Oral Probiotic Strains — S. salivarius K12, M18, and L. reuteri Prodentis
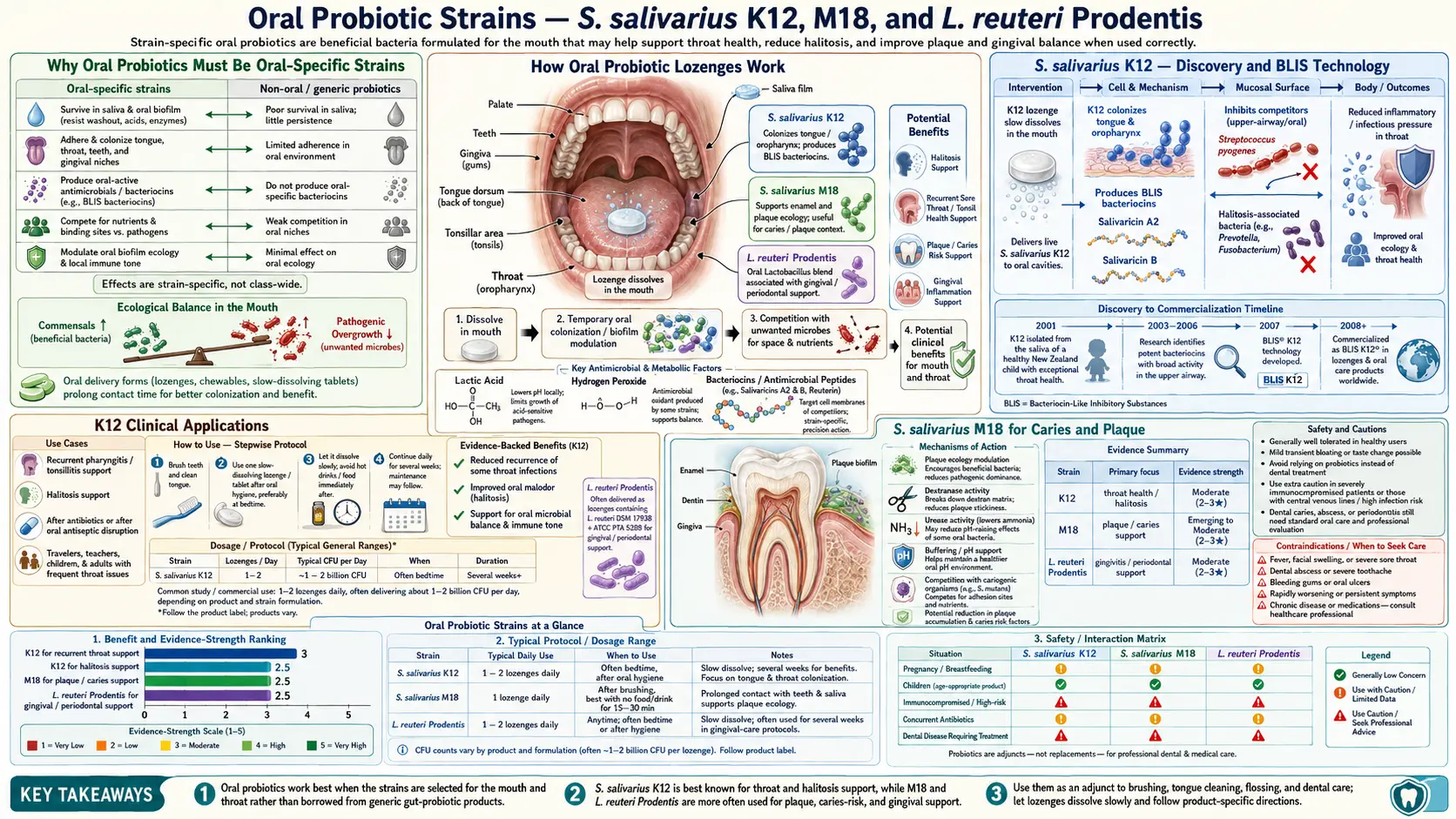
Most probiotic products on the market contain Lactobacillus and Bifidobacterium strains evolved for the lower gastrointestinal tract — they do nothing for the oral cavity because they cannot colonize the very different microenvironment of the mouth. Three specific probiotic strains, evolved or selected to colonize the oral cavity itself, have strong randomized-trial evidence for targeted oral indications: Streptococcus salivarius K12 for halitosis, recurrent streptococcal pharyngitis, and otitis media; S. salivarius M18 (also marketed as BLIS M18) for caries reduction and gingival health; and Lactobacillus reuteri Prodentis (the combination of DSM 17938 + ATCC PTA 5289) for gingivitis and periodontitis. All three are delivered in lozenge format, dissolved slowly in the mouth as the last thing before bed, so that the colonizing organisms can adhere to the oral epithelium overnight without being washed away by eating or drinking.
Table of Contents
- Why Oral Probiotics Must Be Oral-Specific Strains
- S. salivarius K12 — Discovery and BLIS Technology
- K12 Clinical Applications
- S. salivarius M18 for Caries and Plaque
- L. reuteri Prodentis for Periodontitis
- L. paracasei and Otitis Media Adjunct
- Why Lozenge Format Matters
- Practical Protocols by Indication
- Cautions and Limitations
- Key Research Papers
- Connections
- Featured Videos
Why Oral Probiotics Must Be Oral-Specific Strains
A common consumer misconception is that any probiotic supplement will help with oral health. It will not. The oral cavity and the lower gastrointestinal tract are radically different microbial habitats:
- Oxygen — the mouth is aerobic to microaerophilic. The colon is strictly anaerobic. Strains that thrive in the colon (most Bifidobacterium, most Lactobacillus) are oxygen-sensitive and cannot colonize the mouth.
- pH — saliva pH is near-neutral (6.5-7.5), buffered tightly. Colon contents are also near-neutral but the stomach acid bath in between (pH 1-3) selects for acid-tolerant strains. Strains evolved to survive stomach transit may not be the strains best at oral colonization.
- Surfaces and biofilm — the mouth provides hard mineralized surfaces (teeth), keratinized mucosa (palate), and non-keratinized mucosa (cheek, tongue, floor of mouth). The colon provides only mucus-coated soft epithelium. Bacterial adhesion mechanisms are surface-specific.
- Diet — the oral microbiome encounters all food and drink in original form, including sugars, acids, alcohol, and antimicrobial spices. The colon receives only what survives upper digestion.
Strains that work in the oral cavity must (a) tolerate the local oxygen and pH conditions, (b) adhere to oral surfaces against the continuous washing by saliva swallowing, and (c) actively suppress competing pathogenic species through bacteriocin production or competitive exclusion. Only a small subset of probiotic strains meet all three requirements. The four that have the strongest evidence base are listed in this article.
Strains specifically NOT useful for oral health (despite being good gut probiotics):
- Most Bifidobacterium species — obligate anaerobes, cannot colonize mouth
- Lactobacillus acidophilus — can transiently inhabit mouth but does not colonize
- Lactobacillus rhamnosus GG (LGG) — minor effects on caries in milk-delivery studies but does not colonize the oral cavity
- Saccharomyces boulardii — a yeast probiotic for gut; no oral application
- Most "broad-spectrum" 10-strain probiotic blends marketed for general gut health
S. salivarius K12 — Discovery and BLIS Technology
Streptococcus salivarius is the most abundant bacterial species in the healthy human oral cavity. It colonizes the tongue, palate, throat, and saliva from the first 24 hours of life and remains a dominant member of the oral commensal community throughout the lifespan. Within the species, individual strains differ dramatically in their ability to produce inhibitory substances against pathogenic species.
The K12 strain was isolated in 1999 by Professor John Tagg at the University of Otago in New Zealand from the throat of a healthy child who had never experienced a strep throat infection — an unusually rare phenotype. Tagg's research group hypothesized that this child's natural resistance to strep throat was due to colonization with a particularly potent strain of S. salivarius that out-competed Streptococcus pyogenes (group A strep) by producing bacteriocins — protein antibiotics — that selectively killed the pathogen while leaving commensals intact.
This bacteriocin production capability was named BLIS (Bacteriocin-Like Inhibitory Substance) technology. K12 produces two characterized bacteriocins:
- Salivaricin A2 — active against multiple oral and pharyngeal pathogens
- Salivaricin B — active against Streptococcus pyogenes specifically
The combination of these two lantibiotics provides K12 with broad inhibitory activity against:
- Streptococcus pyogenes (strep throat)
- Volatile-sulfur-compound producing bacteria (halitosis)
- Some Moraxella catarrhalis strains (otitis media)
- Some Streptococcus pneumoniae strains
K12 is the most-studied oral probiotic strain. It is commercialized globally by BLIS Technologies (New Zealand) and licensed to multiple consumer brands including Bactoblis, ProBioRA, Now Foods OralBiotic, Hyperbiotics PRO-Dental, and others. Cost is moderate ($20-30 per month) due to the need for specialized cold-chain manufacturing and lozenge formulation.
K12 Clinical Applications
The randomized-trial evidence base for K12 covers three main indications:
- Halitosis — Burton 2006 in Journal of Applied Microbiology randomized 23 subjects with elevated VSCs to K12 lozenges vs placebo for 1 week. The K12 group showed measurable reduction in VSCs and self-reported halitosis. The mechanism is competitive exclusion of the gram-negative anaerobes (predominantly tongue-coating bacteria, see Tongue Scraping) that produce H₂S and methyl mercaptan.
- Recurrent streptococcal pharyngitis — Di Pierro 2014 randomized 130 children with documented recurrent strep throat to K12 lozenges for 90 days vs placebo. The K12 group experienced approximately 90% reduction in strep throat episodes vs the prior year, and 80% reduction in viral pharyngitis episodes (an unexpected secondary finding suggesting K12 also produces general antiviral or anti-inflammatory benefit in the throat).
- Otitis media (middle ear infections) — Di Pierro 2015 in Drug, Healthcare and Patient Safety showed that K12 supplementation reduced the incidence of acute otitis media episodes in otitis-prone children. The proposed mechanism is K12 colonization of the nasopharynx and Eustachian tube outlet, where it competitively excludes the bacterial pathogens responsible for otitis media.
- Adjunct in dental caries — smaller body of evidence supports K12 colonization producing modest reductions in Streptococcus mutans abundance, though M18 is the better-studied salivarius strain for this indication.
The Wescombe 2009 review in Future Microbiology remains the most comprehensive summary of K12's mechanism and clinical applications, written by members of the original BLIS Technologies / University of Otago group.
The key practical point: K12 actually colonizes the throat and oral cavity, persisting for weeks to months after a course of supplementation, rather than producing only a transient effect during the supplementation period. Most users following the standard protocol (1 lozenge per night for 30-90 days) achieve persistent colonization that continues to produce benefits long after stopping supplementation.
S. salivarius M18 for Caries and Plaque
The M18 strain (also marketed as BLIS M18) was isolated by the same Tagg / BLIS group at Otago through systematic screening of S. salivarius isolates for those producing salivaricins active specifically against Streptococcus mutans, the principal cariogenic organism. M18 produces salivaricins A, B, M, 9, and MPS, plus the enzyme dextranase, which breaks down the extracellular polysaccharide matrix produced by S. mutans as it forms cariogenic plaque biofilm.
The principal randomized trial is Burton 2013 in Journal of Medical Microbiology. Researchers randomized 100 schoolchildren aged 5-10 to M18 lozenges twice daily for 3 months vs placebo. After 3 months and at 6-month follow-up, the M18 group showed:
- Significantly lower plaque scores
- Lower gingival inflammation indices
- Reduced S. mutans counts in saliva
- Persistence of M18 colonization in most subjects 3 months after supplementation ended
A subsequent Italian trial (Di Pierro 2015) in adults showed similar benefit for plaque and gingivitis indices.
M18 is well-suited to combination with K12 in a single lozenge format, and several commercial products include both strains in the same lozenge (e.g., ProBio M18+K12 combinations). For users primarily concerned with caries prevention and gingival health, M18 is the priority strain; for users primarily concerned with halitosis, throat infections, or otitis media, K12 is the priority strain; for those wanting general oral microbiome optimization, the combination product is reasonable.
L. reuteri Prodentis for Periodontitis
Lactobacillus reuteri Prodentis is a specific commercial combination of two characterized strains: L. reuteri DSM 17938 and L. reuteri ATCC PTA 5289. These two strains were selected from a screening program by BioGaia AB (Sweden) for their adhesion to oral epithelial cells, suppression of periodontal pathogens, and production of reuterin, a broad-spectrum antimicrobial compound that L. reuteri produces from glycerol metabolism.
Unlike most Lactobacillus species, L. reuteri Prodentis does adhere to oral surfaces and can colonize transiently, though it does not appear to achieve the long-term colonization that K12 and M18 do. Effects depend on continued daily supplementation.
The pivotal randomized trial is Krasse 2006 in Swedish Dental Journal: 59 patients with moderate to severe gingivitis were randomized to L. reuteri Prodentis chewing gum or lozenges vs placebo for 2 weeks. The Prodentis group showed statistically significant reduction in gingival inflammation, bleeding on probing, and plaque indices.
The subsequent Vivekananda 2010 trial extended the evidence to periodontitis specifically: 30 chronic periodontitis patients were randomized to L. reuteri Prodentis lozenges vs placebo, with and without scaling and root planing. The Prodentis arm showed greater reductions in probing pocket depth, clinical attachment level, and bleeding on probing — both as monotherapy and as adjunct to scaling.
The Tekce 2015 trial confirmed Prodentis as a useful adjunct to scaling and root planing for chronic periodontitis, with clinical and microbiological improvements maintained at 1 year post-treatment.
L. reuteri Prodentis is commercialized as BioGaia Prodentis lozenges and similar products. Typical dose: 1 lozenge twice daily, dissolved slowly in the mouth, for 4-12 weeks. Often combined with periodontal scaling and root planing for synergistic benefit. Cost: $25-35 per month.
For patients with active periodontitis, this is the highest-evidence probiotic adjunct currently available. It does not replace periodontal scaling, periodontal surgery where indicated, or treatment of contributing factors (smoking cessation, diabetes management). It augments those interventions.
L. paracasei and Otitis Media Adjunct
A fourth strain worth mentioning is Lactobacillus paracasei, specifically strains evaluated as nasal sprays or oral lozenges for prevention of acute otitis media in otitis-prone children. The evidence base is smaller than for K12, but the Roos 2001 trial showed reduced rates of acute otitis media recurrence in children receiving L. paracasei nasal spray after acute infection.
Some commercial otitis-prevention products combine K12, M18, and L. paracasei into single lozenges or sprays, with the rationale that the three strains cover overlapping but somewhat different microbial niches in the upper respiratory tract / nasopharynx / oral cavity.
For the most evidence-based recommendation on otitis-media-prone children, the K12 protocol from Di Pierro's work is the principal intervention, with L. paracasei as a secondary consideration if K12 alone does not produce adequate reduction in episodes.
Why Lozenge Format Matters
The format in which an oral probiotic is delivered matters more than for gut probiotics. The key requirements:
- Slow dissolution in the mouth — the bacteria need extended contact time with oral surfaces to adhere and colonize. A swallowed capsule delivers the organisms directly to the stomach (where gastric acid kills most of them) and bypasses the oral cavity entirely — defeating the purpose. A lozenge that dissolves slowly over 5-10 minutes provides extended exposure of oral surfaces to high concentrations of viable organisms.
- No subsequent eating or drinking — immediately after lozenge dissolution, eating or drinking will mechanically wash unattached organisms away. The lozenge should be the last thing in the mouth, with no food, drink, brushing, mouthwash, or oil pulling for at least 30 minutes afterward — ideally taken last thing before sleep so the entire overnight period is available for colonization.
- Adequate dose — the standard K12 dose is 1 billion CFU per lozenge; M18 also 1 billion CFU; L. reuteri Prodentis ~200 million CFU per lozenge. Sub-dose products are common in the consumer market — check the label.
- Viable organisms — probiotic lozenges have a finite shelf life and viability declines especially in heat. Refrigerated storage extends shelf life. Look for products with guaranteed CFU at expiration (not just at manufacture).
- Sugar-free or xylitol-sweetened — lozenges sweetened with sucrose or fructose feed cariogenic bacteria, partially counteracting the probiotic benefit. Xylitol-sweetened lozenges are preferred because xylitol itself has anti-cariogenic activity (it inhibits S. mutans growth and metabolism).
The right pattern: brush teeth normally before bed, then dissolve one oral probiotic lozenge in the mouth as the last thing before sleep. Do not eat, drink, rinse, or brush after the lozenge. The colonization happens overnight while the mouth is relatively dormant.
Practical Protocols by Indication
- Chronic halitosis (after ruling out underlying cause) — combine tongue scraping (morning), oil pulling (morning), and K12 lozenge (evening, last thing before sleep) for 4-6 weeks. Re-evaluate. If improved, continue indefinitely with K12 every 1-2 days as maintenance.
- Recurrent strep throat (3+ episodes per year) — K12 lozenge nightly for 90 days. Monitor through next at-risk season. If episodes reduced, may discontinue or use intermittently during cold/flu season.
- Recurrent otitis media in otitis-prone child — K12 lozenge (pediatric formulation) nightly for the at-risk season. Coordinate with pediatrician.
- Gingivitis, plaque accumulation, mild periodontitis — M18 lozenge twice daily for 90 days. Combine with comprehensive oral hygiene (brushing, flossing, tongue scraping, oil pulling). Re-evaluate at next dental cleaning.
- Moderate to severe periodontitis (with active scaling and root planing) — L. reuteri Prodentis lozenges twice daily for 12 weeks beginning at the time of scaling. Continue at maintenance dose of once daily for 6-12 months. Coordinate with periodontist.
- General oral microbiome optimization — combined K12 + M18 lozenge nightly for 30-60 days, then 2-3 times per week as maintenance.
None of these protocols replace standard dental care. They augment it. The oral probiotics are an addition to brushing, flossing, regular cleanings, and treatment of any active dental disease — not a substitute for any of those.
Cautions and Limitations
- Immunocompromised patients — oral probiotics are live organisms. In severely immunocompromised patients (advanced HIV/AIDS, active hematologic malignancy on intensive chemotherapy, post-transplant on heavy immunosuppression), bacteremia from live probiotics has been reported as a rare complication. Probiotic use should be cleared with the treating physician in these populations.
- Central venous catheter — patients with central lines have higher risk of probiotic-associated bacteremia and should generally avoid live probiotic supplementation.
- Endocarditis prophylaxis — patients with prosthetic heart valves, history of infective endocarditis, or certain congenital cardiac conditions are at increased risk of bacteremia-related endocarditis. Although oral commensal streptococcal bacteremia is what already happens during routine tooth brushing, the introduction of high-dose probiotic strains warrants discussion with cardiology.
- Concurrent antibiotics — oral antibiotics (especially broad-spectrum) will kill the probiotic strains. Schedule probiotic doses at least 2 hours apart from antibiotic doses; expect to need to re-establish colonization after the antibiotic course is complete.
- Concurrent chlorhexidine mouthwash — chlorhexidine will kill probiotic strains. Use one or the other, not both. If chlorhexidine is needed for an acute indication, suspend probiotic use; restart probiotics 1 week after stopping chlorhexidine.
- Concurrent oil pulling — can be combined, but separate them in time. Morning oil pulling, evening probiotic lozenge.
- Diabetes (poorly controlled) — the oral microbiome is significantly altered by hyperglycemia. Probiotic colonization may be less stable in poorly controlled diabetes. Improving glycemic control is a prerequisite for sustainable oral microbiome health.
- Smoking — tobacco smoke is severely toxic to the oral microbiome (commensals and probiotics alike) and is a major contributor to periodontitis progression. Smoking cessation is more important than any probiotic intervention.
- Cost — quality oral probiotics cost $20-35 per month. This is not trivial for many patients. If budget-constrained, prioritize tongue scraping (one-time scraper purchase, no recurring cost) and oil pulling (modest recurring cost for coconut oil) ahead of probiotic supplementation.
- Marketing claims — the oral probiotic market includes some products with weak or no evidence base. Stick with products containing specifically K12, M18, or L. reuteri Prodentis at clinically validated doses. Be skeptical of "10-strain oral probiotic" blends that include strains with no oral evidence base.
Key Research Papers
- Burton JP, Chilcott CN, Moore CJ, Speiser G, Tagg JR (2006). A preliminary study of the effect of probiotic Streptococcus salivarius K12 on oral malodour parameters. Journal of Applied Microbiology, 100(4):754-64. — PubMed
- Di Pierro F, Colombo M, Zanvit A, Risso P, Rottoli AS (2014). Use of Streptococcus salivarius K12 in the prevention of streptococcal and viral pharyngotonsillitis in children. Drug, Healthcare and Patient Safety, 6:15-20. — PubMed
- Di Pierro F et al. (2015). Use of a probiotic-based product containing Streptococcus salivarius K12 in the prevention of recurrent acute otitis media. International Journal of General Medicine, 8:303-8. — PubMed
- Burton JP, Drummond BK, Chilcott CN et al. (2013). Influence of the probiotic Streptococcus salivarius strain M18 on indices of dental health in children. Journal of Medical Microbiology, 62(Pt 6):875-884. — PubMed
- Wescombe PA, Hale JD, Heng NC, Tagg JR (2012). Developing oral probiotics from Streptococcus salivarius. Future Microbiology, 7(12):1355-71. — PubMed
- Krasse P, Carlsson B, Dahl C, Paulsson A, Nilsson A, Sinkiewicz G (2006). Decreased gum bleeding and reduced gingivitis by the probiotic Lactobacillus reuteri. Swedish Dental Journal, 30(2):55-60. — PubMed
- Vivekananda MR, Vandana KL, Bhat KG (2010). Effect of the probiotic Lactobacilli reuteri (Prodentis) in the management of periodontal disease: a preliminary randomized clinical trial. Journal of Oral Microbiology, 2:5344. — PubMed
- Tekce M, Ince G, Gursoy H et al. (2015). Clinical and microbiological effects of probiotic lozenges in the treatment of chronic periodontitis: a 1-year follow-up study. Journal of Clinical Periodontology, 42(4):363-72. — PubMed
- Power DA, Burton JP, Chilcott CN, Dawes PJ, Tagg JR (2008). Preliminary investigations of the colonisation of upper respiratory tract tissues of infants using a paediatric formulation of the oral probiotic Streptococcus salivarius K12. European Journal of Clinical Microbiology & Infectious Diseases, 27(12):1261-3. — PubMed
- Stensson M, Koch G, Coric S et al. (2014). Oral administration of Lactobacillus reuteri during the first year of life reduces caries prevalence in the primary dentition at 9 years of age. Caries Research, 48(2):111-7. — PubMed
- Náse L, Hatakka K, Savilahti E et al. (2001). Effect of long-term consumption of a probiotic bacterium, Lactobacillus rhamnosus GG, in milk on dental caries and caries risk in children. Caries Research, 35(6):412-20. — PubMed
- Roos K, Hakansson EG, Holm S (2001). Effect of recolonisation with "interfering" alpha streptococci on recurrences of acute and secretory otitis media in children: randomised placebo controlled trial. BMJ, 322(7280):210-2. — PubMed
- Hillman JD (2002). Genetically modified Streptococcus mutans for the prevention of dental caries. Antonie van Leeuwenhoek, 82(1-4):361-6. — PubMed
PubMed Topic Searches
- PubMed: S. salivarius K12 probiotic
- PubMed: S. salivarius M18 caries
- PubMed: L. reuteri Prodentis
- PubMed: Oral probiotic colonization mechanics
- PubMed: BLIS / salivaricin bacteriocins
Connections
- Oral Microbiome (Main Page)
- Oral Microbiome Benefits Hub
- Hydroxyapatite vs Fluoride
- Oil Pulling
- Tongue Scraping
- Probiotics (General)
- Gingivitis
- Periodontitis
- Halitosis
- Strep Throat
- Otitis Media
- SIBO
- Xylitol
- All Remedies
- All Dentistry