Tongue Scraping — Halitosis, Taste, and the Oral Microbiome
The posterior dorsum of the tongue is the largest reservoir of bacteria in the mouth — the rough surface of filiform papillae creates a vast surface area with microscopic crypts that trap food debris, dead epithelial cells, and bacterial biofilm. Approximately 60% of the bacterial load contributing to bad breath originates not from teeth or gums, but from this tongue coating. The volatile sulfur compounds (VSCs) responsible for the smell — hydrogen sulfide, methyl mercaptan, and dimethyl sulfide — are produced by gram-negative anaerobic bacteria metabolizing sulfur-containing amino acids (cysteine, methionine) from this trapped protein debris. A 2-thousand-year-old Ayurvedic intervention — the U-shaped copper or steel tongue scraper — mechanically removes this coating in 30 seconds of morning use, reducing VSC levels by ~75% in randomized trials and out-performing tongue brushing across multiple endpoints. This page covers the mechanism, the Cochrane evidence, copper vs steel scraper choice, and the swallowed-bacteria pathway to the gut.
Table of Contents
- History and Cultural Origins
- Tongue Anatomy and the Coating Problem
- Halitosis and Volatile Sulfur Compounds
- Cochrane Evidence: Scraping vs Brushing vs Nothing
- Taste Perception and Tongue Coating
- The Swallowed-Bacteria Pathway to the Gut
- Choosing a Tongue Scraper: Copper, Stainless Steel, Plastic
- How to Tongue Scrape Properly
- Key Research Papers
- Connections
- Featured Videos
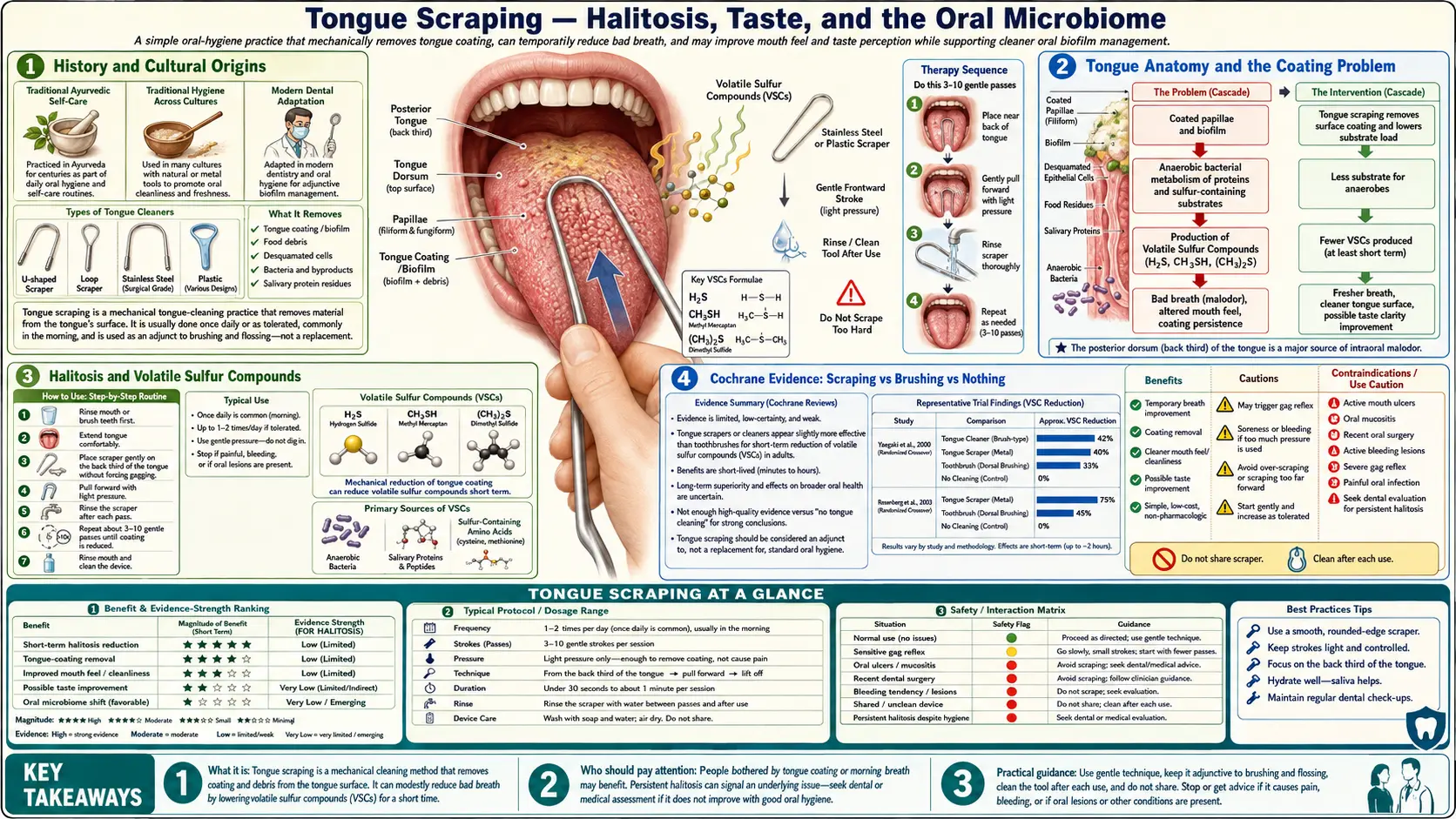
History and Cultural Origins
Tongue scraping is one of the oldest documented hygienic practices in human medicine. The Charaka Samhita (compiled approximately 200 BCE - 200 CE) prescribes it as a daily morning dinacharya (daily routine) practice, alongside oil pulling and oil massage. The Ayurvedic recommendation was for a copper scraper (jihwa prakshalana), based on the belief that copper's mild antimicrobial activity added to the mechanical effect.
The practice is documented independently across multiple cultures:
- India (Ayurveda) — copper or gold scrapers, daily morning use, embedded in the dinacharya routine.
- Africa — chewed-stick variants (Miswak from Salvadora persica) with tongue-scraping fibers, used across much of the Islamic world and East Africa.
- Pre-modern Europe — aristocratic European hygiene from the 15th-19th centuries included ivory, tortoiseshell, and silver tongue scrapers as standard items in personal grooming kits. Surviving examples from this period are common in museums.
- South America — indigenous Amazonian practices using carved wooden scrapers.
The practice essentially disappeared from mainstream Western dental hygiene during the 20th century, overtaken by the focus on toothbrush + toothpaste + dental floss. It re-entered Western awareness through two pathways in the early 2000s: the Ayurvedic revival in the natural-products movement, and the work of academic dental researchers (Quirynen, Pedrazzi, Outhouse) systematically comparing tongue scraping to tongue brushing in randomized trials.
Tongue Anatomy and the Coating Problem
The tongue surface is not smooth. It is covered in four types of specialized epithelial structures called papillae:
- Filiform papillae — the most numerous, distributed across the entire dorsum. These are slender, conical projections that do NOT contain taste buds. Their function is mechanical (grip and friction during chewing and speech) and tactile. They create a surface texture similar to fine velvet or a soft hairbrush — lots of crevices and microscopic surface area.
- Fungiform papillae — mushroom-shaped, scattered between the filiform papillae across the front two-thirds of the tongue. These DO contain taste buds (mostly sweet, salty, and umami detection).
- Foliate papillae — on the posterior lateral edges, containing taste buds (predominantly sour).
- Circumvallate papillae — the large, prominent papillae forming a V-shape near the back of the tongue, surrounded by deep moats containing taste buds (predominantly bitter).
The filiform papillae are the structural problem. Their microscopic crevices trap and accumulate three things:
- Sloughed-off dead epithelial cells from the tongue surface itself (constant turnover)
- Food debris that doesn't get washed away by saliva (especially protein-rich material from meat, dairy, eggs)
- Bacterial biofilm — predominantly anaerobic gram-negative species that thrive in the oxygen-poor microenvironment created by the dense biofilm structure
This combined material is what is called the "tongue coating" — visible to the eye as a white, yellow, brown, or sometimes black layer on the dorsum, especially the posterior third (the part closer to the throat that is harder to reach and harder to clean). The coating thickness correlates with halitosis severity, bacterial load, and the concentration of volatile sulfur compounds in exhaled breath.
The coating is also self-perpetuating. The bacterial biofilm produces an extracellular matrix of polysaccharides and proteins that holds the bacteria together and protects them from saliva, oxygen, and antimicrobials. Once established, the biofilm is resistant to removal by saliva alone or by gentle brushing.
Halitosis and Volatile Sulfur Compounds
The smell of bad breath is overwhelmingly produced by three small molecules collectively called volatile sulfur compounds (VSCs):
- Hydrogen sulfide (H₂S) — the rotten-egg smell, the dominant VSC in most cases of halitosis.
- Methyl mercaptan (CH₃SH) — rotting cabbage / sulfurous, particularly noxious; the principal VSC in patients with periodontal disease.
- Dimethyl sulfide ((CH₃)₂S) — cabbage-like odor; quantitatively smaller contribution but with very low olfactory threshold.
VSCs are produced by anaerobic gram-negative bacteria (predominantly Solobacterium moorei, Atopobium parvulum, Fusobacterium nucleatum, Prevotella species, Tannerella forsythia, Porphyromonas gingivalis) metabolizing sulfur-containing amino acids derived from protein debris. The metabolic pathway:
- Bacterial proteases break down protein debris into individual amino acids
- Sulfur-containing amino acids (cysteine, methionine) are taken up by VSC-producing bacteria
- Bacterial cysteine desulfhydrase and methionine gamma-lyase enzymes liberate the sulfur atoms as H₂S and CH₃SH respectively
- These small gases diffuse out of the biofilm into the air space, contributing to exhaled odor
Approximately 60-90% of bad-breath cases originate in the mouth (not from the lungs, sinuses, stomach, or systemic disease). Of the oral fraction, the tongue coating contributes more than the teeth and gums combined — the Yaegaki and Coil classic Japanese halitosis studies established this in the late 1990s, demonstrating that mechanical cleaning of the posterior tongue produces larger VSC reductions than any other single oral hygiene intervention.
The Outhouse Cochrane review (2006) on tongue scraping for halitosis concluded that tongue cleaning significantly reduces volatile sulfur compounds and self-reported breath odor, with tongue scraping somewhat more effective than tongue brushing. The Pedrazzi 2004 trial (Journal of Periodontology) directly compared toothbrush and tongue scraper for tongue cleaning, finding the scraper produced 75% reduction in VSCs vs the toothbrush's 45% reduction.
Cochrane Evidence: Scraping vs Brushing vs Nothing
The Cochrane Collaboration's Outhouse 2006 systematic review on tongue scraping for halitosis is the highest-quality evidence-grading effort on this question. Key findings:
- Two RCTs met inclusion criteria (the Pedrazzi 2004 and Quirynen 2004 trials).
- Both trials showed statistically significant reduction in VSCs from tongue cleaning vs no intervention.
- Tongue scrapers produced larger VSC reductions than tongue brushes (mean difference favored scrapers).
- The effect persisted as long as the intervention was maintained — it is a daily-use intervention, not a one-time cure.
- Authors noted limitations of the small number of trials and recommended additional research; subsequent trials have generally supported the Cochrane finding.
Why scrapers out-perform brushes: a tongue brush's soft bristles compress against the tongue surface but do not effectively pull material out of the inter-papillary crevices. A scraper's rigid edge, drawn across the surface with downward pressure, mechanically excavates the coating from between the filiform papillae and removes it bodily. The visible material accumulated on the scraper edge after each pull (white-yellow paste, often with substantial volume) is direct evidence of the difference — you can see what was extracted that brushing would have missed.
Additional evidence:
- Quirynen 2004 — tongue cleansers significantly reduced both bacterial load and improved taste perception in subjects with significant tongue coating.
- Solis 2011 — tongue scraping for 30 days reduced VSCs by 70-75% in subjects with morning breath as primary complaint.
- Van der Sleen 2010 systematic review — mechanical tongue cleaning is effective for breath odor and tongue coating reduction; scrapers preferred over brushes.
- Faveri 2006 — cross-over comparing morning breath interventions; tongue scraping was the highest-impact single intervention.
Taste Perception and Tongue Coating
A frequently overlooked benefit of regular tongue scraping is improved taste sensitivity. The mechanism is straightforward: the taste buds in the fungiform, foliate, and circumvallate papillae need direct contact with dissolved food chemicals to function. A thick coating of biofilm and debris physically shields the taste buds from this contact, dulling all four primary tastes.
The Quirynen 2004 trial measured taste perception before and after introduction of tongue cleaning, finding statistically significant improvement in taste threshold detection across all four primary tastes (sweet, salty, sour, bitter) within 2 weeks. Subjects often report that food becomes "more flavorful" after a few weeks of consistent tongue scraping — this is the unmasking of taste buds that had been functionally blunted by coating.
This has practical relevance for:
- Patients with reduced appetite (especially elderly patients) where dulled taste contributes to under-eating
- Patients trying to reduce sugar or salt intake (more sensitive taste means lower thresholds needed)
- Patients trying to enjoy whole-food cooking after years of processed-food diet (rediscovering subtle flavors)
- Patients post-chemotherapy with treatment-related taste alteration (mechanism is different but tongue hygiene supports any return of function)
The taste-perception benefit is one of the more immediately rewarding effects of starting a tongue-scraping practice — users typically notice within 1-2 weeks that morning coffee, fruit, and salads taste fuller and more interesting.
The Swallowed-Bacteria Pathway to the Gut
An adult swallows approximately 1.5 liters of saliva per day. That saliva carries with it a continuous bacterial load harvested from the oral cavity — primarily from the tongue coating (largest reservoir) and the gingival sulcus. Most of these swallowed bacteria are killed by gastric acid in the stomach. However, in two scenarios, swallowed oral bacteria reach the gut alive in significant numbers:
- Hypochlorhydria (low stomach acid) — older adults, patients on long-term proton pump inhibitors (omeprazole, esomeprazole, etc.), patients with atrophic gastritis, and patients with H. pylori infection have reduced gastric acid output. Without adequate acid, swallowed oral bacteria survive transit to the small intestine, where they can colonize ectopically (contributing to SIBO — small intestinal bacterial overgrowth) and downstream colon dysbiosis.
- Bolus protection — bacteria embedded within food boluses are partially protected from gastric acid by the surrounding food matrix. Subsequent gastric emptying delivers viable bacteria to the duodenum.
The 2019 Olsen and Yamazaki review (Journal of Oral Microbiology) summarizes the evidence that oral bacteria translocate to and influence the gut microbiome. Patients with periodontitis have measurably increased abundance of oral-origin taxa (including Fusobacterium nucleatum, the same organism strongly linked to colorectal cancer) in their stool. The same connection has been demonstrated for inflammatory bowel disease, liver cirrhosis, and rheumatoid arthritis — conditions where downstream microbiome consequences of oral dysbiosis appear to play a measurable role.
Tongue scraping reduces the bacterial burden delivered to the gut via the swallowed-saliva pathway. A 30-second morning scrape can reduce total oral bacterial load by a substantial fraction, with proportional reduction in the daily swallowed pathogen dose. This is one of the rare interventions that simultaneously improves oral health (local), gut health (downstream), and systemic inflammation (further downstream) through a single mechanism.
For patients with diagnosed SIBO, IBD, or chronic gut inflammation, tongue scraping is a reasonable adjunct to whatever gut-directed therapy is in progress. It will not by itself reverse those conditions, but it removes one ongoing input that can perpetuate or worsen them. For more on the gut connection, see SIBO and Inflammatory Bowel Disease.
Choosing a Tongue Scraper: Copper, Stainless Steel, Plastic
Three materials dominate the tongue-scraper market. Each has tradeoffs:
- Copper (traditional Ayurvedic choice) — The original material specified in Ayurvedic texts. Copper has mild antimicrobial activity (the Cu ion releases at low rate from the metal surface), which adds an antimicrobial effect on top of the mechanical cleaning. Copper develops a darker patina over time which is cosmetic, not harmful. Slightly heavier and stiffer than stainless steel; the U-shape holds its form well. Cost: $8-15. Source: numerous Ayurvedic brands available on Amazon and at natural food stores.
- Stainless steel — the most common modern material. Inert (no copper-style ion release, no patina), easy to clean, dishwasher-safe, lasts indefinitely. The most hygienic choice from a "what is on the scraper between uses" perspective. Slightly less rigid than copper, sometimes flexes during use. Cost: $5-10.
- Plastic — cheapest, lightest, slightly flexible. Modern plastic scrapers (often called "Orabrush" or similar consumer brands) are well-designed and effective. Limitations: plastic eventually shows wear at the scraping edge, requiring replacement every 6-12 months. Some plastic scrapers add bristles that move them toward "tongue brush" territory (less effective). Cost: $3-5.
The differences in clinical outcome between copper, stainless steel, and plastic scrapers are small in published trials — the dominant factor is whether you actually use one consistently. The handful of head-to-head trials comparing materials (mostly small studies) have not shown a definitively superior material.
Recommendation: stainless steel for most users (hygienic, inexpensive, lasts forever). Copper for users with cultural or traditional preference, willing to clean and dry it after each use to maintain. Avoid scrapers with attached bristles (move toward "brush" territory and lose the rigid-edge mechanical advantage).
Avoid:
- Using a toothbrush as a tongue scraper — less effective per the Pedrazzi data
- Tongue scrapers with attached bristles — same problem
- Excessively wide scrapers (more than 1.5 inches across) — harder to reach the posterior tongue
- Excessively curved scrapers that don't conform well to your tongue's natural curve
How to Tongue Scrape Properly
The technique is simple:
- When — first thing in the morning, before eating, drinking, brushing, or oil pulling. The overnight accumulation is at maximum.
- Position — standing at the bathroom sink, mouth open wide, tongue extended forward as far as comfortable.
- Grip — hold the scraper with both hands, one on each end of the U. This gives even pressure across the scraping edge.
- Placement — reach the scraper as far back on the tongue as you can without triggering the gag reflex. The posterior third of the tongue is where the coating is heaviest and the cleaning yield is highest.
- The stroke — press the scraper down onto the tongue surface with moderate pressure, then pull forward in one continuous motion from back to front. The visible coating will accumulate on the scraping edge.
- Rinse the scraper — under the tap, rinse the accumulated material off the scraper after each stroke.
- Repeat — 5-10 strokes total, working the entire tongue surface (center, then each lateral side).
- Rinse the mouth — once with warm water at the end.
- Then continue your morning oral routine — optional oil pulling, then tooth brushing with hydroxyapatite toothpaste, then floss.
The whole tongue scraping process takes 30-60 seconds once you have the technique. It is by far the highest-yield-per-minute oral hygiene practice for halitosis specifically.
Two common technique mistakes:
- Not reaching far enough back — the cleaning yield drops dramatically if you only scrape the front and middle of the tongue. The posterior third is the highest-bacteria zone. Build up tolerance to reaching back further over the first week of practice.
- Excessive pressure — the goal is mechanical removal of the surface coating, not abrading the tongue surface itself. If your tongue feels sore or bleeds, you are pressing too hard. Use firm but moderate pressure, and let the scraper's edge do the work.
Between uses, rinse the scraper, shake dry, and store in a clean place (ideally not in a closed wet container where bacteria can grow). Stainless steel scrapers can periodically go in the dishwasher. Copper scrapers should be hand-washed and dried to maintain the surface.
Key Research Papers
- Outhouse TL, Al-Alawi R, Fedorowicz Z, Keenan JV (2006). Tongue scraping for treating halitosis. Cochrane Database of Systematic Reviews, (2):CD005519. — PubMed
- Pedrazzi V, Sato S, de Mattos Mda G, Lara EH, Panzeri H (2004). Tongue-cleaning methods: a comparative clinical trial employing a toothbrush and a tongue scraper. Journal of Periodontology, 75(7):1009-12. — PubMed
- Quirynen M, Avontroodt P, Soers C et al. (2004). Impact of tongue cleansers on microbial load and taste. Journal of Clinical Periodontology, 31(7):506-10. — PubMed
- Van der Sleen MI, Slot DE, Van Trijffel E et al. (2010). Effectiveness of mechanical tongue cleaning on breath odour and tongue coating: a systematic review. International Journal of Dental Hygiene, 8(4):258-68. — PubMed
- Yaegaki K, Coil JM (2000). Examination, classification, and treatment of halitosis; clinical perspectives. Journal of the Canadian Dental Association, 66(5):257-61. — PubMed
- Solis AC, Marques A, Pannuti CM et al. (2011). Evaluation of an essential oil mouthrinse, chlorhexidine and a tongue scraper on tongue coating and breath odor. — PubMed
- Faveri M, Hayacibara MF, Pupio GC, Cury JA, Tsuzuki CO, Hayacibara RM (2006). A cross-over study on the effect of various therapeutic approaches to morning breath odour. Journal of Clinical Periodontology, 33(8):555-60. — PubMed
- Kapoor U, Sharma G, Juneja M, Nagpal A (2017). Halitosis: current concepts on etiology, diagnosis and management. European Journal of Dentistry, 10(2):292-300. — PubMed
- Tonzetich J (1977). Production and origin of oral malodor: a review of mechanisms and methods of analysis. Journal of Periodontology, 48(1):13-20. — PubMed
- Roldan S, Herrera D, Sanz M (2003). Biofilms and the tongue: therapeutical approaches for the control of halitosis. Clinical Oral Investigations, 7(4):189-97. — PubMed
- Olsen I, Yamazaki K (2019). Can oral bacteria affect the microbiome of the gut? Journal of Oral Microbiology, 11(1):1586422. — PubMed
- Allaker RP, Waite RD, Hickling J et al. (2008). Topographic distribution of bacteria associated with oral malodour on the tongue. Archives of Oral Biology, 53 Suppl 1:S8-12. — PubMed
PubMed Topic Searches
- PubMed: Tongue scraping and VSCs
- PubMed: Tongue coating microbiology
- PubMed: Brush vs scraper head-to-head
- PubMed: Oral-gut bacterial translocation
- PubMed: Taste perception and tongue hygiene
Connections
- Oral Microbiome (Main Page)
- Oral Microbiome Benefits Hub
- Hydroxyapatite vs Fluoride
- Oil Pulling
- Oral Probiotic Strains
- Ayurveda
- Halitosis
- Gingivitis
- Periodontitis
- SIBO
- Inflammatory Bowel Disease
- Copper
- Stomach Acid & Hypochlorhydria
- All Remedies
- All Dentistry