pesticide manufacturing: Chlorophenol-based herbicide synthesis, particularly 2,4,5-trichlorophenoxyacetic acid (2,4,5-T) and its derivatives, generates TCDD as a synthetic impurity. The herbicide mixture known as Agent Orange (equal parts 2,4-D and 2,4,5-T) was contaminated with TCDD during manufacturing at levels ranging from 0.05 to 47 parts per million (ppm).
- Metal smelting and reclamation: Secondary copper and aluminum smelting, sintering of iron ore, and scrap metal recycling involving chlorinated materials are notable industrial sources.
- Cement kilns: When burning chlorine-containing waste fuels, cement kilns generate dioxins, though modern kiln designs minimize emissions.
- Open burning: Backyard burning of household waste, agricultural residue burning, and wildfires involving chlorine-containing vegetation or debris continue to be significant sources globally, particularly in developing countries.
Agent Orange and Military History
Between 1962 and 1971, the United States military sprayed approximately 77 million liters of herbicides over Vietnam, Cambodia, and Laos as part of Operation Ranch Hand. Agent Orange, which contained TCDD contamination estimated at 1–50 mg/kg, was the most heavily used formulation. The total TCDD released during the Vietnam War has been estimated at approximately 170 kg, contaminating over 3.1 million hectares of forest and agricultural land.
Veterans exposed to Agent Orange have demonstrated elevated rates of soft tissue sarcoma, non-Hodgkin lymphoma, Hodgkin disease, chloracne, type 2 diabetes, ischemic heart disease, Parkinson disease, peripheral neuropathy, and several other conditions now recognized by the U.S. Department of Veterans Affairs as “presumptive diseases” linked to Agent Orange exposure. Vietnamese populations living in former spray zones continue to exhibit elevated rates of birth defects and cancers attributed to residual dioxin contamination of local food supplies.
Food Chain as Primary Human Exposure Route
Despite dramatic reductions in industrial dioxin emissions over the past three decades, dietary intake remains the overwhelmingly dominant route of human exposure, accounting for more than 90% of total dioxin body burden in the general population. The remaining exposure comes from inhalation and dermal contact with contaminated soils, particularly near industrial sites.
Foods of animal origin — including meat, poultry, dairy products, fish, and eggs — contribute the vast majority of dietary dioxin intake because these animals concentrate dioxins acquired through their own feed and environmental exposures. High-fat dairy products and fatty fish are consistently identified as the highest-contributing food categories in dietary exposure assessments conducted in Europe and North America.
3. Mechanism of Toxicity
Aryl Hydrocarbon Receptor (AhR) Binding
The molecular mechanism of dioxin toxicity centers on binding to the aryl hydrocarbon receptor (AhR), a ligand-activated transcription factor present in virtually all vertebrate tissues. Under normal (unliganded) conditions, AhR resides in the cytoplasm as part of a multiprotein complex including two heat shock protein 90 (HSP90) chaperones, the co-chaperone p23, and the immunophilin-like protein XAP2.
When TCDD or another dioxin congener diffuses into the cell (facilitated by its high lipophilicity), it binds to the ligand-binding domain of AhR with extraordinarily high affinity — TCDD has a dissociation constant (Kd) in the range of 0.1–1.0 nM for rodent AhR. Ligand binding triggers a conformational change, dissociation of the chaperone complex, and translocation of the activated AhR into the nucleus.
In the nucleus, AhR dimerizes with the AhR nuclear translocator (ARNT), also called HIF-1β. The AhR/ARNT heterodimer binds to specific DNA sequences called dioxin response elements (DREs) or xenobiotic response elements (XREs), with the core consensus sequence 5′-GCGTG-3′. This binding activates transcription of a battery of genes encoding drug-metabolizing enzymes and regulatory proteins.
Gene Transcription Disruption
AhR-driven transcriptional activation alters the expression of dozens to hundreds of genes, with consequences at multiple levels of biology:
- CYP1A1 and CYP1B1 induction: The cytochrome P450 enzymes CYP1A1 and CYP1B1 are among the most strongly induced by dioxin AhR activation — increases of 10-fold to over 100-fold have been observed in exposed tissues. These enzymes metabolize polycyclic aromatic hydrocarbons (PAHs) and estrogens, and their induction can generate reactive metabolites capable of forming DNA adducts. CYP1A2 induction in the liver alters caffeine and drug metabolism, forming the basis of the widely used CYP1A2 phenotyping breath test.
- Endocrine pathway cross-talk: The AhR/ARNT dimer interacts functionally with the estrogen receptor (ER) signaling pathway through multiple mechanisms, including competitive binding to ARNT and AhR-mediated induction of CYP1B1 which catabolizes estradiol. This cross-talk underlies the anti-estrogenic and developmental toxicity of dioxins.
- Cell cycle and apoptosis disruption: AhR activation modulates expression of cell-cycle regulatory genes including cyclin D1 and p21(WAF1/CIP1), and interacts with the retinoblastoma protein (Rb) pathway, contributing to tumor-promoting effects.
- Immune gene regulation: Dioxin exposure suppresses antibody responses partly by AhR-mediated downregulation of B-cell differentiation factors and upregulation of immunosuppressive cytokines.
The Toxic Equivalency Factor (TEF) and TEQ System
Because environmental and food samples invariably contain complex mixtures of PCDD, PCDF, and co-planar PCB congeners rather than individual compounds, the World Health Organization established a Toxic Equivalency Factor (TEF) system to facilitate risk assessment. Each relevant congener is assigned a TEF relative to TCDD (TEF = 1.0). The Toxic Equivalency Quotient (TEQ) for a mixture is calculated as:
TEQ = Σ (concentration of congeneri × TEFi)
Selected WHO-TEF values (2005 revision) include: TCDD = 1.0; 1,2,3,7,8-PeCDD = 1.0; 1,2,3,4,7,8-HxCDD = 0.1; 2,3,4,7,8-PeCDF = 0.3; 2,3,7,8-TCDF = 0.1. The most recent WHO TEF reassessment was conducted in 2005 and remains the international standard. TEQ values allow regulators to set a single tolerable intake limit applicable to mixed real-world exposures.
4. Health Effects
Cancer — IARC Group 1 Carcinogen
The International Agency for Research on Cancer (IARC) classified TCDD as a Group 1 human carcinogen in 1997, based on sufficient evidence of carcinogenicity in humans and laboratory animals. The epidemiological evidence includes cohort studies of occupationally exposed workers (chemical plant workers, herbicide sprayers, Vietnam veterans) and populations exposed via industrial accidents (Seveso, Italy 1976). The strongest associations have been observed for:
- All cancers combined (modest but consistent elevation in heavily exposed cohorts)
- Soft tissue sarcoma
- Non-Hodgkin lymphoma
- Chronic lymphocytic leukemia
- Lung cancer (in some occupational cohorts)
TCDD acts primarily as a tumor promoter rather than an initiator (it does not directly damage DNA), operating through the AhR-mediated mechanisms described above. The broader category of “dioxin-like compounds” (DLCs), including certain PCBs, was classified as IARC Group 1 in 2015.
Endocrine Disruption
Dioxins are well-established endocrine-disrupting chemicals (EDCs). They interfere with the synthesis, secretion, transport, metabolism, and action of natural hormones — most extensively characterized for estrogens and thyroid hormones. Effects documented in epidemiological studies and experimental models include:
- Altered sex hormone ratios (decreased testosterone in males, anti-estrogenic effects)
- Reduced semen quality and testicular volume
- Altered timing of puberty
- Thyroid hormone disruption (decreased T4, altered TSH regulation)
- Disrupted glucose metabolism and insulin signaling, associated with increased risk of type 2 diabetes
Chloracne
Chloracne is the hallmark dermatological manifestation of acute high-dose dioxin exposure. It is characterized by cyst and comedo formation primarily on the face (especially the malar region and behind the ears), neck, and trunk. Unlike ordinary acne, chloracne lesions are predominantly cysts (milia-like) and comedones (blackheads) rather than pustules, and they may persist for years to decades. Chloracne is caused by AhR-mediated disruption of sebaceous gland differentiation and function. It has been documented in chemical plant workers, accident victims, and most famously in Viktor Yushchenko, the Ukrainian president poisoned with TCDD in 2004 (blood TCDD level: 108,000 pg/g lipid weight, approximately 50,000 times background).
Immunosuppression
Dioxins suppress multiple branches of the immune system. Animal models demonstrate dose-dependent thymic atrophy (involution of the thymus with loss of immature T-cell precursors), reduced antibody responses, suppressed natural killer (NK) cell activity, and impaired macrophage function. Human epidemiological data show associations between dioxin body burden and increased susceptibility to infections and elevated inflammatory markers. Children in the Seveso cohort showed impaired diphtheria antibody responses years after the 1976 accident.
Reproductive and Developmental Effects — Seveso Disaster Data
The explosion at the ICMESA chemical plant in Seveso, Italy on July 10, 1976 released an estimated 1–6 kg of TCDD into a densely populated area, affecting approximately 37,000 residents. This disaster has provided the most detailed epidemiological dataset on dioxin developmental effects in humans.
Key findings from the Seveso Women's Health Study and related investigations include:
- Sex ratio alteration: In the most heavily contaminated Zone A, a statistically significant reduction in the male-to-female birth ratio was observed for children born to fathers (not mothers) who had elevated serum TCDD at the time of conception. This finding has been replicated in other dioxin-exposed cohorts and is attributed to AhR-mediated impairment of Y-bearing sperm viability.
- Endometriosis: Women in higher-exposure zones demonstrated dose-dependent increases in endometriosis prevalence, consistent with dioxin's anti-estrogenic and pro-inflammatory actions on endometrial tissue.
- Breast cancer: A follow-up study published in 2008 found a statistically significant dose-response relationship between serum TCDD levels measured after the accident and subsequent breast cancer incidence, with relative risks up to 2.1 in the highest quintile of exposure.
- Neurodevelopment: Children born to women with elevated dioxin body burden showed subtle but measurable deficits in thyroid-dependent cognitive development, analogous to effects of other thyroid-disrupting agents.
Cardiovascular Effects
Epidemiological studies of dioxin-exposed workers and the general population have demonstrated associations between higher dioxin body burden and increased risk of ischemic heart disease and cardiovascular mortality. Mechanistic pathways include AhR-mediated induction of inflammatory mediators (IL-6, TNF-α), disruption of lipid metabolism, endothelial dysfunction, and altered coagulation factor expression. The U.S. Department of Veterans Affairs recognizes ischemic heart disease as a presumptive condition associated with Agent Orange exposure in Vietnam veterans.
5. Dioxins in the Food Supply
Bioaccumulation and Biomagnification
Due to their extreme lipophilicity (log Kow values of 6.8–8.2 for different dioxin congeners) and resistance to metabolic degradation, PCDDs and PCDFs partition preferentially into fatty tissues and resist elimination. This leads to bioaccumulation — concentration within an individual organism — and biomagnification — progressive concentration increase at each trophic level of a food chain.
In aquatic food chains, biomagnification factors from water to top predator fish can exceed 100,000-fold. In terrestrial food chains, dioxins deposited on pasture grasses are consumed by grazing animals, where they accumulate in milk fat and adipose tissue. The result is that humans, as apex consumers, receive the most concentrated dioxin exposure through food of animal origin.
Highest-Risk Foods
Dietary exposure assessments consistently rank the following food categories as the primary contributors to human dioxin TEQ intake:
- Fatty ocean fish (wild-caught salmon, mackerel, herring, sardines, eel) — particularly from the Baltic Sea, North Sea, and historically contaminated coastal zones
- Butter and high-fat dairy products — cream, full-fat cheese, whole milk
- Beef and lamb fat — especially from animals on contaminated pastures
- Eggs — free-range hens foraging in contaminated soil can accumulate substantially higher dioxin levels than caged hens on controlled feed
- Poultry fat
- Pork fat (lard)
Plant foods generally contain negligible dioxin levels, and non-fatty fish (lean white fish) carry much lower burdens than fatty species. The WHO estimated tolerable monthly intake (TMI) for dioxins and dioxin-like PCBs combined is 70 pg TEQ/kg body weight per month (equivalent to 2.3 pg TEQ/kg/day), a level that a significant proportion of populations in industrialized countries historically exceeded before major emission reductions in the 1990s–2000s.
Geographic Hotspots
Dioxin concentrations in food vary significantly by geography, reflecting proximity to industrial sources, soil contamination history, and local emission controls. Areas of elevated concern include:
- Baltic Sea region — legacy contamination from pulp mills and industrial zones has resulted in elevated dioxin levels in Baltic herring, salmon, and eel, prompting the EU to grant temporary exemptions to Nordic countries allowing the sale of fish exceeding EU maximum levels for domestic consumption
- Vietnam — former Agent Orange spray zones, particularly hotspots at former U.S. air bases (Bien Hoa, Da Nang, Phu Cat), with TCDD concentrations in soil exceeding 1,000 ppt in some samples
- Midwestern United States — areas around former pesticide manufacturing facilities and the Times Beach, Missouri contamination site
- Industrial river deltas — Hudson River (PCBs and dioxins from GE manufacturing), Passaic River (dioxins from Agent Orange precursor manufacturing at Diamond Alkali facility in Newark, NJ)
Major Contamination Incidents
Belgian Dioxin Crisis (1999): In January 1999, a batch of animal feed fat used in Belgian poultry and pig feed was accidentally contaminated with approximately 50 kg of PCB-containing transformer oil (Pyranol), which itself contained dioxin impurities. The resulting contaminated feed distributed to thousands of farms caused dioxin concentrations in Belgian poultry and eggs to reach levels 1,000–1,500 times above EU regulatory limits. The crisis went undetected for approximately 4 months (January to May 1999), during which contaminated products entered the food supply across Europe. When detected, the Belgian government ordered the destruction of approximately 7 million chickens and 60,000 pigs. The economic cost exceeded 1.5 billion euros, and the political fallout contributed to the fall of the Belgian government in the June 1999 elections. The crisis directly led to the establishment of the European Food Safety Authority (EFSA) and major reforms in EU food safety regulation.
Times Beach, Missouri (1971–1983): Waste oil sludge contaminated with TCDD from the synthesis of 2,4,5-T (a component of Agent Orange) at the Northeastern Pharmaceutical and Chemical Company (NEPACCO) plant was mixed with waste oil and sprayed on dirt roads throughout Missouri for dust suppression. The city of Times Beach was discovered in 1982 to have soil TCDD concentrations up to 300 ppb — 300 times the level EPA considered dangerous for residential exposure. The EPA recommended evacuation of Times Beach in January 1983; the federal government purchased the town for $33 million and relocated all 2,240 residents. Times Beach was subsequently demolished and the site remediated using high-temperature incineration.
Agent Orange in Vietnam: As described above, an estimated 170 kg of TCDD was deposited across 3.1 million hectares of Vietnam between 1962 and 1971. Residual TCDD contamination at former U.S. air bases remains a significant public health concern. Studies of residents near the Da Nang air base found mean serum TCDD levels of 3.5 pg/g lipid in adults — approximately 3–4 times the typical background level in developed nations — and substantially higher levels in individuals who consumed ducks and fish from base area drainage ponds.
6. Body Burden and Half-Life
TCDD Half-Life and Tissue Distribution
The biological half-life of TCDD in humans is exceptionally long, estimated at 7 to 11 years in most individuals, though estimates from heavily exposed individuals (Seveso accident victims, Viktor Yushchenko) suggest half-lives at the higher end of this range. This prolonged half-life reflects the compound's extreme resistance to hepatic metabolism at background exposure levels, its tight sequestration in adipose tissue, and the slow rate of adipose tissue turnover.
TCDD and other dioxins distribute primarily to adipose tissue (approximately 90% of body burden), with lower concentrations in liver, skin, and other lipid-containing compartments. Concentrations are typically expressed as picograms per gram of lipid weight (pg/g lipid) to normalize for individual differences in body fat percentage.
Background TCDD concentrations in the general population of industrialized nations, measured in blood or adipose tissue, have declined markedly since peak industrial emissions in the 1970s–1980s. Current background levels in adults in developed countries are typically in the range of 1–5 pg TCDD/g lipid, compared to levels of 20–50 pg/g lipid or higher in adults measured in the 1980s in the same populations.
Other Congeners and TEQ Body Burden
While TCDD is the most toxic individual congener, the total TEQ body burden includes contributions from multiple PCDD, PCDF, and dioxin-like PCB congeners. In the general population, 1,2,3,7,8-PeCDD, 1,2,3,4,7,8-HxCDD, 1,2,3,6,7,8-HxCDD, and the more chlorinated heptachloro- and octachlorodibenzo-p-dioxins contribute substantially to total body burden by mass, though their lower TEF values mean TCDD often still dominates TEQ calculations. Including dioxin-like PCBs (particularly PCB-126 with TEF = 0.1 and PCB-169 with TEF = 0.03), total TEQ body burdens in the general population range from approximately 10 to 50 pg WHO-TEQ/g lipid.
Breast Milk Transfer
Because dioxins are stored in adipose tissue and breast milk is an emulsion rich in maternal fat, breast milk is the primary route of dioxin transfer from mother to infant. Nursing infants receive dioxin doses per kilogram body weight estimated to be 30–60 times higher than the typical adult dietary intake on a per-body-weight basis. An exclusively breastfed infant receiving 750 mL/day of breast milk with a typical dioxin TEQ concentration of 15–25 pg/g fat may ingest 50–100 pg TEQ/day, far exceeding the WHO tolerable daily intake of 2.3 pg TEQ/kg/day when expressed relative to infant body weight.
Despite this quantitative exceedance, public health agencies worldwide consistently recommend continued breastfeeding for most infants, citing the well-established nutritional, immunological, and developmental benefits of breast milk. The recommendation reflects the fact that dioxin body burden in infants is declining over time as maternal and environmental levels fall, and that the benefits of breastfeeding substantially outweigh the dioxin-related risks for the general population. However, the situation underscores the importance of reducing maternal dioxin body burden before and during pregnancy.
Biomonitoring Data
National biomonitoring programs, including the U.S. National Health and Nutrition Examination Survey (NHANES) and the German Human Biomonitoring Commission programs, have documented the declining trend in blood dioxin levels in the general population. NHANES data show that mean serum TCDD concentrations in U.S. adults declined from approximately 7.4 pg/g lipid in 1987 to less than 2.0 pg/g lipid by the mid-2000s, tracking the reduction in industrial dioxin emissions achieved through environmental regulations.
7. Detoxification and Reduction Strategies
Dietary Approaches
Chlorella supplementation: Several animal and limited human studies suggest that Chlorella pyrenoidosa, a single-celled green alga, may accelerate fecal excretion of dioxins and PCBs. Proposed mechanisms include adsorption of dioxins in the gut, interruption of enterohepatic recirculation, and induction of hepatic biotransformation enzymes. A Japanese study by Morita et al. (1999) demonstrated that Chlorella supplementation in nursing mothers significantly reduced dioxin concentrations in breast milk over a 3-month period compared to controls. However, the clinical evidence base remains limited and Chlorella's effects are modest compared to the long half-life of stored dioxins.
Dietary fiber: Soluble and insoluble dietary fiber may reduce dioxin absorption from the gastrointestinal tract and facilitate fecal excretion. Fiber-rich foods (whole grains, legumes, fruits, vegetables) support gut microbiome diversity and bile acid excretion, potentially reducing enterohepatic recirculation of dioxins. Psyllium husk and other bulk-forming fibers have been studied in the context of POPs elimination.
Cruciferous vegetables: Indole-3-carbinol (I3C) and its condensation product diindolylmethane (DIM), derived from cruciferous vegetables (broccoli, Brussels sprouts, cabbage, cauliflower), modulate AhR signaling and induce phase I and phase II detoxification enzymes. I3C has been shown to compete with TCDD for AhR binding and to promote excretion of some dioxin congeners in animal models. Regular consumption of cruciferous vegetables (3–5 servings per week) is consistent with general cancer-prevention dietary recommendations.
Olestra studies: Olestra (sucrose polyester) is a non-absorbable fat substitute that binds lipophilic compounds in the gut, preventing their absorption. A landmark study by Moser and Aungst (1999) and subsequent work demonstrated that Olestra consumption significantly increased fecal excretion of PCBs and dioxins in humans and animals. In a controlled trial, regular Olestra consumption reduced serum hexachlorobenzene concentrations and was associated with modest reductions in dioxin-like compounds. However, Olestra is no longer widely available as a food ingredient, limiting its practical application.
Weight Loss Caution — Dioxin Mobilization
Because dioxins are stored in adipose tissue, weight loss — particularly rapid weight loss — releases stored dioxins into the bloodstream as fat is catabolized. Studies have documented transient increases in serum dioxin concentrations during periods of rapid weight loss, including calorie restriction, bariatric surgery, and intensive exercise regimens. This phenomenon has been called “dioxin mobilization” or “stored toxin release.”
The clinical significance of this mobilization is uncertain. Blood concentration spikes are temporary and dioxins are eventually re-deposited in remaining adipose stores or excreted. Nevertheless, individuals with known high dioxin body burden (occupational exposures, contamination incident survivors) should pursue gradual rather than rapid weight loss, and pregnant or nursing women should be aware that rapid weight loss could potentially increase fetal or infant dioxin exposure.
Reducing Dietary Fat and Selecting Lower-Risk Foods
Since more than 90% of dioxin exposure occurs via high-fat animal foods, dietary modification represents the most practical population-wide strategy for reducing intake:
- Trim visible fat from meat and remove poultry skin before cooking
- Choose lower-fat dairy options (skim milk, reduced-fat cheese)
- Moderate consumption of high-fat Baltic Sea fish (herring, eel, salmon); favor lean white fish or fish from less-contaminated waters
- Prefer baked, broiled, or steamed preparations over frying, as some fat (and associated dioxins) drips away during cooking of fatty meats
- Increase plant-based foods in the diet, which carry negligible dioxin contamination
8. Regulatory Standards
World Health Organization (WHO) Tolerable Intake
The WHO established a tolerable monthly intake (TMI) of 70 pg WHO-TEQ/kg body weight per month for dioxins and dioxin-like PCBs combined (equivalent to approximately 2.3 pg TEQ/kg body weight per day). This value was derived from the lowest observed adverse effect levels (LOAELs) in the most sensitive animal and human studies, applying appropriate safety factors. The European Food Safety Authority (EFSA) conducted a re-evaluation in 2018 and recommended a substantially lower tolerable weekly intake (TWI) of 2 pg TEQ/kg body weight per week (approximately 0.29 pg/kg/day), based on more sensitive endpoints including developmental neurotoxicity and endocrine disruption.
European Union Maximum Levels in Food
EU Regulation (EU) 2023/915 (consolidating earlier regulations) sets maximum levels for dioxins and dioxin-like PCBs in food. Representative limits include:
- Beef, pork, poultry, and lamb fat: 1.75 pg WHO-TEQ/g fat (dioxins + furans); 4.0 pg WHO-TEQ/g fat (dioxins + furans + dioxin-like PCBs)
- Liver and derived products: 4.5 pg WHO-TEQ/g fat; 12 pg WHO-TEQ/g fat (including dioxin-like PCBs)
- Fish muscle: 3.5 pg WHO-TEQ/g wet weight; 6.5 pg WHO-TEQ/g wet weight (including dioxin-like PCBs)
- Cow's milk and dairy products: 2.5 pg WHO-TEQ/g fat; 5.5 pg WHO-TEQ/g fat (including dioxin-like PCBs)
- Hen eggs: 2.5 pg WHO-TEQ/g fat; 5.0 pg WHO-TEQ/g fat (including dioxin-like PCBs)
U.S. EPA Standards
The U.S. Environmental Protection Agency published a comprehensive dioxin reassessment in 2012 concluding that TCDD is a known human carcinogen. The EPA cancer slope factor for TCDD is 1 × 105 per pg/kg/day (i.e., a daily lifetime exposure of 1 pg TCDD/kg body weight corresponds to a theoretical excess lifetime cancer risk of approximately 1 in 100,000). The EPA has proposed but not finalized a formal reference dose (RfD) for non-cancer endpoints. The FDA regulates dioxin levels in specific food categories through enforcement discretion levels and import alerts.
Stockholm Convention POPs
The Stockholm Convention lists unintentionally produced PCDDs and PCDFs in its Annex C (unintentional releases), requiring parties to develop and implement national action plans to reduce total releases from all source categories. The Convention also lists certain dioxin-like PCBs (Annex A, elimination) and requires parties to develop inventories of polychlorinated dibenzo-p-dioxin and dibenzofuran releases based on best available techniques (BAT) and best environmental practices (BEP). Parties are required to report on progress every four years, and global dioxin emission inventories maintained by UNEP document the substantial progress achieved in reducing emissions from developed nations.
9. Recent Research and Advances
Non-genomic AhR signaling: Research published in the 2010s–2020s has established that AhR exerts biological effects through pathways independent of DRE-driven gene transcription — so-called “non-genomic” or “extra-nuclear” AhR signaling. These include rapid activation of kinase cascades (Src, EGFR), modulation of the cytoskeleton, and cross-talk with Wnt/β-catenin and Notch signaling. Non-genomic AhR effects may explain some acute toxicity endpoints that occur at concentrations too low or too rapidly to be explained by transcriptional changes alone.
Epigenetic mechanisms: Studies have demonstrated that dioxin exposure produces lasting epigenetic modifications — changes in DNA methylation patterns and histone modifications — at promoters of AhR-responsive and immune-regulatory genes. These epigenetic marks can persist long after the compound is eliminated and may contribute to the long-term health consequences of even transient high-dose exposures. Transgenerational epigenetic effects of TCDD have been documented in rodent models, raising questions about inherited effects in human populations with historical high-dose exposures.
Gut microbiome interactions: Emerging research has identified the gut microbiome as both a target of and modulator of dioxin toxicity. Germ-free mice show altered responses to TCDD compared to conventionally colonized mice. Certain gut bacteria produce tryptophan-derived AhR ligands that compete with dioxins for receptor binding. Conversely, dioxin exposure has been shown to alter microbiome composition in animal models, potentially contributing to metabolic and immune effects. This research area is rapidly evolving and may identify probiotic interventions for reducing dioxin toxicity.
Low-dose effects and non-monotonic dose-response: Several studies have reported biological effects of dioxins at doses at or below current tolerable intake values, and some endpoints (particularly endocrine-sensitive outcomes) show non-monotonic (U-shaped or inverted U-shaped) dose-response relationships. These findings challenge traditional toxicological assumptions and have led to ongoing scientific debate about the adequacy of current regulatory limits, particularly for sensitive populations (infants, pregnant women).
Remediation technology advances: In-situ bioremediation approaches using dioxin-dechlorinating bacteria (including species of Dehalococcoides and related anaerobic organisms) have been demonstrated in laboratory and pilot field studies. Phytoremediation using high-lipid plants to extract dioxins from shallow soils is also under investigation. High-temperature incineration (>1,100°C with rapid quench) remains the regulatory gold standard for dioxin-contaminated soil treatment but is expensive and energy-intensive.
Declining body burden and population trends: National and international biomonitoring programs confirm continued declining trends in blood dioxin TEQ concentrations across developed nations, attributed to reduced industrial emissions. However, modeling studies suggest that the rate of decline is slowing as background environmental concentrations approach a new steady state driven by natural re-emission of deposited dioxins from soils and sediments. Emerging economies with rapidly growing waste incineration and metal smelting sectors may be experiencing increasing dioxin exposures, representing a global equity dimension to dioxin risk management.
10. Related Topics
- Heavy Metals in Food
- Pesticides
- BPA and Plastics
- Chlorella (natural detoxification support)
- Polychlorinated Biphenyls (PCBs)
11. References
- Van den Berg M, Birnbaum LS, Denison M, et al. The 2005 World Health Organization reevaluation of human and mammalian toxic equivalency factors for dioxins and dioxin-like compounds. Toxicol Sci. 2006;93(2):223–241.
- IARC Working Group. Polychlorinated dibenzo-para-dioxins and polychlorinated dibenzofurans. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. 1997;69:33–343. IARC Monographs Vol. 69
- Consonni D, Pesatori AC, Zocchetti C, et al. Mortality in a population exposed to dioxin after the Seveso, Italy, accident in 1976: 25 years of follow-up. Am J Epidemiol. 2008;167(7):847–858.
- Eskenazi B, Mocarelli P, Warner M, et al. Serum dioxin concentrations and breast cancer risk in the Seveso Women's Health Study. Environ Health Perspect. 2004;112(16):1561–1566.
- Mocarelli P, Gerthoux PM, Ferrari E, et al. Paternal concentrations of dioxin and sex ratio of offspring. Lancet. 2000;355(9218):1858–1863.
- Poland A, Knutson JC. 2,3,7,8-Tetrachlorodibenzo-p-dioxin and related halogenated aromatic hydrocarbons: examination of the mechanism of toxicity. Annu Rev Pharmacol Toxicol. 1982;22:517–554.
- Mimura J, Fujii-Kuriyama Y. Functional role of AhR in the expression of toxic effects by TCDD. Biochim Biophys Acta. 2003;1619(3):263–268.
- Birnbaum LS. The mechanism of dioxin toxicity: relationship to risk assessment. Environ Health Perspect. 1994;102(Suppl 9):157–167.
- Schecter A, Birnbaum L, Ryan JJ, Constable JD. Dioxins: an overview. Environ Res. 2006;101(3):419–428.
- EFSA CONTAM Panel. Risk for animal and human health related to the presence of dioxins and dioxin-like PCBs in feed and food. EFSA Journal. 2018;16(11):5333.
- Fierens S, Mairesse H, Heilier JF, et al. Dioxin/polychlorinated biphenyl body burden, diabetes and endometriosis: findings in a population-based study in Belgium. Biomarkers. 2003;8(6):529–534.
- Morita K, Ogata M, Hasegawa T. Chlorophyll derived from Chlorella inhibits dioxin absorption from the gastrointestinal tract and accelerates dioxin excretion in rats. Environ Health Perspect. 2001;109(3):289–294.
- Liem AK, Furst P, Rappe C. Exposure of populations to dioxins and related compounds. Food Addit Contam. 2000;17(4):241–259.
- Startin JR. Sources and fate of PCDDs and PCDFs in food and humans. Food Addit Contam. 1994;11(4):473–480.
- Hanrahan LP, Falk C, Anderson HA, et al. Serum PCB and DDE levels of frequent Great Lakes sport fish consumers — a first look. Environ Res. 1999;80(2 Pt 2):S26–S37.
- Baccarelli A, Giacomini SM, Corbetta C, et al. Neonatal thyroid function in Seveso 25 years after maternal exposure to dioxin. PLoS Med. 2008;5(7):e161.
- Viel JF, Clement MC, Hagi M, Grandjean S, Challier B, Danzon A. Dioxin emissions from a municipal solid waste incinerator and risk of invasive breast cancer: a population-based case-control study with GIS-derived exposure. Int J Health Geogr. 2008;7:4.
- U.S. EPA. Exposure and Human Health Reassessment of 2,3,7,8-Tetrachlorodibenzo-p-Dioxin (TCDD) and Related Compounds — National Academy of Sciences External Review Draft. EPA/600/P-00/001Cb. Washington, DC: U.S. EPA; 2012. EPA Dioxin Reassessment
- Schecter A, Pavuk M, Päpke O, Ryan JJ, Birnbaum L, Rosen R. Polybrominated diphenyl ethers (PBDEs) in U.S. mothers' milk. Environ Health Perspect. 2003;111(14):1723–1729.
- Rowlands JC, Gustafsson JA. Aryl hydrocarbon receptor-mediated signal transduction. Crit Rev Toxicol. 1997;27(2):109–134.
Connections
- PCBs
- Heavy Metals
- Pesticides
- BPA and Plastics
- Chlorella
- Cancer
- Endometriosis
- Sarcoma
- Lymphoma
- Detoxification
- Gut Brain Axis
- Gut Microbiome
- Milk
- Eggs
- Salmon
- Beef
- Type 2 Diabetes
- Sucralose