Common Human Parasites
Human parasites divide naturally into three biological categories: protozoa (single-celled organisms like Giardia, Entamoeba, Cryptosporidium, Toxoplasma), helminths (parasitic worms including roundworms, flatworms, and tapeworms), and ectoparasites (lice, scabies, demodex mites). Each category has distinct biology, transmission routes, diagnostic approaches, and pharmacotherapy. This page walks through the species most relevant to humans in both developed and developing settings, the signs and symptoms that should prompt clinical evaluation, the diagnostic tests that actually find them (stool microscopy is far less sensitive than commonly assumed), and the conventional drug treatments still considered first-line for each.
Table of Contents
- The Three Categories of Human Parasites
- Protozoa — The Single-Celled Parasites
- Nematodes (Roundworms)
- Cestodes (Tapeworms)
- Trematodes (Flukes)
- Ectoparasites
- Common Transmission Routes
- Clinical Symptoms and When to Suspect Parasitism
- Diagnostic Approach
- Conventional Pharmacotherapy
- Key Research Papers
- Connections
- Featured Videos
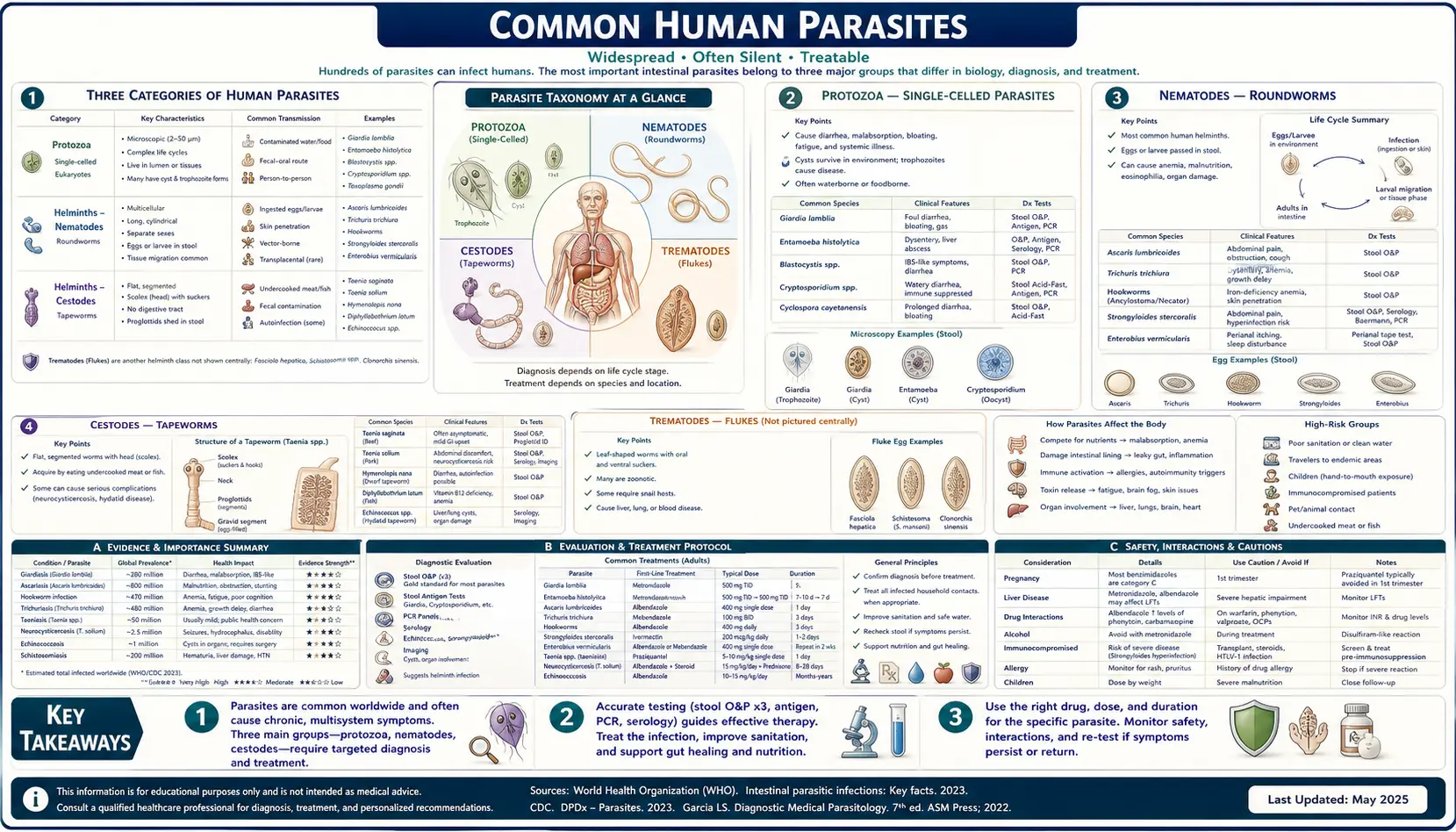
The Three Categories of Human Parasites
A parasite is any organism that lives on or in a host of another species and derives its nutrition at the host's expense. By this strict biological definition, all infectious bacteria and viruses are parasites — but conventional medical usage restricts the term "parasite" to eukaryotic organisms (cells with a nucleus). This restricts the discussion to three groups that have very different biology and require different therapeutic approaches:
- Protozoa — single-celled eukaryotes. They reproduce asexually inside the host (often as cysts shed in feces) and can have explosive intra-host population growth from a single infectious organism.
- Helminths — multicellular worms. Subdivided into nematodes (roundworms, segmented body), cestodes (tapeworms, flat segmented body), and trematodes (flukes, leaf-shaped unsegmented). With few exceptions, helminths cannot multiply inside the host — one ingested egg or larva becomes one adult worm, and the worm load reflects cumulative exposure rather than intra-host reproduction.
- Ectoparasites — arthropods that live on the skin surface (lice, scabies mites, demodex) or attach briefly to feed (ticks, fleas, bedbugs). Treatment is usually topical.
This three-category distinction matters for treatment design. Protozoa often need prolonged or repeat courses to clear because of rapid reproduction. Helminths often respond to a single dose because reproduction within the host is absent or limited. Ectoparasite treatment is usually a one-time topical application with a repeat at 7-14 days to catch hatching eggs.
Protozoa — The Single-Celled Parasites
Giardia lamblia (also called Giardia intestinalis or Giardia duodenalis) is the most common waterborne parasite in the US and the world. Trophozoites attach to the small intestinal mucosa via a ventral adhesive disc; the resulting villous blunting causes malabsorption, fat-laden floating stools (steatorrhea), abdominal cramping, and chronic fatigue. The infectious dose is as low as 10 cysts. Transmission is via contaminated water (untreated mountain stream water, daycare/childcare settings, pool water swallowed by children, fecal-oral spread). First-line treatment: tinidazole single dose 2 g or metronidazole 250-500 mg three times daily for 5-7 days. Nitazoxanide is an alternative.
Entamoeba histolytica causes amoebic dysentery and, in a smaller fraction of cases, amoebic liver abscess (the parasite traverses the colonic wall, enters the portal circulation, and forms hepatic abscesses, classically right-lobe). Distinction from the non-pathogenic Entamoeba dispar (morphologically identical on microscopy) requires antigen testing or PCR. Treatment: metronidazole 750 mg three times daily for 10 days followed by a luminal agent like paromomycin or iodoquinol to eradicate residual cysts.
Cryptosporidium (C. parvum and C. hominis) is a leading cause of waterborne diarrhea outbreaks (Milwaukee 1993 outbreak: 400,000 cases from municipal water contamination). Oocysts are chlorine-resistant and require either filtration or UV/ozone for water treatment. Disease is usually self-limited in immunocompetent hosts (1-2 weeks of watery diarrhea) but can be devastating and chronic in HIV/AIDS or transplant patients. Nitazoxanide is the only FDA-approved treatment.
Toxoplasma gondii is the protozoan with which 11-12% of US adults (and approximately one-third of humans globally) have been infected. Cats are the definitive host (sexual reproduction in the feline gut), but humans can acquire infection from undercooked meat (tissue cysts) or from environmental exposure to oocyst-contaminated soil or cat litter. Acute infection in immunocompetent adults is usually asymptomatic or causes a mild mononucleosis-like illness. The major clinical concerns are congenital transmission (severe brain and eye disease in the fetus if a mother seroconverts during pregnancy) and reactivation in immunosuppressed hosts (toxoplasma encephalitis in AIDS).
Blastocystis hominis is the most commonly detected organism on stool ova-and-parasite testing in symptomatic and asymptomatic individuals. Its pathogenicity remains controversial — some subtypes appear to cause IBS-like symptoms, while others appear to be commensal. Treatment is reserved for symptomatic patients in whom other causes have been excluded: metronidazole, nitazoxanide, or trimethoprim-sulfamethoxazole.
Trichomonas vaginalis is a sexually transmitted protozoan and the most common non-viral STI worldwide (CDC estimates 2 million US infections per year). Causes vaginitis in women and usually asymptomatic urethritis in men. Treatment: metronidazole or tinidazole single dose 2 g for both partners.
Nematodes (Roundworms)
Ascaris lumbricoides is the largest and most common intestinal worm globally — WHO estimates ~800 million people infected, mostly in tropical and subtropical regions with poor sanitation. Eggs ingested from fecally contaminated soil hatch in the duodenum; larvae penetrate the gut wall, migrate through the liver and lungs (the Loeffler syndrome of pulmonary eosinophilia and cough), are coughed up and swallowed, and mature into adult worms 15-35 cm long in the small intestine. Treatment: single-dose albendazole 400 mg or mebendazole 100 mg twice daily for 3 days.
Enterobius vermicularis (pinworm) is the most common worm in the US, particularly in school-age children. Female worms exit the anus at night to lay eggs on perianal skin, causing the classic nocturnal anal itch. Diagnosis is the "scotch tape test" (clear adhesive tape pressed to the perianal skin in the morning and examined for eggs). Treatment: single-dose pyrantel pamoate (over-the-counter as Reese's Pinworm Medicine) or albendazole, repeated in 2 weeks to catch eggs hatched after the first dose. The entire household should be treated, and bedding/clothing washed.
Necator americanus and Ancylostoma duodenale (hookworm) infect ~700 million people globally. Larvae in soil penetrate intact skin (typically through bare feet), migrate through lungs, are swallowed, and attach to the duodenal/jejunal mucosa with their hooked mouthparts, where they feed on blood. The chronic blood loss (each Necator worm consumes ~0.03 mL/day, each Ancylostoma ~0.15 mL/day) is a major cause of iron-deficiency anemia in endemic populations. Treatment: albendazole or mebendazole.
Trichuris trichiura (whipworm) embeds its threadlike anterior end into the colonic mucosa and is the third member of the "soil-transmitted helminth" trio with Ascaris and hookworm. Heavy infections cause chronic dysentery and rectal prolapse in children. Treatment is less reliably curative than for the other STH; albendazole multi-day courses are preferred.
Strongyloides stercoralis deserves special mention because it is the one nematode that can autoinfect — larvae can re-penetrate the gut wall or perianal skin, producing a self-sustaining infection that can persist for decades after the original exposure. In an immunosuppressed host (corticosteroids, transplant, HTLV-1 coinfection), autoinfection can become hyperinfection with massive larval burden, sepsis, and high mortality. Anyone with potential exposure who will receive immunosuppression should be screened. Treatment: ivermectin 200 mcg/kg, often as two doses 2 weeks apart.
Cestodes (Tapeworms)
Tapeworms are flat, segmented worms attached to the intestinal wall by a scolex (head with hooks and/or suckers). They lack a digestive tract and absorb nutrients directly across their tegument from the host's intestinal lumen. Each gravid proglottid (segment) packed with eggs detaches and is shed in feces.
Taenia saginata (beef tapeworm) — humans acquire it by eating raw or undercooked beef containing cysticerci. The adult worm in the small intestine can reach 4-12 meters in length and live 25+ years. Symptoms are often minimal beyond passage of proglottids in the stool. Treatment: single-dose praziquantel 5-10 mg/kg.
Taenia solium (pork tapeworm) is biologically more serious than beef tapeworm because the human can serve as either the definitive host (adult worm in the intestine, acquired from undercooked pork) or the intermediate host (cysticerci in tissue, acquired from ingesting eggs from fecally contaminated food or via autoinfection from one's own intestinal adult worm). Neurocysticercosis — T. solium cysticerci in the brain — is the leading cause of acquired epilepsy in the developing world and is increasingly seen in the US Southwest. Treatment of intestinal infection is praziquantel; neurocysticercosis requires albendazole plus corticosteroids and often antiepileptics.
Diphyllobothrium latum (fish tapeworm) — the largest human tapeworm (10+ meters), acquired from raw or undercooked freshwater fish (the historic exposure was pike and other Great Lakes / Baltic fish; modern sushi-grade salmon farming has reduced but not eliminated risk). Unique among human parasites in causing megaloblastic anemia through competitive uptake of vitamin B12. Treatment: praziquantel.
Hymenolepis nana (dwarf tapeworm) — the only human tapeworm that completes its entire life cycle in a single host (no intermediate host required) and can autoinfect. Common in children in tropical regions. Treatment: praziquantel 25 mg/kg single dose.
Echinococcus granulosus and multilocularis — the canine tapeworms that cause hydatid disease and alveolar echinococcosis when humans serve as accidental intermediate hosts. Slow-growing cysts in liver, lung, brain. Treatment is often surgical, with long-course albendazole.
Trematodes (Flukes)
Schistosoma species (mansoni, haematobium, japonicum) cause schistosomiasis, the second most prevalent parasitic disease worldwide after malaria. Cercariae released from infected freshwater snails penetrate human skin during water contact, mature into adult worms that pair-bond in the mesenteric or vesical venous plexus, and lay eggs that cause chronic granulomatous inflammation in liver, intestine, or bladder. S. haematobium chronic infection is a strong risk factor for bladder squamous cell carcinoma. Treatment: praziquantel.
Fasciola hepatica (liver fluke) — acquired from eating watercress or other freshwater plants harboring metacercariae. The fluke migrates through the liver into the bile ducts, causing acute right-upper-quadrant pain, fever, and eosinophilia followed by chronic biliary disease. Treatment: triclabendazole (not stocked at most US pharmacies; available from CDC).
Clonorchis sinensis and Opisthorchis viverrini (Asian liver flukes) — from raw or undercooked freshwater fish. Chronic infection is a documented risk factor for cholangiocarcinoma. Treatment: praziquantel.
Ectoparasites
Pediculus humanus capitis (head lice) — estimated 6-12 million US infestations per year, mostly school-age children. Treatment: permethrin 1% or pyrethrin OTC, ivermectin lotion, or spinosad. Wet combing and mechanical removal is essential because resistance to permethrin is widespread.
Sarcoptes scabiei (scabies mite) — mites burrow into the epidermis, especially in finger webs, wrists, axillae, and genitals. Intense itch, especially nocturnal. Treatment: permethrin 5% cream from neck down, washed off after 8-14 hours, repeated in 7-14 days. Oral ivermectin 200 mcg/kg as an alternative or for crusted (Norwegian) scabies in immunosuppressed hosts.
Demodex folliculorum and brevis — mites residing in hair follicles and sebaceous glands, present on most adult faces. Associated with rosacea, blepharitis, and pityriasis folliculorum when overpopulated. Treatment: ivermectin 1% cream (Soolantra), tea tree oil eyelid scrubs.
Common Transmission Routes
- Fecal-oral via contaminated water — Giardia, Cryptosporidium, Entamoeba histolytica
- Fecal-oral via contaminated food (unwashed vegetables, fertilizer) — Ascaris, Trichuris, Toxoplasma oocysts
- Soil penetration of bare skin — hookworms, Strongyloides, schistosome cercariae from freshwater contact
- Undercooked meat with cysts — Taenia (beef and pork), Trichinella (pork, bear, wild game), Toxoplasma
- Raw freshwater fish — Diphyllobothrium, Clonorchis, Opisthorchis
- Mosquito or sandfly bite — malaria (Plasmodium), Leishmania, Trypanosoma
- Reduviid bug (kissing bug) bite — Trypanosoma cruzi (Chagas disease)
- Sexual contact — Trichomonas vaginalis, pubic lice (Pthirus pubis)
- Direct person-to-person — pinworm, scabies, head lice
- Cat litter / cat contact — Toxoplasma oocysts shed in feces
- Daycare / institutional settings — Giardia, pinworm, Hymenolepis
Clinical Symptoms and When to Suspect Parasitism
Parasitic infection rarely produces a single pathognomonic symptom. Suspicion should be raised by combinations of:
- Chronic unexplained GI symptoms — especially intermittent diarrhea, fat-laden floating stools, bloating, abdominal cramping, particularly after travel or water exposure
- Unexplained iron-deficiency anemia — particularly in someone with potential hookworm exposure or any GI parasitism with chronic occult blood loss
- Eosinophilia >500 cells/µL on CBC — strongly suggestive of tissue-invasive helminth (Strongyloides, hookworm migration, schistosomiasis, filariasis, toxocariasis). Eosinophilia does not occur with protozoa or with intraluminal-only worm infection.
- Nocturnal anal itch — classic pinworm
- B12 deficiency in someone who eats fish — consider Diphyllobothrium
- Right-upper-quadrant pain plus fever plus eosinophilia — consider liver fluke or amoebic abscess
- New-onset seizures in someone from a T. solium-endemic area — consider neurocysticercosis
- Intense itch in fingerwebs/wrists, family members affected — scabies
- Visible worm or proglottids in stool — Ascaris or Taenia respectively
Diagnostic Approach
The traditional gold standard — stool ova-and-parasite (O&P) examination — has surprisingly limited sensitivity. A single stool examination detects approximately 50% of established infections; three stool specimens collected on different days raise sensitivity to about 85% for many parasites. For pinworm, scotch tape testing of the perianal area in the early morning is more sensitive than stool O&P. For Giardia, Cryptosporidium, and Entamoeba histolytica, stool antigen tests (ELISA or rapid immunoassay) are now preferred over microscopy for sensitivity.
Molecular PCR multiplex panels (BioFire, xTAG GPP) detect parasitic DNA alongside bacterial and viral pathogens and have dramatically improved sensitivity for clinical decision-making, though they cannot distinguish viable from dead organisms. Serology (specific IgG/IgM) is useful for tissue-invasive parasites where stool testing misses the organism: schistosomiasis, strongyloidiasis (with caveat of cross-reactivity in filariasis), Toxoplasma, Toxocara, cysticercosis.
For diagnosis of intestinal parasitism more broadly, the comprehensive ordering pattern includes: CBC with differential (eosinophilia), three stool O&P specimens, Giardia/Cryptosporidium antigen, scotch tape if pinworm suspected, and serology for tissue-invasive parasites if exposure history warrants. See our stool testing page for more on the diagnostic options.
Conventional Pharmacotherapy
- Albendazole 400 mg — Ascaris, hookworm, pinworm, Strongyloides, neurocysticercosis (long course)
- Mebendazole 100-500 mg — soil-transmitted helminths (similar spectrum to albendazole)
- Pyrantel pamoate — OTC for pinworm, Ascaris, hookworm
- Ivermectin 200 mcg/kg — Strongyloides, scabies, head lice, filariasis, onchocerciasis
- Praziquantel — tapeworms (cestodes), flukes (trematodes including schistosomiasis)
- Metronidazole 250-750 mg three times daily — Giardia, Entamoeba histolytica (followed by luminal agent), Trichomonas, anaerobic bacteria
- Tinidazole 2 g single dose — Giardia, Trichomonas, amoebiasis (better tolerated than metronidazole)
- Nitazoxanide 500 mg twice daily for 3 days — Cryptosporidium (only FDA-approved), Giardia, Hymenolepis, broad spectrum
- Paromomycin / iodoquinol — luminal amoebicides after metronidazole for E. histolytica
- Permethrin 5% cream — scabies, repeat in 7-14 days
- Triclabendazole — Fasciola hepatica (CDC-only stock in US)
The botanical alternatives (Hulda Clark's wormwood-clove-black walnut triplet, pumpkin seeds) discussed in the sister pages are not substitutes for these proven first-line drugs in confirmed serious infection — Strongyloides hyperinfection, neurocysticercosis, severe amoebic dysentery, and visceral schistosomiasis are not appropriate targets for botanical-only treatment. Botanicals have a defensible role in periodic preventive cleansing and in adjunctive support in mild infections, particularly where access to pharmacotherapy is limited or where lower-toxicity alternatives are preferred for prophylactic use.
Key Research Papers
- Bethony J et al. (2006). Soil-transmitted helminth infections: ascariasis, trichuriasis, and hookworm. The Lancet. — PubMed
- Hotez PJ et al. (2008). Helminth infections: the great neglected tropical diseases. Journal of Clinical Investigation. — PubMed
- Adam RD (2001). Biology of Giardia lamblia. Clinical Microbiology Reviews. — PubMed
- Stanley SL (2003). Amoebiasis. The Lancet. — PubMed
- Mac Kenzie WR et al. (1994). A massive outbreak in Milwaukee of Cryptosporidium infection transmitted through the public water supply. NEJM. — PubMed
- Montoya JG, Liesenfeld O (2004). Toxoplasmosis. The Lancet. — PubMed
- Garcia HH et al. (2003). Taenia solium cysticercosis. The Lancet. — PubMed
- Olds GR, Dasarathy S (2000). Strongyloidiasis. Clinical Microbiology Reviews. — PubMed
- Gryseels B et al. (2006). Human schistosomiasis. The Lancet. — PubMed
- Currie BJ, McCarthy JS (2010). Permethrin and ivermectin for scabies. NEJM. — PubMed
- Jones JL et al. (2014). Toxoplasma gondii infection in the United States, 2011-2014. American Journal of Tropical Medicine and Hygiene. — PubMed
- Stensvold CR, Clark CG (2016). Current status of Blastocystis: a personal view. Parasitology International. — PubMed
PubMed Topic Searches
- PubMed: Human parasite US epidemiology
- PubMed: O&P diagnostic sensitivity
- PubMed: Anthelmintic drug review
- PubMed: Eosinophilia helminth workup
- PubMed: Stool multiplex PCR
Connections
- Parasites Overview
- Parasites Benefits Hub
- Wormwood, Clove & Black Walnut
- Pumpkin Seeds
- Cycle & Detox Symptoms
- Wormwood
- Clove
- Black Walnut
- Pumpkin Seeds
- SIBO
- IBS
- Crohn's Disease
- Stool Testing
- Iron (Hookworm Anemia)
- Vitamin B12 (Fish Tapeworm)