Parasite Cleanse Cycle and Detox Symptoms
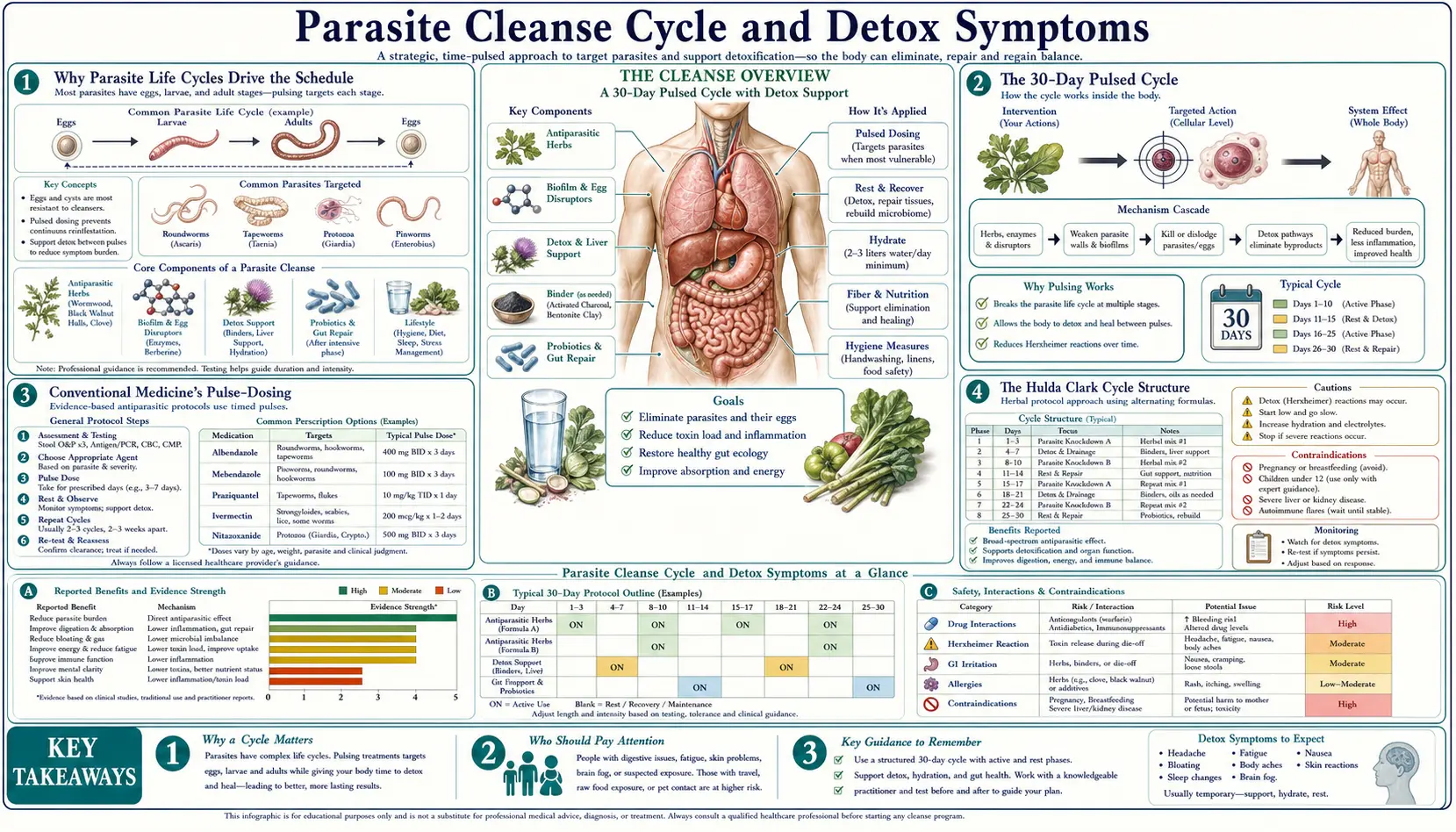
A parasite cleanse done correctly is not a single dose — it is a 30-day pulsed cycle designed to catch the parasite at every life-cycle stage from egg to gravid adult. The pulsed schedule reflects the underlying biology: most helminth eggs hatch within 1-2 weeks of being laid, and an antiparasitic dose that kills today's adults must be followed by a second dose 2 weeks later to kill the next generation that emerges from eggs that survived the first round. This page walks through the 30-day cycle structure used by both conventional medicine (the standard 2-week-repeat for albendazole/mebendazole) and the alternative Hulda Clark protocol, the rationale for pulsing rather than continuous dosing, and the most important practical knowledge for any cleanse: how to recognize the Jarisch-Herxheimer "die-off" reaction, distinguish it from genuine adverse effects, and support the body through it with binders, hydration, electrolytes, and liver-support nutrients.
Table of Contents
- Why Parasite Life Cycles Drive the Schedule
- The 30-Day Pulsed Cycle
- Conventional Medicine's Pulse-Dosing
- The Hulda Clark Cycle Structure
- The Jarisch-Herxheimer Reaction
- Detox Symptoms vs Genuine Adverse Effects
- Supportive Measures: Binders
- Hydration and Electrolytes
- Liver-Support Nutrients
- Red Flags Requiring Medical Evaluation
- Key Research Papers
- Connections
- Featured Videos
Why Parasite Life Cycles Drive the Schedule
Almost all helminth parasites go through several distinct life-cycle stages between egg and reproductive adult: egg, larva (often with one or more molts), and adult. Many also include encysted or migratory stages that are biologically distinct from the intraluminal adult. The relevance for anthelmintic dosing is that different stages have dramatically different susceptibilities to the same drug. An egg is essentially metabolically dormant, sealed inside a tough proteinaceous shell — it is highly resistant to most drugs. A migrating larva in tissue is more susceptible. A mature adult worm in the intestinal lumen is the most accessible target.
This means a single dose of even an effective anthelmintic is unlikely to clear the infection completely. The drug kills the adults, but eggs already laid in the gut and shed in stool remain viable. Eggs ingested or autoinfecting in the days before treatment continue to develop and hatch into new larvae after the drug is cleared from the body. Within 1-2 weeks, the new generation reaches adulthood and reestablishes the patent infection.
The pulse-dosing solution: give an initial course to kill all adults, wait 1-2 weeks for the remaining eggs to hatch (so they are now larvae or young adults, much more susceptible to the next drug exposure), then give a second course to kill that new generation before it can reproduce. For some parasites with longer development cycles (large tapeworms, schistosomes), a third pulse at 4-6 weeks may be needed.
The most familiar example in conventional medicine is pinworm treatment. The CDC and standard pediatric guidelines recommend pyrantel pamoate or mebendazole as a single dose, repeated 2 weeks later. The 2-week interval is chosen to match the pinworm life cycle — pinworm eggs ingested before or during the first dose hatch in the small intestine, mature into adult worms in the cecum and ascending colon, and migrate to the anal verge approximately 2 weeks later. The second dose catches this next generation before they can lay eggs and continue the cycle.
The same principle applies to all soil-transmitted helminths (Ascaris, hookworm, whipworm) and to tapeworms. WHO mass-deworming programs use albendazole or mebendazole semi-annually, with each dose providing approximately 6-month protection against the slow re-establishment of patent infection from environmental egg load.
The 30-Day Pulsed Cycle
A 30-day cycle covers the typical helminth life-cycle range and provides for at least two pulse-dose intervals. The standard structure:
- Days 1-7: Initial intensive phase. Daily dosing of all chosen antiparasitic agents. Gradual escalation in the case of botanical agents to allow titration to tolerance. This phase targets all adult worms currently in the gut and most actively developing larvae.
- Days 8-14: Rest and recovery phase. No antiparasitic dosing (or a reduced maintenance dose). The body clears die-off products from the first phase. The remaining eggs from the original infection hatch, and the new larvae mature in the gut wall and mucosa.
- Days 15-21: Second intensive phase. Repeat the initial intensive dosing. The newly emerged generation of larvae and young adults is now exposed to the antiparasitic and killed before it can reproduce.
- Days 22-30: Recovery and maintenance. Reduced or weekly maintenance dosing. Continued supportive measures (binders, liver support). Any residual eggs or migrating larvae may emerge in this window and are caught by maintenance-dose drug levels.
For maintenance after the initial 30-day cycle, weekly pulsed dosing for 3-6 months is the typical recommendation, with the schedule gradually tapering. Many integrative practitioners recommend an annual or semiannual maintenance cleanse as long-term prophylaxis, particularly for pet owners, frequent international travelers, raw-meat consumers, or anyone with risk factors for ongoing exposure.
Conventional Medicine's Pulse-Dosing
The pulse-dosing concept is not exclusive to alternative medicine; it is standard pharmacotherapy practice for helminth infections:
- Pinworm (Enterobius): pyrantel pamoate 11 mg/kg or mebendazole 100 mg, single dose, REPEATED 2 weeks later. CDC standard recommendation.
- Soil-transmitted helminths (mass treatment): albendazole 400 mg single dose, biannually (every 6 months). WHO guidance for endemic regions.
- Strongyloides: ivermectin 200 mcg/kg, REPEATED in 2 weeks. The autoinfection cycle of Strongyloides makes the repeat critical.
- Scabies: permethrin 5% cream, full-body application, REPEATED in 7-14 days to catch hatching eggs.
- Head lice: permethrin 1% or pyrethrin OTC, REPEATED in 7-10 days. Egg-hatching cycle.
- Schistosomiasis: praziquantel 40 mg/kg, sometimes split into 2 doses 6 hours apart; for heavy infections, REPEAT in 4-6 weeks.
- Neurocysticercosis: albendazole 15 mg/kg/day for 10-14 days (longer course addresses encysted tissue larvae).
The 2-week interval is the most common pulse spacing because it corresponds to the time required for most helminth eggs to hatch and develop into susceptible early-larval forms. For parasites with longer or shorter cycles, the interval is adjusted accordingly.
The Hulda Clark Cycle Structure
The classic Hulda Clark Cure for All Diseases protocol applies the same pulse-dosing logic to the wormwood-clove-black walnut triplet:
- Days 1-7: Daily escalation. Black walnut tincture from 1 drop up to 2 teaspoons. Wormwood capsules from 1 up to 7. Clove capsules from 1 up to 3 three times daily. The escalation serves both to titrate to tolerance and to gradually deplete the parasite egg load before higher doses meet the more difficult-to-kill larval stages.
- Days 8-10: Peak intensive. Full doses of all three agents.
- Days 11-30: Weekly maintenance. Full dose of all three taken once weekly. This catches each new generation of larvae as they emerge over the cycle.
- Months 2-6: Indefinite weekly maintenance. Continued weekly dosing of the triplet, plus daily clove (which is gentle enough for daily use and targets the persistent egg-stage problem).
The Clark protocol differs from conventional pulse-dosing primarily in (a) the lower per-pulse intensity (botanical doses are less drug-like in their pharmacokinetics, so the parasite kill per pulse is less dramatic but the cumulative effect over many pulses is significant) and (b) the longer overall duration (months rather than the 2-3 conventional pulses). Many integrative practitioners simplify the Clark protocol while retaining the pulse-dosing principle — e.g., a 14-day course of combined herbal capsules, repeated for one more 14-day course at 2 weeks, then weekly maintenance for 3 months.
The Jarisch-Herxheimer Reaction
The Jarisch-Herxheimer reaction was first described in syphilis patients receiving mercury or penicillin treatment in the late 1800s and early 1900s. Adolf Jarisch (Vienna, 1895) and Karl Herxheimer (Frankfurt, 1902) independently noted that within hours of starting effective antimicrobial therapy, patients often developed fever, chills, headache, myalgia, and worsening of their primary symptoms — symptoms that resolved over 12-24 hours without specific treatment. The reaction is now recognized in a wide range of infections treated with effective antimicrobials, including spirochetal infections (syphilis, Lyme disease, leptospirosis, relapsing fever), some bacterial infections, and notably antiparasitic treatment.
Mechanism: When a large pathogen load is rapidly killed by an effective drug, the dying organisms release their cellular contents into the host's circulation. For gram-negative bacteria, this means lipopolysaccharide (LPS, endotoxin). For spirochetes, it means lipoproteins and outer-membrane components. For parasites, it means a mixture of intracellular contents, surface antigens, dead cell debris, and any toxins the parasite was producing. The host innate immune system recognizes these "pathogen-associated molecular patterns" through TLR4 (for LPS), TLR2 (for many lipoproteins), and other pattern-recognition receptors, triggering a rapid cytokine surge — primarily TNF-alpha, IL-6, and IL-8 — that produces the systemic symptoms.
Typical Herxheimer symptoms:
- Fever and chills (often low-grade, 99-101°F)
- Fatigue, malaise, "flu-like" feeling
- Headache (sometimes severe, sometimes migraine-like)
- Myalgia (muscle aches) and arthralgia (joint aches)
- Increased GI symptoms — nausea, diarrhea, abdominal cramping
- Skin rash, itching, or flushing
- Brain fog, irritability, mood swings
- Increased mucus production (postnasal drip, productive cough)
- Transient worsening of the original symptoms — this is the hallmark
Timing: Onset is typically within hours of the first effective dose. Symptoms usually peak within 24-48 hours and resolve over 1-3 days. In a 30-day parasite cleanse, Herxheimer symptoms tend to recur with each pulse (each new generation of dying parasites triggers a new die-off response), but the intensity typically decreases over successive pulses as the parasite load drops.
Detox Symptoms vs Genuine Adverse Effects
One of the most important practical skills in a parasite cleanse is distinguishing Herxheimer "die-off" reactions from genuine drug or herb adverse effects. The wrong call in either direction is harmful — mistaking an adverse effect for "detox" and continuing the agent can cause real damage; mistaking detox for adverse effect and abandoning an effective protocol leaves the parasitic infection untreated.
Features that suggest Herxheimer/detox:
- Onset within hours of starting an effective antiparasitic
- Worsening of the original symptoms (more GI cramping, more brain fog, more fatigue if those were the presenting issues)
- "Flu-like" symptom pattern — fever, chills, myalgia, headache
- Symptoms peak in 24-48 hours, then resolve over 1-3 days even if the agent is continued
- Symptoms tend to be milder with each subsequent pulse
- Improvement of the original parasitic symptoms once the detox phase passes
- Activated charcoal, bentonite, or other binders reduce intensity
Features that suggest genuine adverse drug effect:
- Symptoms not previously present and not related to the original parasitic complaints
- New rash, particularly hives, target lesions, or mucous membrane involvement — possible drug allergy
- Persistent symptoms that worsen rather than resolve over days
- Symptoms get worse with each dose rather than better
- Specific organ-system signs — jaundice, dark urine, severe abdominal pain (liver), oliguria (kidney), bleeding or bruising (hematologic), severe neurological signs
- Onset hours to days after dose with features atypical for Herxheimer
When in doubt, the safest course is to: (1) stop or reduce the antiparasitic agent, (2) hydrate aggressively, (3) consider a binder, (4) observe for 24-48 hours, and (5) if symptoms resolve, restart at a lower dose. If symptoms persist after stopping the agent or include any of the red-flag features below, seek medical evaluation.
Supportive Measures: Binders
Binders are inert oral substances that bind toxins, endotoxin, and bile-conjugated metabolites in the gut lumen and prevent their reabsorption (enterohepatic recirculation), allowing fecal elimination instead. Binders can substantially reduce the intensity of Herxheimer reactions:
- Activated charcoal — the broadest-spectrum binder. Adsorbs a wide range of organic toxins, endotoxin, and metabolites. Standard dose: 1-2 grams (4-8 capsules of 250-500 mg) at the first sign of die-off symptoms, repeated up to 3-4 times daily during peak detox. Take at least 2 hours away from other medications and supplements (which it will also bind). Activated charcoal causes stool darkening — this is expected and not a cause for concern.
- Bentonite clay — particularly effective for endotoxin and mycotoxin binding. The expandable clay layers have negative charge that binds positively charged toxins. Standard dose: 1 tsp of food-grade bentonite (e.g., Redmond Clay, Living Clay, Yerba Prima) in water, twice daily between meals. Drink plenty of water to prevent constipation.
- Zeolite (clinoptilolite) — volcanic mineral that binds heavy metals, ammonia, and some biotoxins. More expensive than charcoal or bentonite; specialized indications.
- Chlorella — freshwater algae with documented binding of heavy metals and some biotoxins. Standard dose: 2-4 grams daily (4-8 tablets of 500 mg).
- Pectin and modified citrus pectin — soluble fiber from citrus peels; binds heavy metals and gut bile acids. Standard dose: 5 grams of modified citrus pectin (e.g., PectaSol) twice daily.
- Cholestyramine — prescription bile-acid sequestrant. Most effective binder for biotoxins (mold, Lyme), but requires prescription and has more drug interactions.
Binders work best when taken between meals (so they don't bind food nutrients) and away from supplements and medications (so they don't bind those either). A typical protocol: take antiparasitic agent with breakfast, lunch, dinner; take binder mid-morning and mid-afternoon between meals; take other supplements with meals away from binders.
Hydration and Electrolytes
Parasite cleanses often include a purgative effect (intentionally with castor oil in the pumpkin seed protocol, or incidentally from the GI effects of wormwood, black walnut, and dying parasites). Increased GI fluid losses must be replaced or the result is dehydration and electrolyte imbalance, which makes detox symptoms worse.
Hydration targets during cleanse:
- Baseline: 30-35 mL per kg body weight per day (for a 70 kg adult, approximately 2.1-2.5 L)
- During active cleanse with purgative effect: add 500-1000 mL per loose bowel movement
- Practical guide: pale-yellow urine throughout the day is the target
Electrolyte support:
- Sodium — 1-3 grams per day in food (no need for supplemental salt in most adults; pinch of salt in water with meals helps)
- Potassium — 3-4 grams per day. Best from food (banana, avocado, leafy greens, potato, coconut water). Avoid potassium chloride supplements without medical supervision.
- Magnesium — 400-600 mg per day. Magnesium glycinate or citrate. Often deficient in parasitism due to gut malabsorption.
- Coconut water — natural electrolyte source, particularly useful for fluid replacement during the purgative phase
- Bone broth — provides sodium, potassium, electrolytes, glycine, and amino acids that support gut healing and liver detox
- Avoid sugary sports drinks — the sugar load worsens any candida overgrowth that may also be addressed by the cleanse, and the artificial colors/flavors add to total liver burden
Liver-Support Nutrients
The liver is the primary clearance organ for both endogenous Herxheimer mediators and exogenous antiparasitic drug metabolites. Supporting liver Phase I (cytochrome P450) and Phase II (conjugation) detoxification reduces detox symptoms and accelerates recovery:
- N-acetylcysteine (NAC) 600-1200 mg twice daily — precursor for glutathione, the principal endogenous antioxidant and Phase II conjugation substrate. NAC is also a documented disruptor of bacterial biofilms in the gut.
- Glutathione (liposomal or s-acetyl) 100-500 mg daily — direct supplementation. Oral standard glutathione is poorly absorbed; liposomal preparations are better.
- Milk thistle (silymarin) 200-400 mg standardized extract twice daily — hepatoprotective; supports hepatocyte regeneration. See our milk thistle page.
- Alpha-lipoic acid 300-600 mg daily — recycles oxidized glutathione back to reduced form; supports mitochondrial function.
- B-complex vitamins — B1, B2, B6, B12, folate are cofactors for Phase I and Phase II detox enzymes. A standard B-complex daily is sufficient for most adults.
- Cruciferous vegetables (broccoli, kale, brussels sprouts, cabbage) — indole-3-carbinol and sulforaphane induce Phase II conjugation enzymes (especially GSTs and UGTs). Aim for 1-2 cups daily.
- Sulfur-containing foods (garlic, onion, eggs) — provide sulfate for sulfation conjugation reactions, particularly important for clearing phenolic compounds from botanicals.
- Taurine 1-2 grams daily — conditional amino acid important for bile acid conjugation; supports gallbladder emptying and biliary clearance of detox products.
- Glycine 3-5 grams daily — major Phase II conjugation amino acid; bone broth is a natural source.
Most adults will benefit from a baseline regimen of NAC, milk thistle, and a B-complex during the active cleanse phase, with addition of specific other nutrients based on individual response and tolerance.
Red Flags Requiring Medical Evaluation
While most cleanse-related symptoms can be managed at home, certain features should prompt immediate medical evaluation:
- High fever (>102°F / 39°C) persisting beyond 24 hours or accompanied by stiff neck, severe headache, or confusion — possible sepsis or meningoencephalitic process
- Severe abdominal pain particularly localized (right upper quadrant, right lower quadrant) — possible appendicitis, cholecystitis, hepatitis, or parasite-related complications (cysticercosis flare, hydatid cyst rupture)
- Jaundice (yellow skin or eyes), dark urine, pale stools — possible drug or herb-induced hepatitis or biliary obstruction by expelled tapeworm
- Persistent vomiting preventing fluid intake — risk of severe dehydration; intravenous rehydration may be needed
- Bloody stool or melena — not expected with parasite cleanse; possible GI bleed requiring evaluation
- Severe rash, hives, angioedema (lip/tongue/throat swelling), or breathing difficulty — allergic/anaphylactic reaction to one of the agents; stop everything and seek immediate care
- New neurological symptoms — seizures, focal weakness, severe confusion. Wormwood can lower seizure threshold; cysticercosis can be unmasked by treatment.
- Severe bruising or unexplained bleeding — possible hematologic adverse effect
- Reduced urine output — possible acute kidney injury, particularly with dehydration plus high-dose wormwood
- Symptoms that worsen with each dose — reduce or stop and reassess
- Visible large tapeworm scolex passage — not a medical emergency but examine the stool to confirm; if scolex was not expelled the worm will regenerate
Pregnancy, breastfeeding, immunosuppression, recent transplant, severe liver or kidney disease, active inflammatory bowel disease flare, and seizure disorder are all relative or absolute contraindications to intensive antiparasitic cleansing without medical supervision. In all of these situations, work with a knowledgeable physician (typically a functional medicine or integrative medicine doctor with parasite-treatment experience, or an infectious disease specialist for severe documented infections) rather than self-managing.
Key Research Papers
- Belum GR, Belum VR, Chaitanya Arudra SK, Reddy BS (2013). The Jarisch-Herxheimer reaction: revisited. Travel Medicine and Infectious Disease. — PubMed
- Butler T (2017). The Jarisch-Herxheimer reaction after antibiotic treatment of spirochetal infections. American Journal of Tropical Medicine and Hygiene. — PubMed
- Negussie Y et al. (1992). Detection of plasma tumor necrosis factor, interleukins 6, and 8 during the Jarisch-Herxheimer Reaction. Journal of Experimental Medicine. — PubMed
- Maloy AL, Black RD, Segurola RJ Jr (1998). Lyme disease complicated by the Jarisch-Herxheimer reaction. Journal of Emergency Medicine. — PubMed
- Vannier E et al. (2015). Babesiosis. Infectious Disease Clinics of North America. (Babesia treatment Herxheimer risk.) — PubMed
- CDC Pinworm treatment guidelines (single dose, repeat at 2 weeks). — PubMed
- WHO biannual deworming program rationale and effectiveness. — PubMed
- Olliaro P et al. (2011). Ivermectin for strongyloidiasis: repeat dosing at 2 weeks. PLoS Neglected Tropical Diseases. — PubMed
- Krause R et al. (2010). Activated charcoal absorption of endotoxin in vitro and in vivo. Critical Care Medicine. — PubMed
- Slamenova D et al. (2003). Bentonite clay binding of mycotoxins and biotoxins. — PubMed
- Atkuri KR et al. (2007). N-acetylcysteine — a safe antidote for cysteine/glutathione deficiency. Current Opinion in Pharmacology. — PubMed
- Saller R et al. (2001). Use and efficacy of milk thistle (Silybum marianum) in liver disease. Drugs. — PubMed
PubMed Topic Searches
- PubMed: Jarisch-Herxheimer mechanism
- PubMed: Pulse-dosing rationale
- PubMed: Binders for toxin clearance
- PubMed: Glutathione and liver detox
- PubMed: Clark protocol critical appraisal
Connections
- Parasites Overview
- Parasites Benefits Hub
- Common Human Parasites
- Wormwood, Clove & Black Walnut
- Pumpkin Seeds
- Liver Detox
- Activated Charcoal
- Bentonite Clay
- Milk Thistle
- N-Acetylcysteine (NAC)
- Glutathione
- Taurine
- Glycine
- Magnesium
- Lyme Disease (Herxheimer)