Oral Microbiome — Benefits Deep Dive
The oral microbiome is the second most diverse microbial community in the human body after the gut — roughly 700 bacterial species colonize the teeth, gingival sulcus, tongue, palate, cheek mucosa, and saliva. Unlike the gut, which is partitioned from the bloodstream by an intact epithelial barrier, the oral cavity bleeds easily and intimately into the systemic circulation through the highly vascular gingival tissue. This is why oral dysbiosis has measurable downstream effects on cardiovascular disease, Alzheimer's, rheumatoid arthritis, preterm birth, and gut microbiome composition. The four deep-dive pages below explore the most evidence-supported, low-cost, non-pharmaceutical interventions for restoring a healthy oral microbiome — choosing hydroxyapatite over fluoride toothpaste, oil pulling, tongue scraping, and targeted oral probiotic strains.
Deep-Dive Articles
Hydroxyapatite vs Fluoride
Why nano-hydroxyapatite (n-HAp) toothpaste, originally developed by NASA in the 1970s for astronaut tooth-remineralization and refined in Japan as the OTC ingredient "Apagard," is now backed by multiple randomized trials showing non-inferiority or superiority to 1,450 ppm fluoride for caries prevention — without the dose-dependent fluorosis, neurodevelopmental, and thyroid concerns associated with systemic fluoride exposure. The biochemistry of enamel remineralization, the calcium-phosphate vs calcium-fluoride lattice, and the consumer-product landscape.
Oil Pulling
The traditional Ayurvedic practice of swishing 1 tablespoon of cold-pressed coconut, sesame, or sunflower oil in the mouth for 10-20 minutes daily. Randomized trials demonstrate reductions in plaque (Streptococcus mutans counts), gingivitis bleeding scores, and halitosis comparable to chlorhexidine mouthwash — without the chlorhexidine-induced staining or microbiome disruption. The lauric acid in coconut oil and its conversion to monolaurin gives the practice its specific antimicrobial action.
Tongue Scraping
A two-thousand-year-old Ayurvedic practice using a U-shaped copper or stainless steel scraper to mechanically remove the biofilm and volatile sulfur compound (VSC)-producing bacteria from the posterior dorsum of the tongue. Modern studies show 75% reduction in VSC-driven halitosis, measurable improvement in taste perception, and reduced bacterial load reaching the gut on swallowing. Why tongue scraping out-performs tongue brushing.
Oral Probiotic Strains
The three oral-cavity-specific probiotic strains with the strongest randomized-trial evidence: Streptococcus salivarius K12 and M18 for halitosis, strep throat, and otitis media; Lactobacillus reuteri Prodentis (DSM 17938 + ATCC PTA 5289) for gingivitis and periodontitis; and Lactobacillus paracasei for ear infections and dental caries reduction. Why generic gut probiotics do nothing for the mouth, and how lozenge format matters.
Table of Contents
- Deep-Dive Articles
- Why the Oral Microbiome Matters for Whole-Body Health
- The Oral Dysbiosis Cascade
- Research Papers: Hydroxyapatite vs Fluoride
- Research Papers: Oil Pulling
- Research Papers: Tongue Scraping
- Research Papers: Oral Probiotic Strains
- Research Papers: Oral-Systemic Links
- External Authoritative Resources
- Connections
- Featured Videos
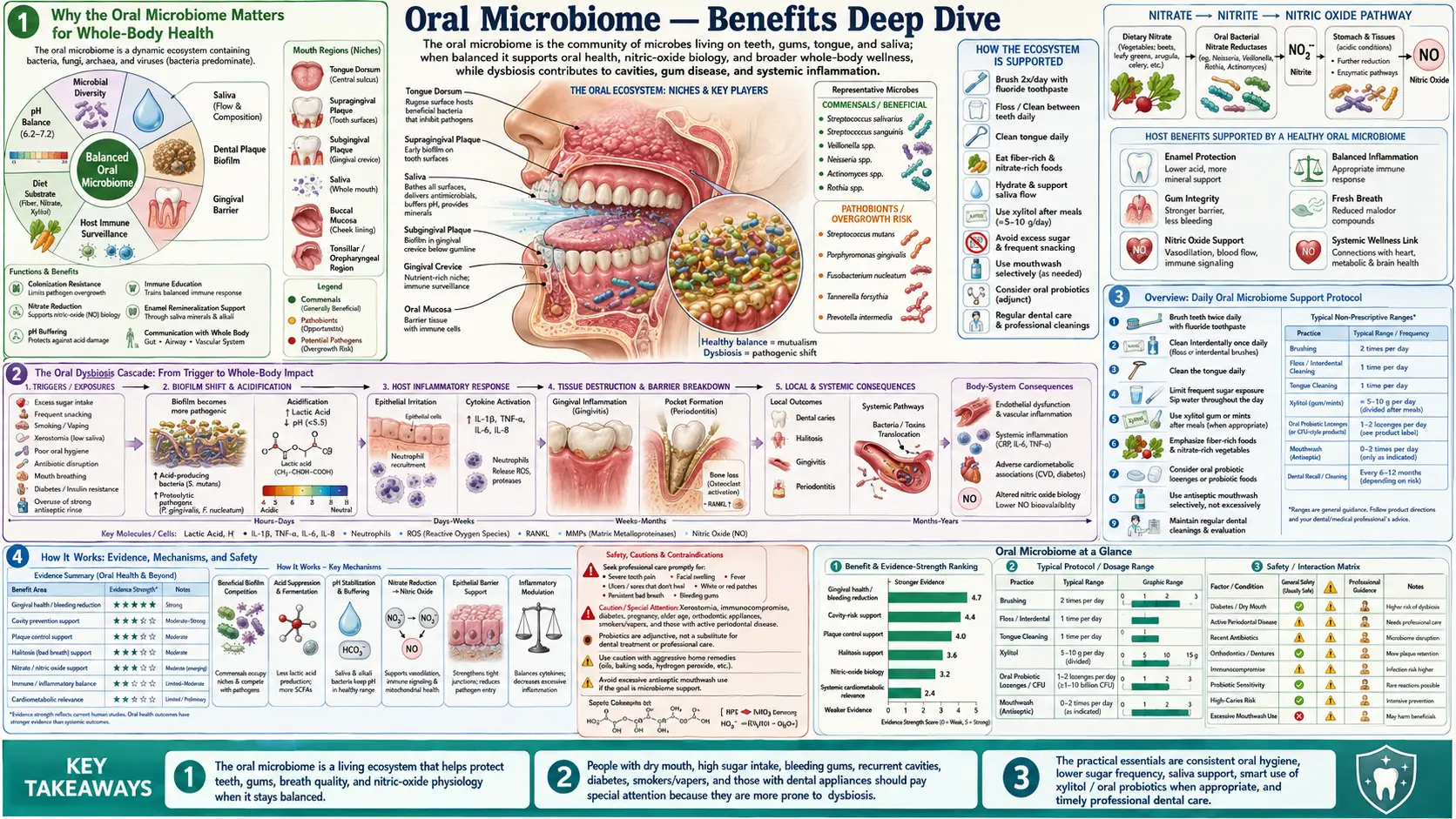
Why the Oral Microbiome Matters for Whole-Body Health
The mouth is unique among microbial habitats. Unlike the colon, where 38 trillion bacteria are partitioned from the bloodstream by a single layer of enterocytes plus a thick mucin layer plus the largest concentration of immune tissue in the body, the gingival sulcus — the V-shaped pocket between tooth and gum — is a fragile junction that bleeds even from gentle flossing in a healthy mouth. In gingivitis or periodontitis, that bleeding becomes constant and the bacterial entry into the bloodstream becomes a continuous low-grade systemic insult.
Three downstream consequences are now established at high evidence levels:
- Cardiovascular disease — Porphyromonas gingivalis, the keystone periodontal pathogen, has been recovered intact from human carotid atheroma plaque by PCR and culture. Periodontitis raises CRP and IL-6 and is independently associated with increased risk of myocardial infarction and stroke even after adjustment for traditional cardiovascular risk factors.
- Alzheimer's disease — P. gingivalis DNA, and the bacterium's characteristic gingipain proteases, have been detected in postmortem Alzheimer brain tissue at higher rates than in cognitively normal controls (Dominy et al. 2019). The hypothesis that chronic oral pathogen translocation drives a fraction of late-life cognitive decline is now being tested in clinical trials of gingipain inhibitors.
- Pregnancy outcomes — Fusobacterium nucleatum, an oral commensal, is recovered from amniotic fluid in cases of preterm birth and stillbirth. Periodontitis is associated with approximately 2-fold increased risk of preterm low-birth-weight delivery, and treatment of periodontitis during pregnancy reduces (but does not eliminate) the risk.
Beyond these systemic associations, the oral microbiome also seeds the gut: most swallowed saliva passes the stomach and contributes oral microbes to the small intestine and colon. Patients with periodontitis have measurably higher gut abundance of oral-origin taxa, including the same F. nucleatum that is now strongly linked to colorectal cancer. A healthy mouth feeds a healthy gut, not just figuratively.
The Oral Dysbiosis Cascade
A healthy oral microbiome is dominated by commensal Streptococcus (especially S. salivarius, S. sanguinis, S. mitis), Veillonella, Actinomyces, Rothia, and Neisseria species that maintain a near-neutral pH at the tooth surface, produce hydrogen peroxide and bacteriocins that suppress pathogenic species, and form a stable biofilm that competitively excludes invasive organisms.
The dysbiosis cascade typically proceeds in three stages:
- Acid stress (caries-favoring dysbiosis) — frequent dietary sugar intake feeds Streptococcus mutans and Lactobacillus species, which produce lactic acid that drops local pH below the critical 5.5 threshold for hydroxyapatite demineralization. Repeated demineralization cycles erode the enamel surface and create the carious lesion. The driver here is dietary sugar frequency, not total sugar — the mouth recovers between exposures, but not if exposures are continuous (sipping a sugary drink all afternoon is far worse than the same amount consumed at one sitting).
- Inflammation-favoring dysbiosis (gingivitis) — plaque accumulation along the gumline drives a local inflammatory response. Aggregatibacter actinomycetemcomitans, Tannerella forsythia, and Treponema denticola begin to displace commensals. Gums become red, swollen, and bleed easily. This stage is fully reversible with mechanical plaque removal.
- Red-complex dysbiosis (periodontitis) — P. gingivalis becomes the keystone organism, suppressing local immune defenses through its gingipain proteases and reshaping the entire microbial community toward the red complex (P. gingivalis + T. forsythia + T. denticola). The periodontal pocket deepens, bone is resorbed around the tooth root, and the tooth eventually loosens. This stage is not fully reversible — once bone is lost, it doesn't come back without surgical intervention.
The four deep-dive interventions below address different stages of this cascade. Hydroxyapatite addresses stage 1 (remineralization of acid-stressed enamel). Oil pulling and tongue scraping address stage 2 (reducing total bacterial burden and biofilm at the gumline and tongue). Oral probiotics address all three stages by restoring competitive exclusion from commensal taxa.
Research Papers: Hydroxyapatite vs Fluoride
- Amaechi BT et al. (2019). Comparative efficacy of a hydroxyapatite and a fluoride toothpaste for prevention and remineralization of dental caries in children. — PubMed
- O'Hagan-Wong K et al. (2022). The use of hydroxyapatite toothpaste to prevent dental caries. Odontology. — PubMed
- Kani T et al. (1989). Effect of apatite-containing dentifrices on dental caries in school children (the original Japanese Apagard trial). — PubMed
- Hannig M, Hannig C (2010). Nanomaterials in preventive dentistry. Nature Nanotechnology. — PubMed
- NASA hydroxyapatite enamel remineralization research history — PubMed
- Najibfard K et al. (2011). Remineralization of early caries by a nano-hydroxyapatite dentifrice. — PubMed
- Bashash M et al. (2017). Prenatal fluoride exposure and cognitive outcomes in children. Environmental Health Perspectives. — PubMed
- Grandjean P (2019). Developmental fluoride neurotoxicity: an updated review. — PubMed
- NTP fluoride monograph 2024 (US National Toxicology Program review) — PubMed
- Esteves-Oliveira M et al. (2017). Caries-preventive effect of anti-erosive and nano-hydroxyapatite-containing toothpastes. — PubMed
Research Papers: Oil Pulling
- Asokan S et al. (2009). Effect of oil pulling on plaque induced gingivitis: a randomized, controlled, triple-blind study. Indian Journal of Dental Research. — PubMed
- Asokan S et al. (2008). Effect of oil pulling on Streptococcus mutans count in plaque and saliva using Dentocult SM Strip mutans test. — PubMed
- Peedikayil FC et al. (2015). Effect of coconut oil in plaque related gingivitis — a preliminary report. Nigerian Medical Journal. — PubMed
- Kim JY et al. (2018). Effects of intensive oral hygiene including coconut oil pulling on oral health — PubMed
- Naseem M et al. (2017). Oil pulling and importance of traditional medicine in oral health maintenance. International Journal of Health Sciences. — PubMed
- Shanbhag VK (2017). Oil pulling for maintaining oral hygiene — a review. Journal of Traditional and Complementary Medicine. — PubMed
- Lauric acid and monolaurin antimicrobial mechanism — PubMed
- Anand TD et al. (2008). Effect of oil-pulling on dental caries causing bacteria. African Journal of Microbiology Research. — PubMed
- Sezgin Y et al. (2019). Comparing the antiplaque and antigingivitis efficacy of coconut oil pulling vs chlorhexidine. — PubMed
- Kaushik M et al. (2016). The effect of coconut oil pulling on Streptococcus mutans count in saliva in comparison with chlorhexidine mouthwash. — PubMed
Research Papers: Tongue Scraping
- Outhouse TL et al. (2006). Tongue scraping for treating halitosis. Cochrane Database of Systematic Reviews. — PubMed
- Pedrazzi V et al. (2004). Tongue-cleaning methods: a comparative clinical trial employing a toothbrush and a tongue scraper. Journal of Periodontology. — PubMed
- Quirynen M et al. (2004). Impact of tongue cleansers on microbial load and taste. Journal of Clinical Periodontology. — PubMed
- Van der Sleen MI et al. (2010). Effectiveness of mechanical tongue cleaning on breath odour and tongue coating: a systematic review. International Journal of Dental Hygiene. — PubMed
- Yaegaki K, Coil JM (2000). Examination, classification, and treatment of halitosis; clinical perspectives. — PubMed
- Volatile sulfur compounds (VSCs) and tongue dorsum bacteria — PubMed
- Solis AC et al. (2011). The use of tongue scraping for reducing volatile sulfur compounds. — PubMed
- Faveri M et al. (2006). A cross-over study on the effect of various therapeutic approaches to morning breath odour. — PubMed
- Tongue coating index and oral hygiene measurement — PubMed
- Roldan S et al. (2003). The effects of a new mouthrinse containing chlorhexidine, cetylpyridinium chloride and zinc lactate on the microflora of oral halitosis patients. — PubMed
Research Papers: Oral Probiotic Strains
- Burton JP et al. (2006). A preliminary study of the effect of probiotic Streptococcus salivarius K12 on oral malodour parameters. Journal of Applied Microbiology. — PubMed
- Di Pierro F et al. (2014). Use of Streptococcus salivarius K12 in the prevention of streptococcal and viral pharyngotonsillitis in children. Drug, Healthcare and Patient Safety. — PubMed
- Burton JP et al. (2013). Influence of the probiotic Streptococcus salivarius strain M18 on indices of dental health in children. — PubMed
- Krasse P et al. (2006). Decreased gum bleeding and reduced gingivitis by the probiotic Lactobacillus reuteri. Swedish Dental Journal. — PubMed
- Vivekananda MR et al. (2010). Effect of the probiotic Lactobacilli reuteri (Prodentis) in the management of periodontal disease. Journal of Oral Microbiology. — PubMed
- Tekce M et al. (2015). Clinical and microbiological effects of probiotic lozenges in the treatment of chronic periodontitis. — PubMed
- Náse L et al. (2001). Effect of long-term consumption of a probiotic bacterium, Lactobacillus rhamnosus GG, in milk on dental caries and caries risk in children. Caries Research. — PubMed
- Wescombe PA et al. (2009). Streptococcus salivarius K12: a colonizing oral probiotic. Future Microbiology. — PubMed
- Power DA et al. (2008). Preliminary investigations of the colonisation of upper respiratory tract tissues of infants using a paediatric formulation of the oral probiotic Streptococcus salivarius K12. — PubMed
- Stensson M et al. (2014). Oral administration of Lactobacillus reuteri during the first year of life reduces caries prevalence in the primary dentition. Caries Research. — PubMed
Research Papers: Oral-Systemic Links
- Dominy SS et al. (2019). Porphyromonas gingivalis in Alzheimer's disease brains: evidence for disease causation and treatment with small-molecule inhibitors. Science Advances. — PubMed
- Haraszthy VI et al. (2000). Identification of periodontal pathogens in atheromatous plaques. Journal of Periodontology. — PubMed
- Lockhart PB et al. (2012). Periodontal disease and atherosclerotic vascular disease: an AHA scientific statement. Circulation. — PubMed
- Han YW et al. (2010). Term stillbirth caused by oral Fusobacterium nucleatum. Obstetrics & Gynecology. — PubMed
- Castellarin M et al. (2012). Fusobacterium nucleatum infection is prevalent in human colorectal carcinoma. Genome Research. — PubMed
- Mougeot JC et al. (2017). Porphyromonas gingivalis is the most abundant species detected in coronary and femoral arteries. Journal of Oral Microbiology. — PubMed
- Olsen I, Yamazaki K (2019). Can oral bacteria affect the microbiome of the gut? Journal of Oral Microbiology. — PubMed
- Bui FQ et al. (2019). Association between periodontal pathogens and systemic disease. Biomedical Journal. — PubMed
- Hajishengallis G (2015). Periodontitis: from microbial immune subversion to systemic inflammation. Nature Reviews Immunology. — PubMed
- Kassebaum NJ et al. (2014). Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. Journal of Dental Research. — PubMed
External Authoritative Resources
- eHOMD — Expanded Human Oral Microbiome Database — the canonical reference for oral microbial taxonomy maintained at the Forsyth Institute / Marine Biological Laboratory
- NIH NIDCR — National Institute of Dental and Craniofacial Research
- American Academy of Periodontology
- FDI World Dental Federation
- PubMed — All research on oral microbiome (~25,000+ papers)
Connections
- Oral Microbiome (Main Page)
- Hydroxyapatite vs Fluoride
- Oil Pulling
- Tongue Scraping
- Oral Probiotic Strains
- All Remedies
- Fluoride (Toxin Profile)
- Alzheimer's Disease
- Atherosclerosis
- Rheumatoid Arthritis
- Colorectal Cancer
- Calcium
- Phosphorus
- Vitamin D3
- Vitamin K2