Oil Pulling — Coconut, Sesame, and Sunflower for Oral Health
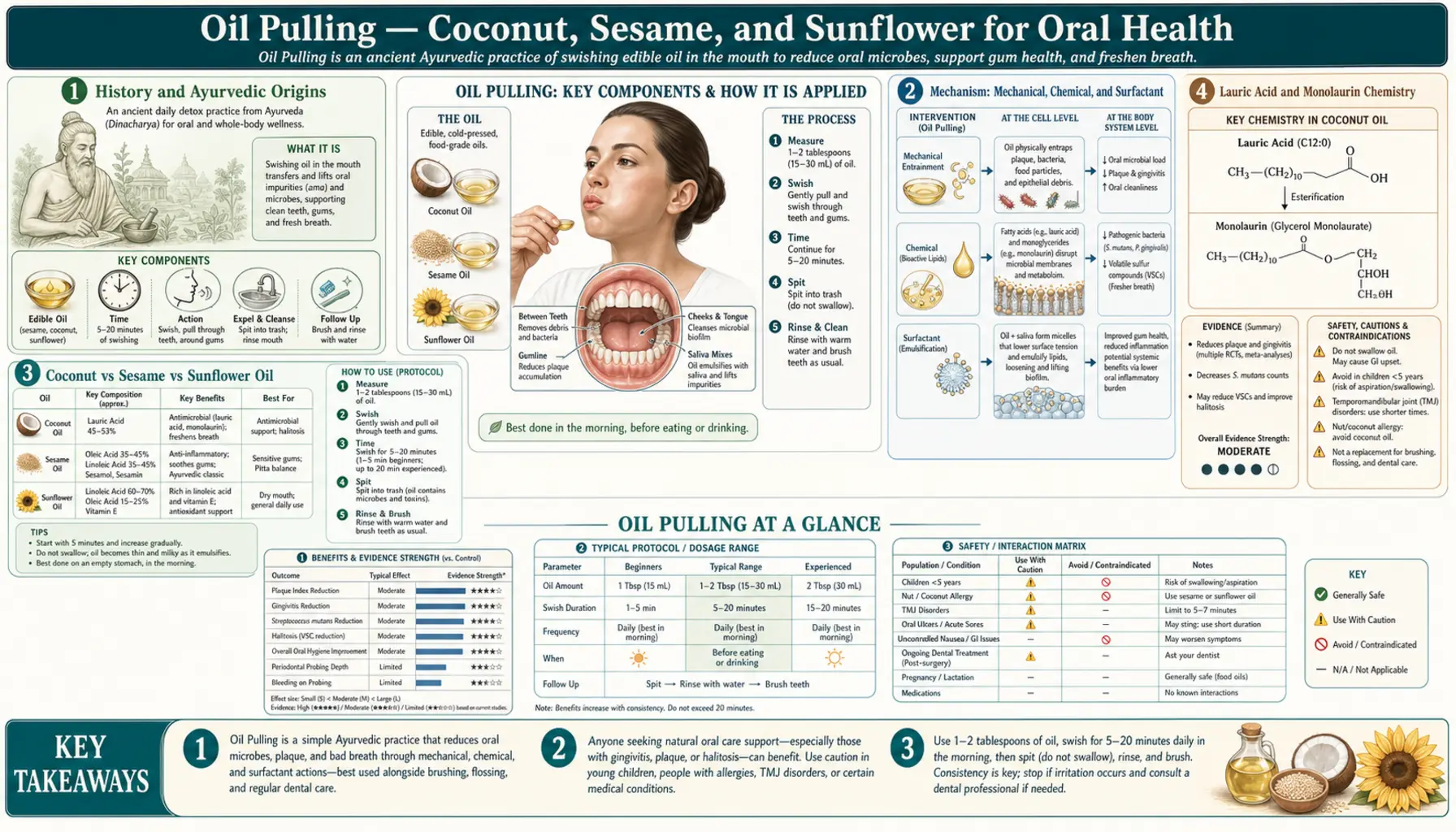
Oil pulling, called kavala or gandusha in classical Ayurvedic texts, is the practice of swishing 1 tablespoon of edible oil — traditionally sesame, increasingly coconut — in the mouth for 10-20 minutes, then spitting it out. The practice was first described in detail in the Charaka Samhita and Sushruta Samhita, Ayurvedic medical texts dating to roughly 500-200 BCE. Modern randomized trials published since 2008 confirm that daily oil pulling reduces plaque, gingivitis bleeding scores, Streptococcus mutans counts, and halitosis to a degree comparable to chlorhexidine mouthwash — without the brown staining, taste alteration, or microbiome disruption associated with prolonged chlorhexidine use. The coconut-oil specific antimicrobial effect is attributable to lauric acid, which is metabolized in the mouth to monolaurin, a potent bacteriocidal and viricidal monoglyceride.
Table of Contents
- History and Ayurvedic Origins
- Mechanism: Mechanical, Chemical, and Surfactant
- Coconut vs Sesame vs Sunflower Oil
- Lauric Acid and Monolaurin Chemistry
- Clinical Trial Evidence
- Why Oil Pulling vs Chlorhexidine
- How to Oil Pull Properly
- Cautions and Common Mistakes
- Key Research Papers
- Connections
- Featured Videos
History and Ayurvedic Origins
Oil pulling is documented in two of the foundational texts of Ayurveda. The Charaka Samhita (compiled approximately 200 BCE - 200 CE, drawing on much older oral tradition) describes kavala as a daily oral hygiene practice, recommended particularly for the strengthening of teeth, jaws, and voice, and for the prevention of dryness in the mouth. The Sushruta Samhita, a contemporaneous surgical text, expands the recommendations with prescriptions for medicated oils — sesame oil infused with neem, triphala, licorice, or other herbs, depending on the patient's constitution and the clinical indication.
Two distinct techniques are described in the classical texts:
- Kavala graha — using a smaller amount of liquid (less than fills the mouth), held in the mouth and moved about for several minutes, then spit out. This is closer to what would be called a "swish" in English.
- Gandusha — filling the mouth completely with the medicated oil, holding it static for 3-5 minutes, then spitting it out. This was the more formal therapeutic procedure, prescribed for specific conditions.
Modern oil pulling as commonly practiced is closer to kavala graha — 1 tablespoon of oil, actively swished for 10-20 minutes, then spit out. The extended duration of modern practice (vs the 3-5 minutes of classical gandusha) is a 20th-century elaboration popularized by Dr. F. Karach in the early 1990s, whose Ukrainian-origin oil-pulling protocol gave the practice its current global form.
The practice fell out of routine Western medical view for most of the 20th century, then re-entered Western awareness in the 2000s through two channels: the Ayurvedic revival in India and the broader natural-products movement, and a sequence of randomized clinical trials beginning with Asokan's work at Meenakshi Ammal Dental College in Chennai starting around 2008.
Mechanism: Mechanical, Chemical, and Surfactant
Three mechanisms are plausibly operating during a 10-20 minute oil-pulling session, and likely all three contribute to the observed clinical effects:
- Mechanical removal — the act of vigorously swishing oil throughout the oral cavity, pulling it back and forth between teeth, and drawing it through interproximal spaces by negative pressure (which is what "pulling" refers to) physically dislodges food debris, plaque, and loosely-adherent biofilm. This mechanical action alone, repeated for 10-20 minutes, removes more material than a brief 30-second rinse.
- Surfactant emulsification — oils are amphipathic, with hydrophobic fatty acid tails and hydrophilic glycerol heads. During the prolonged swishing, the oil emulsifies with saliva, forming a milky white-yellow foam that is much more effective at solubilizing and lifting bacterial cell membranes (which are themselves lipid bilayers) than plain water. By the end of a 15-minute session, the spit-out liquid is dramatically lighter in color and noticeably foamy — this is the emulsion containing dispersed bacteria and biofilm material.
- Chemical antimicrobial action — specific fatty acids in the oils, particularly medium-chain saturated fatty acids like lauric acid (12 carbons) in coconut oil, have direct antibacterial action. Lauric acid integrates into bacterial cell membranes and disrupts their structural integrity. The effect is concentration-dependent and dramatically enhanced when lauric acid is partially hydrolyzed to monolaurin, the corresponding monoglyceride, by salivary lipase during the session.
The relative contribution of each mechanism is debated. The Asokan trials showed that oil pulling produces dramatic effects on S. mutans counts and gingivitis even when the oil is sesame (low lauric acid content) — suggesting that mechanical and surfactant effects are the dominant action. The Peedikayil and Kaushik trials showed that coconut oil specifically produces faster onset of effect and lower S. mutans counts than other oils, suggesting that lauric acid does provide additional benefit on top of the mechanical and surfactant effects.
For the practical patient, the choice of oil matters but it is not a deal-breaker. Any of the three traditional oils (sesame, coconut, sunflower) will provide most of the benefit; coconut likely provides somewhat more.
Coconut vs Sesame vs Sunflower Oil
The three traditional oils used for pulling, with their relevant fatty acid profiles:
- Coconut oil — approximately 50% lauric acid (C12), 18% myristic acid (C14), 8% caprylic acid (C8), 7% capric acid (C10), plus smaller fractions of palmitic, oleic, and others. Coconut oil is unique among edible oils in its high lauric acid content. Solid at room temperature below ~76°F (24°C); melts in the mouth within seconds of being introduced. Mild, pleasant flavor that most users find acceptable.
- Sesame oil (the traditional Ayurvedic choice) — approximately 41% linoleic acid (C18:2 omega-6), 39% oleic acid (C18:1 omega-9), 9% palmitic acid (C16), and minor stearic acid. Negligible lauric acid. Contains sesame-specific lignans (sesamin, sesamolin) which have antioxidant activity that may contribute to anti-inflammatory effects on gingival tissue. Stronger, more distinctive flavor than coconut.
- Sunflower oil — approximately 60% linoleic acid, 25% oleic acid, 5% palmitic, 4% stearic. Largely flavor-neutral. Used in some traditional preparations as an alternative to sesame when sesame is unavailable.
Other oils sometimes used in modern practice:
- MCT oil — fractionated coconut oil with predominantly C8 and C10 fatty acids, with lauric acid removed. Liquid at room temperature. Provides the surfactant effect of coconut oil but without the specific lauric acid/monolaurin antimicrobial action — not recommended as a substitute for whole virgin coconut oil for this purpose.
- Olive oil — predominantly oleic acid. Some users prefer it; works on mechanical and surfactant effects but lacks specific antimicrobial fatty acid content.
- Ghee (clarified butter) — mentioned in some Ayurvedic preparations. Contains butyric acid which is anti-inflammatory but the lauric acid content is much lower than coconut. Some users find the flavor unpleasant for oral use.
Recommendation: for most users, virgin (unrefined) coconut oil is the optimal choice based on the combination of clinical trial evidence, fatty acid profile, mild flavor, and wide availability. The 2016 Kaushik comparison trial showed coconut oil reduced S. mutans counts equivalently to chlorhexidine after 30 days. For users who genuinely dislike the coconut flavor, sesame oil is the traditional alternative with strong clinical trial support (Asokan's body of work used sesame).
Lauric Acid and Monolaurin Chemistry
Lauric acid (dodecanoic acid, C12:0) is a medium-chain saturated fatty acid present at approximately 50% concentration in coconut oil — an unusually high concentration compared to most edible oils. In nature, the only other significant dietary source is human breast milk, where lauric acid concentration of 5-10% of fatty acid content contributes to the antimicrobial protection that breast milk provides to nursing infants.
Lauric acid itself has modest direct antibacterial activity. What it does much more potently is convert, in the presence of lipase enzymes, to the corresponding 1-monoglyceride: monolaurin (glycerol monolaurate, GML). Monolaurin is dramatically more antimicrobial than lauric acid itself, with documented activity against:
- Streptococcus mutans, S. sanguinis, and other oral streptococci
- Staphylococcus aureus (including MRSA)
- Candida albicans
- Lipid-enveloped viruses (influenza, herpes simplex)
- Various gram-positive pathogens
The mechanism is membrane disruption — monolaurin's amphipathic structure allows it to insert into lipid bilayers, where its presence destabilizes membrane integrity, causes leakage of intracellular contents, and ultimately kills the cell. The effect is concentration-dependent and is most potent against gram-positive bacteria (which have a simpler outer wall structure than gram-negatives).
During oil pulling, salivary lipase begins hydrolyzing the triglycerides in coconut oil within minutes of mouth contact. By the end of a 15-minute session, a fraction of the coconut oil's lauric acid has been converted to free lauric acid and then to monolaurin in situ. This is the chemical foundation for the apparently superior antibacterial effect of coconut oil pulling vs other oils.
Monolaurin is also available as an oral supplement (typically 600-1,800 mg/day in capsule form) for systemic antimicrobial use against chronic infections, biofilm-driven conditions, and certain viral reactivations. The oral pulling approach delivers monolaurin directly to the oral microbiome rather than relying on systemic distribution after intestinal absorption.
Clinical Trial Evidence
The modern clinical trial base for oil pulling is concentrated in publications from Indian dental schools (predominantly between 2008 and 2018) along with a smaller body of work from Saudi Arabia and Turkey. Key findings:
- Asokan 2008 — randomized 20 adolescent subjects to daily sesame oil pulling for 10 minutes vs no intervention. After 2 weeks, the oil-pulling group showed significant reduction in Streptococcus mutans counts in both plaque and saliva as measured by the Dentocult SM Strip mutans test. This was the first modern controlled trial.
- Asokan 2009 — triple-blind RCT of 20 adolescents, sesame oil pulling vs chlorhexidine mouthwash for plaque-induced gingivitis. After 45 days, both interventions produced statistically significant and comparable reductions in plaque index and modified gingival index.
- Anand 2008 — in-vitro and in-vivo study of sesame oil pulling effects on dental caries causing bacteria; demonstrated significant reductions in total bacterial count.
- Peedikayil 2015 — coconut oil pulling for plaque-related gingivitis in 60 adolescents over 30 days. Statistically significant reduction in plaque and gingival index scores observed from day 7 onwards.
- Kaushik 2016 — head-to-head comparison of coconut oil pulling vs chlorhexidine vs distilled water in 45 subjects over 14 days. Coconut oil pulling and chlorhexidine produced statistically equivalent reductions in Streptococcus mutans counts in saliva, both significantly better than water control.
- Sezgin 2019 — comparison of coconut oil pulling vs chlorhexidine for antiplaque and antigingivitis efficacy. Both interventions reduced plaque and gingival indices, with no statistically significant difference between groups.
- Kim 2018 — intensive oral hygiene including coconut oil pulling improved multiple oral health parameters including halitosis measured by volatile sulfur compound concentrations.
- Naseem 2017 review — pooled the available evidence and concluded that oil pulling has scientifically demonstrable benefits for oral health when combined with standard brushing and flossing.
The trial base has several limitations. Most trials are small (n=20-60), of short duration (2-6 weeks), and conducted in single centers. There is no large multi-center trial of the magnitude that would be needed for FDA recognition as a therapeutic intervention. The trials are also predominantly published in regional dental journals rather than top-tier general medical journals. That said, the consistency of results across multiple independent groups, with reasonable methodology (randomization, blinding where feasible, validated endpoints), supports the conclusion that oil pulling produces meaningful clinical effects.
Why Oil Pulling vs Chlorhexidine
Chlorhexidine gluconate (0.12% or 0.20%) is the gold-standard antimicrobial mouthwash in dental practice. It is broadly bactericidal, has well-documented efficacy for gingivitis and pre/post-surgical use, and is widely prescribed. Why might someone prefer oil pulling?
- Tooth staining — chlorhexidine binds to dental pellicle and creates brown-yellow staining of teeth, tongue, dental restorations, and dentures. The staining is reversible with cessation and professional cleaning, but is cosmetically unacceptable to many patients for long-term use. Oil pulling does not stain.
- Taste alteration — chlorhexidine commonly produces a metallic or bitter taste alteration that can persist for hours. The effect is reversible but unpleasant. Oil pulling does not alter taste perception.
- Microbiome disruption — chlorhexidine kills broadly, including beneficial commensals. Prolonged use can disrupt the oral microbiome in ways that may have downstream effects. Some recent research has even raised concerns about chlorhexidine altering nitrate-reducing oral commensals (which produce nitric oxide systemically and contribute to blood pressure regulation). Oil pulling appears to selectively reduce pathogenic species more than commensals, though this is less well characterized.
- Cost and access — chlorhexidine is prescription-only in many jurisdictions and costs $10-15 per bottle. A jar of organic virgin coconut oil costs $5-10 and lasts months at 1 tablespoon per day.
- No allergy risk — chlorhexidine allergy, while uncommon, can be severe and includes anaphylactic reactions in rare cases. Coconut oil allergy is negligible (coconut is in the drupe family, not a true nut, and is generally tolerated even by tree-nut-allergic patients).
Chlorhexidine retains advantages for specific short-term clinical situations (post-surgical mouthrinse, acute necrotizing ulcerative gingivitis, immune-compromised patients with severe oral infections) where rapid broad-spectrum action is needed. For routine daily oral hygiene, oil pulling provides comparable benefit with a much more favorable side-effect profile.
How to Oil Pull Properly
The standard modern protocol:
- When — first thing in the morning, before brushing and before eating or drinking. The overnight bacterial load is highest at this point. Some practitioners do a second session before bed, but morning is the higher-yield slot.
- How much — 1 tablespoon (~15 mL) of unrefined virgin coconut oil. If the oil is solid (below ~76°F), it will liquefy in the mouth within 30 seconds. Do not heat the oil first — mouth-temperature melting is fine.
- How long — 10-20 minutes, depending on personal tolerance. Most clinical trial protocols used 15 minutes. There is a reasonable dose-response in trial data — longer sessions produce more bacterial reduction, with diminishing returns beyond 20 minutes. Start with 5-10 minutes and work up to 15-20 over the first week.
- What to do during — swish, pull, and draw the oil between teeth, around the gumline, and through interproximal spaces. The oil will progressively whiten and foam as it emulsifies with saliva. Do not gargle (the throat tissue is more permeable than oral mucosa and the released bacteria-laden emulsion should not enter the airways).
- What to do if your mouth fills with saliva — spit out a small amount and continue. Saliva flow is a normal response to oil in the mouth and adds to the volume.
- Where to spit — into the trash, never down the sink. Coconut oil solidifies as it cools and will clog drains rapidly. After spitting, rinse mouth with warm water several times.
- Then — brush teeth normally with hydroxyapatite or fluoride toothpaste. Oil pulling does not replace brushing; it is a pre-brush adjunct that reduces overall bacterial load.
The first few sessions are challenging for most users — the gag reflex from a mouth full of oil, jaw fatigue from continuous swishing for 15 minutes, and the unfamiliar sensation can be off-putting. Most users adapt within a week and the practice becomes a comfortable morning routine that fits while showering, getting dressed, or reading.
Cautions and Common Mistakes
- Do not swallow the oil — after 10-20 minutes of swishing, the oil contains substantial quantities of dislodged bacteria, biofilm material, food debris, and bacterial endotoxins. Swallowing it transfers this pathogen-loaded material to the gut.
- Do not gargle — for the same reason. The bacteria-laden emulsion should not contact the throat or be aspirated.
- Do not heat the oil first — cold-pressed virgin coconut oil's thermal history affects its lauric acid bioavailability. Use it at room temperature; mouth heat melts it within seconds.
- Do not use as a replacement for brushing and flossing — oil pulling is an adjunct, not a substitute. The mechanical action of bristles is required for thorough plaque removal.
- Do not expect overnight results — the clinical trial data show measurable effects beginning at day 7-14 and consolidating over weeks. Halitosis improvements may be felt within the first few days; gingivitis bleeding scores take longer.
- Cautions in specific populations:
- Pregnant women — safe; coconut oil is dietary and the practice itself is non-systemic.
- Young children — not recommended for children too young to reliably spit out the oil rather than swallow.
- Coconut allergy — rare but check for personal allergy before first use.
- Aspiration risk — patients with significant swallowing dysfunction (advanced Parkinson's, stroke with dysphagia) should not oil pull due to aspiration risk.
- Do not expect non-oral effects — popular online claims that oil pulling whitens teeth dramatically, cures TMJ, lowers blood pressure, or "detoxifies" the body are not supported by clinical evidence. The validated effects are local oral microbiome and gingival health benefits.
- Drain disposal — never spit oil down the sink. Coconut oil clogs plumbing reliably. Spit into the trash bin or a disposable cup, then rinse the mouth at the sink.
Key Research Papers
- Asokan S, Emmadi P, Chamundeswari R (2009). Effect of oil pulling on plaque induced gingivitis: a randomized, controlled, triple-blind study. Indian Journal of Dental Research, 20(1):47-51. — PubMed
- Asokan S, Rathan J, Muthu MS et al. (2008). Effect of oil pulling on Streptococcus mutans count in plaque and saliva using Dentocult SM Strip mutans test. Journal of Indian Society of Pedodontics and Preventive Dentistry, 26(1):12-7. — PubMed
- Anand TD, Pothiraj C, Gopinath RM, Kayalvizhi B (2008). Effect of oil-pulling on dental caries causing bacteria. African Journal of Microbiology Research, 2:063-066. — PubMed
- Peedikayil FC, Sreenivasan P, Narayanan A (2015). Effect of coconut oil in plaque related gingivitis — a preliminary report. Nigerian Medical Journal, 56(2):143-7. — PubMed
- Kaushik M, Reddy P, Sharma R et al. (2016). The effect of coconut oil pulling on Streptococcus mutans count in saliva in comparison with chlorhexidine mouthwash. Journal of Contemporary Dental Practice, 17(1):38-41. — PubMed
- Sezgin Y, Memis Ozgul B, Alptekin NO (2019). Efficacy of oil pulling therapy with coconut oil on four-day supragingival plaque growth. Journal of Indian Society of Periodontology. — PubMed
- Naseem M, Khiyani MF, Nauman H et al. (2017). Oil pulling and importance of traditional medicine in oral health maintenance. International Journal of Health Sciences, 11(4):65-70. — PubMed
- Shanbhag VK (2017). Oil pulling for maintaining oral hygiene — a review. Journal of Traditional and Complementary Medicine, 7(1):106-109. — PubMed
- Kim JY, Jung HJ, Yu DJ, Choi YH (2018). Effects of intensive oral hygiene care including coconut oil pulling on oral health and quality of life. — PubMed
- Kapoor U, Sharma G, Juneja M, Nagpal A (2017). Halitosis: current concepts on etiology, diagnosis and management. European Journal of Dentistry, 10(2):292-300. — PubMed
- Bergsson G, Arnfinnsson J, Steingrimsson O, Thormar H (2001). In vitro killing of Candida albicans by fatty acids and monoglycerides. Antimicrobial Agents and Chemotherapy, 45(11):3209-12. — PubMed
- Schlievert PM, Peterson ML (2012). Glycerol monolaurate antibacterial activity in broth and biofilm cultures. PLoS ONE, 7(7):e40350. — PubMed
PubMed Topic Searches
- PubMed: Oil pulling and S. mutans
- PubMed: Coconut oil + lauric acid + oral health
- PubMed: Oil pulling vs chlorhexidine
- PubMed: Monolaurin antimicrobial mechanism
- PubMed: Sesame oil Ayurveda kavala gandusha
Connections
- Oral Microbiome (Main Page)
- Oral Microbiome Benefits Hub
- Hydroxyapatite vs Fluoride
- Tongue Scraping
- Oral Probiotic Strains
- Sesame Seeds
- Ayurveda
- Monolaurin
- Gingivitis
- Periodontitis
- Halitosis
- Candida
- Oil Pulling — the standalone remedy page on the practice, covering oil choice, swishing technique, and the wider claims made for it.
- All Remedies