Avoiding Triggers for Gut Healing
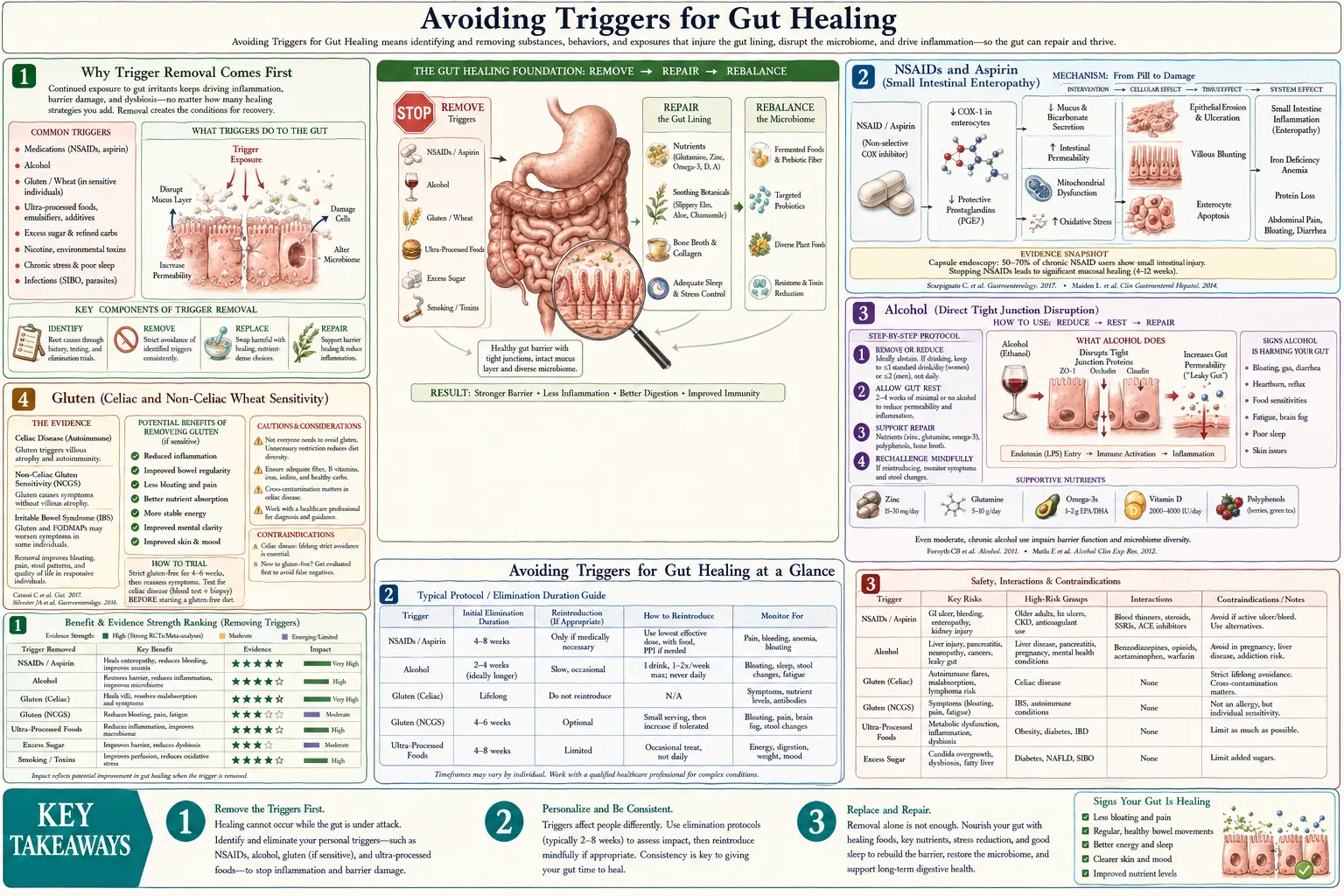
The single most overlooked aspect of gut healing is the recognition that you cannot heal a tissue that is being continuously re-injured. The intestinal epithelium turns over every 3-5 days — remarkable regenerative capacity that is largely wasted if the same daily insults are still present. NSAIDs (ibuprofen, naproxen, aspirin) damage the small intestinal mucosa in approximately 70% of chronic users on capsule endoscopy studies. Alcohol directly disrupts tight junctions within hours of ingestion. Gluten in celiac patients, and in non-celiac wheat-sensitive patients, increases zonulin and degrades barrier integrity. Chronic psychological stress raises corticotropin-releasing factor and activates mucosal mast cells, opening tight junctions and amplifying inflammation. Glyphosate residue in non-organic grain and soy, while controversial in mechanism, correlates with multiple gastrointestinal disease incidence patterns. This deep-dive walks through the major modifiable triggers, the practical work of identifying which apply to you (food and symptom diary, lactulose-mannitol permeability testing, breath testing for SIBO), and a structured elimination-and-reintroduction protocol that systematically isolates individual triggers.
Table of Contents
- Why Trigger Removal Comes First
- NSAIDs and Aspirin (Small Intestinal Enteropathy)
- Alcohol (Direct Tight Junction Disruption)
- Gluten (Celiac and Non-Celiac Wheat Sensitivity)
- Glyphosate Residue (The Controversial Trigger)
- Chronic Psychological Stress (CRF and Mast Cells)
- Chronic Infection (H. pylori, SIBO, Parasites)
- Individual Food Sensitivities (Beyond Gluten)
- Identification Protocol (Diary, Testing, Elimination)
- Structured Elimination and Reintroduction
- Key Research Papers
- Connections
- Featured Videos
Why Trigger Removal Comes First
The cellular biology of intestinal epithelial regeneration is remarkable. Crypt stem cells at the base of intestinal villi divide approximately every 24 hours, producing progenitor cells that migrate up the villus axis, mature into functional enterocytes, perform their absorptive and barrier functions for 3-5 days, and then are shed at the villus tip into the lumen. The entire epithelial surface is replaced approximately twice per week. This is faster turnover than any other tissue in the body except the bone marrow and certain hair follicles.
This regenerative capacity means that the gut can heal from substantial damage very quickly — if the damaging input is removed. NSAID-induced gastropathy resolves within weeks of NSAID discontinuation. Alcoholic gut permeability normalizes within months of abstinence in most patients. Celiac mucosal villous atrophy reverses, often completely, on strict gluten-free diet over 6-24 months. The constraint on gut healing is not regenerative capacity. The constraint is the rate of ongoing injury relative to the rate of regeneration.
This is why trigger identification and removal logically comes first in any gut-healing protocol. Substrate provision (bone broth, glutamine) and microbial support (probiotics, fermented foods) accelerate the rate of repair, but if the daily damaging input continues, even maximally optimized regeneration will not catch up. The patient who continues to take ibuprofen three times daily for joint pain while taking 15 grams of L-glutamine and drinking bone broth will see modest if any improvement. Stopping the ibuprofen and continuing the supportive nutrition will produce dramatic improvement within weeks.
NSAIDs and Aspirin (Small Intestinal Enteropathy)
Non-steroidal anti-inflammatory drugs (ibuprofen, naproxen, diclofenac, ketorolac, indomethacin, meloxicam, celecoxib) are the most underappreciated chronic gut injury source in the United States. Approximately 30 million Americans take an NSAID daily, mostly for chronic musculoskeletal pain, headache, or cardioprotection (low-dose aspirin). The well-known upper-GI risks — gastric ulcer, duodenal ulcer, GI bleeding — are clinically obvious and managed with proton pump inhibitor co-prescription. The less-known and equally important risk is small intestinal enteropathy, which proton pump inhibitors do not prevent (and may worsen via altered microbiome).
The mechanism is two-fold: (1) NSAIDs inhibit cyclooxygenase-1 (COX-1), reducing prostaglandin-mediated mucus secretion and bicarbonate production that protect mucosa, and (2) NSAIDs uncouple mitochondrial oxidative phosphorylation in enterocytes, producing ATP depletion and direct epithelial injury. The combination opens tight junctions, allows enteric bacteria and bile acids to penetrate, and produces a characteristic "diaphragm-like" stricturing in chronic users that is visible on capsule endoscopy.
Bjarnason et al. capsule endoscopy studies have shown that approximately 70% of chronic NSAID users (defined as daily use for 3+ months) have visible small intestinal mucosal breaks, erosions, or hemorrhage. Most are clinically silent; a subset present with iron-deficiency anemia, occult GI blood loss, hypoalbuminemia (from protein-losing enteropathy), or rarely with stricture-related obstruction.
Practical considerations for the patient pursuing gut healing:
- Stop all unnecessary NSAID use — including OTC ibuprofen for general aches, post-exercise inflammation, "as-needed" pain
- For chronic pain conditions, work with the prescribing physician on alternatives: acetaminophen (different mechanism, no NSAID-style gut injury), topical NSAIDs (much less systemic absorption), gabapentinoids, low-dose naltrexone for pain, physical therapy, weight loss for joint pain
- For cardioprotective aspirin, weigh the cardioprotection vs the gut injury for each patient. In primary prevention, the USPSTF has narrowed indications — many adults previously on prophylactic aspirin no longer have indication
- If NSAID use is medically necessary, co-prescription of rebamipide (available in Japan, not US), misoprostol, or PPI provides some upper-GI protection but does not prevent small intestinal damage
- Bone broth, glutamine, and L. rhamnosus GG are reasonable adjuncts during NSAID withdrawal and gut repair, but cannot fully compensate for ongoing NSAID exposure
Alcohol (Direct Tight Junction Disruption)
Alcohol effects on the gut are immediate and dose-dependent. Single-dose studies in human volunteers show that 0.5-1 g/kg ethanol (approximately 3-5 standard drinks in a 70 kg adult) produces measurable increases in intestinal permeability within hours, with elevated serum LPS (lipopolysaccharide, a marker of bacterial translocation across the gut wall). The mechanism involves direct phosphorylation of tight junction proteins (claudins, ZO-1), acetaldehyde-mediated oxidative injury, and microbiome dysbiosis with reduced butyrate-producing genera.
Chronic alcohol use compounds the problem. Heavy drinkers (more than 4 drinks/day for men, 3/day for women, sustained for years) develop a leaky gut state with chronic endotoxemia, low-grade systemic inflammation, and accelerated liver fibrosis (the endotoxin-induced Kupffer cell activation is part of the alcohol-to-cirrhosis mechanism, not just direct ethanol hepatotoxicity).
For a patient pursuing gut healing, alcohol elimination during the active healing phase is the strongest recommendation. After 6-12 months of strict abstinence and gut healing protocol, occasional small alcohol consumption (1 drink, 1-2 times per week, ideally with food) is usually tolerated in non-IBD, non-celiac patients. Patients with active IBD, advanced liver disease, or alcohol use disorder should remain abstinent permanently.
Practical notes:
- "Clean" alcohol (distilled spirits, dry wine) is not less gut-damaging than beer or sweet wine — the ethanol is the primary problem, not the additives or sugars
- Red wine's polyphenol content does not compensate for the ethanol gut injury in someone with active gut symptoms
- Non-alcoholic beer and wine alternatives have improved dramatically in the past 5 years and are reasonable substitutes for the ritual of drinking
- Cannabis is a separate question; gut effects of cannabis are less studied and less obviously injurious than alcohol but include cannabinoid hyperemesis syndrome in heavy chronic users
Gluten (Celiac and Non-Celiac Wheat Sensitivity)
Gluten in genetically susceptible individuals (HLA-DQ2 / HLA-DQ8 positive, approximately 30% of the US population by haplotype) can trigger celiac disease — an autoimmune enteropathy with villous atrophy, intraepithelial lymphocytosis, and crypt hyperplasia. Approximately 1% of the US population has biopsy-confirmed celiac. Strict lifelong gluten elimination is the only effective treatment.
The more complicated story is non-celiac wheat sensitivity (NCWS) — symptoms triggered by wheat ingestion in patients who do not have celiac and do not have wheat allergy. Estimates of NCWS prevalence vary widely (0.5-13% of population depending on study). Symptoms include bloating, abdominal pain, diarrhea, brain fog, fatigue, joint pain, and skin manifestations triggered within hours to days of wheat ingestion and resolving with strict wheat elimination.
The mechanism of NCWS is not fully understood. Candidates include:
- Amylase-trypsin inhibitors (ATIs) — modern wheat-breeding-derived proteins that activate TLR4 on innate immune cells, producing inflammation independent of the gluten protein itself
- FODMAP content of wheat — fructans in wheat are fermentable and contribute to bloating; some patients labeled NCWS may actually be reacting to the FODMAP component rather than the gluten
- Wheat germ agglutinin (WGA) and other lectins — bind to glycoproteins on the gut epithelium and may disrupt tight junctions in susceptible individuals
- Zonulin-mediated barrier disruption — Fasano's work showing that gliadin triggers zonulin release in both celiac and non-celiac individuals, with downstream tight junction opening
Practical approach: for any patient with chronic GI symptoms, a 4-6 week strict gluten elimination trial (no wheat, rye, barley, or contaminated oats) is reasonable. If symptoms improve, formal celiac evaluation (tissue transglutaminase IgA + total IgA, plus duodenal biopsy if positive) is appropriate — ideally before the gluten elimination, since the testing requires recent gluten exposure to be accurate. If celiac is excluded and gluten elimination still helps symptoms, NCWS is the working diagnosis and strict avoidance is the management. Reintroduction trials after several months of gut healing sometimes show improved tolerance in NCWS, though strict avoidance often remains necessary for symptom freedom.
Glyphosate Residue (The Controversial Trigger)
Glyphosate (the active ingredient in Roundup and many other herbicides) is the most-applied agricultural chemical in the world by tonnage. It is used extensively as a desiccant on wheat, oats, barley, and lentils at harvest in addition to its weed-control role in glyphosate-tolerant GMO soybean and corn cultivation. Residue is detectable in approximately 75-95% of non-organic processed food samples tested.
The proposed mechanisms by which dietary glyphosate residue might affect the gut are speculative but biologically plausible:
- Glyphosate inhibits the shikimate pathway for aromatic amino acid synthesis — a pathway absent in human cells but present in many gut bacteria. Selective effects on commensal flora could alter the microbiome composition
- Animal studies suggest glyphosate residue reduces lactobacilli and bifidobacteria while sparing or favoring Clostridia and Enterobacteriaceae — a shift toward a pro-inflammatory microbiome profile
- Glyphosate is a chelator of divalent cations (zinc, manganese, calcium), potentially impairing absorption
- The combination effect with adjuvants in commercial Roundup formulations may exceed the direct glyphosate effect
Critics note that human dietary glyphosate exposure is well below acute toxicity thresholds and that the strongest epidemiologic studies do not yet show clear GI disease associations specific to glyphosate. The IARC classification of glyphosate as Group 2A (probably carcinogenic) is contested by other regulatory bodies.
The pragmatic position for a patient pursuing gut healing is to reduce glyphosate exposure during the healing period by emphasizing organic grain and legume sources, and to monitor whether symptom improvement correlates. Organic wheat, oats, lentils, beans, and corn are the highest-yield substitutions; organic soy is harder to find but worth the effort if soy is a staple. The cost premium is real, but for the duration of an active gut-healing protocol, reasonable.
Chronic Psychological Stress (CRF and Mast Cells)
Chronic psychological stress has measurable, mechanistic gut effects that are easy to overlook in a nutrition-and-supplement-focused gut healing protocol. The major pathway is the corticotropin-releasing factor (CRF) signaling axis. Psychological stress activates the hypothalamic-pituitary-adrenal axis, releasing CRF systemically and locally in the gut. Gut mucosal mast cells express CRF receptors, and CRF binding triggers mast cell degranulation, releasing histamine, tryptase, and other pro-inflammatory mediators directly into the gut wall.
The Vanuytsel 2014 paper in Gut demonstrated this elegantly: healthy volunteers given a public-speaking stress task had measurable increases in intestinal permeability (lactulose-mannitol ratio) within hours of the stressor. The effect was blocked by mast cell stabilizer pretreatment, confirming the mast cell mediation. Chronic stress amplifies and prolongs this effect.
Practical implications:
- Patients pursuing gut healing while in active chronic-stress situations (job loss, divorce, caregiver burden, untreated anxiety or depression) will see limited progress regardless of optimal nutrition and supplements
- Stress reduction interventions with evidence: cognitive behavioral therapy for IBS (multiple RCTs), gut-directed hypnotherapy (Manchester protocol, strong evidence for IBS), mindfulness-based stress reduction, yoga, regular aerobic exercise
- Adequate sleep (7-9 hours) is foundational — sleep deprivation activates CRF independently and exacerbates gut symptoms
- For anxious patients with significant gut symptoms, low-dose tricyclic antidepressants (amitriptyline 10-25 mg at bedtime) have evidence for IBS symptom reduction beyond the antidepressant effect
- SSRIs and SNRIs have mixed evidence in IBS and may worsen GI symptoms in a subset of patients; consider individual response
Chronic Infection (H. pylori, SIBO, Parasites)
Chronic enteric infection is an often-missed driver of persistent gut symptoms and barrier dysfunction. Three categories deserve specific consideration:
- Helicobacter pylori — gastric infection that affects approximately 50% of the global population (lower in developed countries). Diagnostic test of choice is urea breath test or stool antigen test; treatment is quadruple therapy (typically PPI + bismuth + tetracycline + metronidazole for 14 days, or PPI + amoxicillin + clarithromycin + metronidazole). Pursue eradication in patients with peptic ulcer disease, MALT lymphoma, atrophic gastritis, or active chronic gastric symptoms. Even in asymptomatic carriers, treatment is increasingly recommended given the gastric cancer risk.
- Small intestinal bacterial overgrowth (SIBO) — abnormal bacterial colonization of the small intestine, where bacteria should be sparse compared with the colon. Diagnosed with breath testing (hydrogen and methane after lactulose or glucose challenge), though breath testing has significant sensitivity and specificity limitations. Treatment depends on the type: hydrogen-predominant SIBO with rifaximin (550 mg TID for 14 days); methane-predominant (now called IMO, intestinal methanogen overgrowth) with rifaximin plus neomycin or metronidazole. After eradication, prokinetics (low-dose erythromycin, prucalopride, or natural prokinetics like ginger) to prevent recurrence. See the comprehensive SIBO page for detail.
- Parasitic infection — consider in patients with travel history, immigration history, well-water exposure, or unexplained chronic GI symptoms. Stool ova and parasite testing has poor sensitivity; PCR-based stool panels (BioFire GI panel, Quest GI Effects) are more sensitive. Specific organisms: Giardia lamblia (the most common gut parasite in the US, often missed because of cyst shedding intermittency), Cryptosporidium, Entamoeba histolytica, Blastocystis hominis (pathogenicity debated), Dientamoeba fragilis.
A patient with chronic gut symptoms and stalled progress on dietary and supplement intervention warrants formal infectious workup. Treating the underlying infection often produces dramatic improvement that no dietary protocol alone would have achieved.
Individual Food Sensitivities (Beyond Gluten)
Beyond gluten, the major individual food sensitivities that can drive ongoing gut inflammation:
- Dairy — either lactose intolerance (enzyme-based) or casein/whey protein sensitivity (immune-based). Casein A1 vs A2 protein difference is a relevant emerging consideration — conventional Holstein cattle dairy is mostly A1, while goat, sheep, water buffalo, and Jersey/Guernsey cattle produce predominantly A2 milk that some A1-sensitive patients tolerate
- Eggs — common food allergy in children, less common but real in adults; ovalbumin and ovomucoid the most common allergens
- Corn — both as a direct allergen and as a common contamination source (most processed food contains corn derivatives)
- Soy — food allergen plus phytoestrogen and goitrogen content; many patients tolerate fermented soy (miso, tempeh) better than unfermented (tofu, soy milk)
- Nightshades — tomato, potato, pepper, eggplant; alkaloid content (solanine, capsaicin) drives symptoms in a subset of patients, particularly with joint inflammation
- FODMAP-heavy foods — onion, garlic, apple, pear, mango, watermelon, wheat, beans, lactose-containing dairy. In FODMAP-sensitive IBS patients, a structured low-FODMAP elimination followed by systematic reintroduction is the evidence-based approach
- Histamine-heavy foods — aged cheese, fermented food, alcohol, cured meats, leftovers (histamine accumulates over time in refrigerated food). Relevant for the histamine-intolerant / mast cell activation subset
- Sulfite-containing foods and wine — less common than reputation suggests, but real in some patients
The systematic approach is structured elimination and reintroduction (next section), not broad-panel "IgG food sensitivity" testing — the IgG tests have poor specificity (IgG is a normal immune response to recent food exposure, not a pathological sensitivity indicator), and many patients are misled into restricting foods that are not actually causing problems.
Identification Protocol (Diary, Testing, Elimination)
The structured workup for identifying gut triggers in an individual patient:
- Detailed food and symptom diary — 2-4 weeks of recording everything eaten plus symptoms (bloating, pain, stool form using Bristol Stool Form Scale, energy, mood, sleep). Look for temporal patterns. Specific food-to-symptom correlation often becomes obvious that was invisible without recording.
- Medication review — NSAID frequency (including OTC use), PPI duration of use, antibiotic history, opioid use (chronic constipation), metformin (GI effects), SSRIs.
- Celiac screen — tissue transglutaminase IgA + total IgA, before any gluten elimination. If positive, EGD with duodenal biopsy for confirmation.
- SIBO breath test — lactulose or glucose breath test for hydrogen and methane.
- H. pylori test — urea breath test or stool antigen if upper GI symptoms.
- Comprehensive stool analysis — ova/parasite plus PCR pathogen panel for the chronic-symptom patient.
- Intestinal permeability test (optional) — lactulose-mannitol urinary excretion ratio is the validated marker. Less commonly available; useful for objective monitoring of response to treatment.
- Inflammatory markers — fecal calprotectin to distinguish IBD from IBS; C-reactive protein for systemic inflammation.
- Vitamin/mineral panel — B12, folate, iron studies, zinc, vitamin D, magnesium — commonly deficient in malabsorption, useful for objective monitoring.
Structured Elimination and Reintroduction
The evidence-based approach to identifying individual food triggers is structured elimination followed by systematic reintroduction.
Phase 1: Baseline elimination (4-6 weeks). Remove the most common triggers simultaneously: gluten, dairy, eggs, soy, corn, peanuts, shellfish, nightshades, refined sugar, alcohol, processed food. Continue this restricted diet for 4-6 weeks while symptoms ideally improve substantially. If symptoms do not improve in this phase, the trigger may not be food-related and other categories (chronic infection, NSAIDs, stress) should be reconsidered.
Phase 2: Systematic reintroduction (8-16 weeks). Reintroduce one food category every 3-7 days. Add a substantial serving of the test food on Day 1, then return to baseline elimination diet for Days 2-3. Watch for symptom recurrence (bloating, pain, change in bowel habit, rash, fatigue, brain fog, mood change, sleep disruption) within 72 hours of test food ingestion. If symptoms recur, that food is a positive trigger and should be removed. If no symptoms in 72 hours, the food can be reintroduced into the diet and a new test food added on Day 7.
Phase 3: Long-term diet construction. Build a sustainable diet around the foods that tested negative (no symptom recurrence). Foods that tested positive can be permanently avoided, or retested after 6-12 months of healing — some food sensitivities resolve with adequate gut repair, while others (particularly true allergies and celiac) are permanent.
Common reintroduction orders, easiest to hardest:
- Eggs (often well tolerated, easy to test)
- Nightshades
- Nuts and seeds (one type at a time)
- Dairy: butter and ghee first, then fermented dairy (yogurt, kefir), then aged cheese, then fresh milk
- Corn (separate from other grains)
- Soy (fermented forms first)
- Gluten-containing grains (often the most reactive; test last; some patients never reintroduce)
- Refined sugar (often last; many patients find symptom-free life is better without)
Working with a registered dietitian experienced in elimination diets can substantially improve adherence and reduce the risk of unnecessary nutritional restriction.
Key Research Papers
- Bjarnason I et al. (2018). Mechanisms of damage to the gastrointestinal tract from nonsteroidal anti-inflammatory drugs. Gastroenterology. — PubMed
- Vanuytsel T et al. (2014). Psychological stress and corticotropin-releasing hormone increase intestinal permeability in humans by a mast cell-dependent mechanism. Gut. — PubMed
- Bode JC, Bode C (1997). Effect of alcohol consumption on the gut. Best Pract Res Clin Gastroenterol. — PubMed
- Hollon J et al. (2015). Effect of gliadin on permeability of intestinal biopsy explants from celiac disease patients and patients with non-celiac gluten sensitivity. Nutrients. — PubMed
- Fasano A (2012). Zonulin, regulation of tight junctions, and autoimmune diseases. Ann N Y Acad Sci. — PubMed
- Catassi C et al. (2015). Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts' Criteria. Nutrients. — PubMed
- Junker Y et al. (2012). Wheat amylase trypsin inhibitors drive intestinal inflammation via activation of toll-like receptor 4. J Exp Med. — PubMed
- Halmos EP et al. (2014). A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology. — PubMed
- Pimentel M et al. (2020). ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. Am J Gastroenterol. — PubMed
- Camilleri M (2019). Leaky gut: mechanisms, measurement and clinical implications in humans. Gut. — PubMed
- Mu Q et al. (2017). Leaky gut as a danger signal for autoimmune diseases. Front Immunol. — PubMed
- Madsen K et al. (2001). Probiotic bacteria enhance murine and human intestinal epithelial barrier function. Gastroenterology. — PubMed
PubMed Topic Searches
- PubMed: NSAID enteropathy
- PubMed: Alcohol and gut barrier
- PubMed: Non-celiac wheat sensitivity
- PubMed: Stress and gut barrier
- PubMed: Elimination diet protocols
Connections
- Gut Healing Overview
- Gut Healing Benefits Hub
- GAPS Diet
- Bone Broth and Glutamine
- Probiotic Strains for Repair
- SIBO
- Celiac Disease
- Irritable Bowel Syndrome
- Crohn's Disease
- Helicobacter pylori
- Glyphosate
- Glyphosate (Toxin Profile) — the shikimate-pathway and microbiome argument behind the residue trigger discussed above.
- Alcohol
- Stress Management
- Stool Tests
- Immune Boosting