Bone Broth and Glutamine for Gut Healing
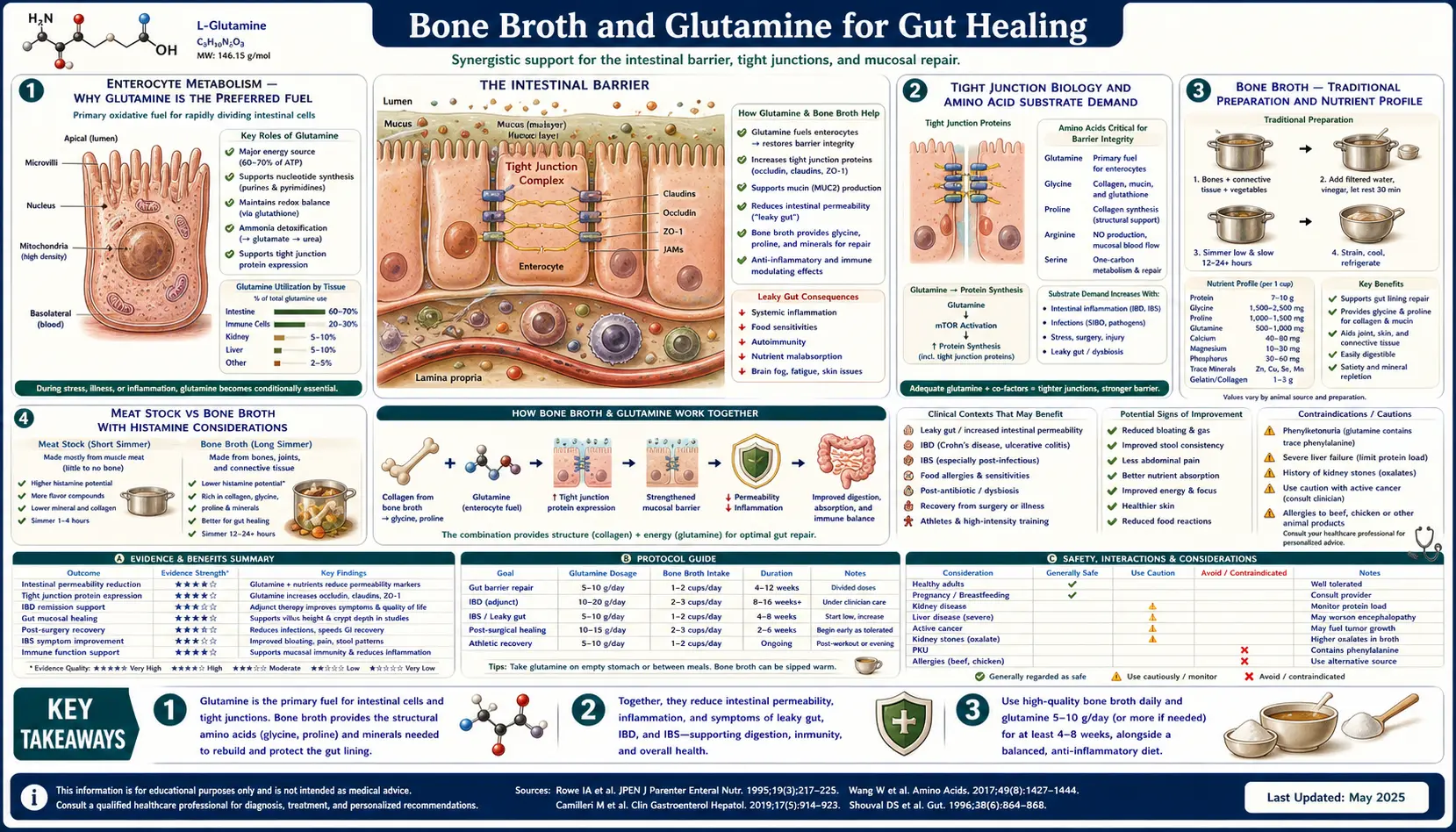
Bone broth and the isolated amino acid glutamine occupy the same conceptual position in gut healing — both deliver the specific molecular substrates that the intestinal epithelium needs to rebuild itself. The small intestinal enterocyte is metabolically unusual: it preferentially oxidizes glutamine rather than glucose for ATP, deriving up to 70% of its energy from glutamine in healthy postabsorptive states. The tight junction proteins (claudin-1, occludin, zonula occludens-1) and the mucin layer above the epithelium are continuously synthesized from dietary amino acids, with glycine, proline, and hydroxyproline particularly important for the collagen and gelatin scaffolding of the lamina propria beneath the epithelium. Long-simmered animal bones deliver all of these in a digestible form, and clinical-grade isolated L-glutamine adds reliable dose control where higher amounts are needed. This deep-dive walks through the metabolism, the practical preparation of bone broth, the clinical evidence for isolated glutamine supplementation, the supporting amino acid co-factors (glycine, proline), the collagen peptide alternative, and the rare but real cautions.
Table of Contents
- Enterocyte Metabolism: Why Glutamine Is the Preferred Fuel
- Tight Junction Biology and Amino Acid Substrate Demand
- Bone Broth: Traditional Preparation and Nutrient Profile
- Meat Stock vs Bone Broth (Histamine Considerations)
- Isolated L-Glutamine Supplementation: Dosing and Evidence
- Glycine, Proline, and Collagen Co-Factors
- Marine and Bovine Collagen Peptide Alternatives
- Clinical Applications (IBD, IBS, NSAID Enteropathy, Critical Illness)
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
Enterocyte Metabolism: Why Glutamine Is the Preferred Fuel
Most cells in the body burn glucose for ATP, drawing on the Krebs cycle to oxidize glucose-derived pyruvate. The small intestinal enterocyte is one of a small set of cells (along with lymphocytes and certain renal tubule cells) that preferentially burns glutamine instead. Studies of isolated enterocytes show that glutamine oxidation can account for 60-70% of cellular ATP production in the postabsorptive state, with glucose contributing only 10-15%.
The metabolic logic is partly evolutionary — glutamine is the most abundant amino acid in plasma (~500-700 µmol/L, two to three times the next most abundant), and it is delivered to the gut both via systemic circulation from the basolateral side and via dietary protein digestion at the apical (luminal) surface. The enterocyte can draw substrate from either direction. Glutamine is also a nitrogen donor for purine and pyrimidine synthesis, supporting the rapid DNA replication of the high-turnover crypt stem cells.
The clinical consequence: under conditions of metabolic stress (sepsis, burns, major surgery, chemotherapy, prolonged fasting, severe IBD flare), plasma glutamine becomes a conditionally essential nutrient. Endogenous synthesis from glutamic acid (via glutamine synthetase) cannot keep up with the increased demand from gut, immune cells, and other glutamine-dependent tissues. Plasma glutamine falls, the gut epithelium becomes substrate-starved, and tight junction integrity degrades — producing the well-documented gut barrier failure of critical illness with its endotoxemia, secondary sepsis, and multi-organ dysfunction. This is the rationale behind glutamine-supplemented total parenteral nutrition and enteral feeding formulas in ICU patients.
Tight Junction Biology and Amino Acid Substrate Demand
The intestinal epithelium is a single-cell-thick monolayer of enterocytes, goblet cells, Paneth cells, and enteroendocrine cells, joined laterally by tight junction protein complexes. The tight junction is not a passive seal — it is a dynamic regulator of paracellular permeability built from a structured assembly of transmembrane and cytoplasmic proteins:
- Claudins — a family of ~26 four-transmembrane-domain proteins; claudin composition determines the size and charge selectivity of the paracellular pore. Claudin-1, -3, -4, -5, -7, and -8 are "sealing" claudins; claudin-2 and -10 form leakier pores
- Occludin — another four-transmembrane protein, regulates tight junction permeability and dynamics
- Junctional adhesion molecules (JAM-A, -B, -C) — immunoglobulin-superfamily proteins at the apical junction
- Zonula occludens proteins (ZO-1, ZO-2, ZO-3) — cytoplasmic scaffolding proteins linking the transmembrane claudins/occludin to the actin cytoskeleton
All of these are proteins that must be continuously synthesized from dietary amino acids. The intestinal epithelium turns over every 3-5 days, and the tight junction complex is remodeled in response to physiologic stimuli (cytokines, hormones, microbial signals, mechanical stress) on an even faster timescale. Glutamine specifically has been shown in cell culture and animal models to upregulate claudin-1, occludin, and ZO-1 expression and to reduce paracellular permeability when added to the medium.
In addition to direct synthesis substrate, glutamine donates the amide nitrogen for synthesis of glutathione — the major intracellular antioxidant that protects enterocyte membranes from lipid peroxidation under oxidative stress. Adequate glutamine supports glutathione adequacy, which in turn protects the epithelium from inflammation-driven oxidative damage in IBD and other chronic gut conditions.
Bone Broth: Traditional Preparation and Nutrient Profile
Bone broth is the long-simmered (typically 24-72 hours) extraction of animal bones — beef, pork, lamb, chicken, fish — in water with the addition of acid (apple cider vinegar, lemon juice, white wine) to facilitate calcium and amino acid extraction. The traditional preparation:
- Roast meaty bones (beef knuckle, marrow bones, chicken backs and feet, fish heads and frames) at 400°F for 30-45 minutes to develop flavor and aid extraction
- Place roasted bones in a stock pot or slow cooker, cover with cold water by 2-3 inches, add 1-2 tablespoons of apple cider vinegar per gallon
- Let sit 30-60 minutes before heat to allow acid to begin demineralizing bone
- Bring to a bare simmer (not a rolling boil — this clouds the broth and breaks down flavor), skim foam in the first hour
- Add aromatics (onion, carrot, celery, garlic, peppercorns, bay leaf) in the last 2-4 hours
- Simmer 24-48 hours for chicken; 36-72 hours for beef. Fish broth is the exception — only 30-45 minutes to avoid bitterness
- Strain through fine mesh; refrigerate; skim solidified fat off the top before use
A well-made bone broth will gel firmly when cold — the visible signature of extracted gelatin. Approximate nutrient density per 1-cup (240 mL) serving:
- 6-10 g protein (mostly gelatin / collagen-derived peptides plus free amino acids)
- 1.5-2 g glutamine (free and bound)
- 1-2 g glycine (free and bound)
- 0.5-1 g proline and hydroxyproline (collagen-specific)
- Variable mineral content depending on simmer time and acid: calcium, magnesium, phosphorus, potassium
- Glycosaminoglycans (hyaluronic acid, chondroitin sulfate, glucosamine) from cartilage
The therapeutic intake range for gut healing is typically 1-3 cups per day, often divided between meals or sipped as a warm beverage. In Intro GAPS, broth can be the primary caloric source in Stage 1, contributing 600-1,000 kcal per day from broth alone.
Meat Stock vs Bone Broth (Histamine Considerations)
Long-simmered bone broth is rich in nutrients but also accumulates histamine and tyramine as breakdown products of protein hydrolysis during extended cooking. Patients with histamine intolerance, mast cell activation syndrome, or active inflammatory states often react poorly to bone broth simmered longer than 6-8 hours.
Dr. Natasha Campbell-McBride formally recommends meat stock rather than bone broth for the first stages of GAPS Intro — specifically because of the histamine difference. Meat stock is made from meaty bones with substantial flesh attached (whole chicken, beef shanks with meat, lamb shoulder bones) and simmered only 2-3 hours rather than 24-72 hours. The shorter simmer extracts gelatin and free amino acids while keeping histamine levels lower. Meat stock will still gel modestly when cold, but less firmly than full-simmer bone broth.
For histamine-sensitive patients, the practical workflow is:
- Use meat stock (3-hour simmer max) rather than bone broth
- Cook broth in batches and freeze in single-serving portions immediately — histamine continues to accumulate in refrigerated stock over days
- Consume within 24 hours of thawing; do not let thawed stock sit refrigerated for multiple days
- If symptoms persist, switch to isolated L-glutamine supplementation and gelatin powder (which lacks histamine), bypassing broth altogether
Isolated L-Glutamine Supplementation: Dosing and Evidence
Isolated L-glutamine is available as a flavorless white powder, dosed by the teaspoon (typically ~5 g per teaspoon). It dissolves readily in water, juice, or smoothies and has minimal taste. Pharmaceutical-grade glutamine is heat-stable enough for warm (not boiling) liquid but should not be added to boiling water as heat degrades the amide bond.
Clinical dosing ranges widely depending on indication:
- Maintenance gut support, mild IBS — 5 g/day in divided doses (typically morning and evening on an empty stomach)
- Active IBD, post-infectious IBS, NSAID enteropathy — 10-15 g/day in 2-3 divided doses
- Severe critical illness (clinical research dosing) — 0.3-0.5 g/kg/day, often via parenteral route in ICU
- Pediatric gut healing (under specialist supervision) — 0.1-0.2 g/kg/day
The evidence base for isolated L-glutamine supplementation in gut conditions:
- Zhou et al. (Gut 2018) — randomized placebo-controlled trial of 5 g three times daily L-glutamine for 8 weeks in patients with postinfectious IBS. Significant reduction in lactulose-mannitol gut permeability, normalization of Bristol Stool Form Scale scores, and improvement in symptom severity. This is the strongest single-trial evidence for isolated glutamine in functional gut disease.
- Benjamin et al. (Dig Dis Sci 2012) — randomized trial of glutamine in Crohn's disease. Modest effects on intestinal permeability and clinical activity in the active disease group.
- Wischmeyer et al. (multiple critical care trials) — reduced gut permeability and reduced infection rates in glutamine-supplemented ICU patients.
- van der Hulst et al. (Lancet 1993) — landmark trial showing glutamine-enriched parenteral nutrition preserved gut integrity vs standard TPN in long-term parenteral feeding.
The strongest clinical signal is in postinfectious IBS and in critical-illness gut barrier preservation. Evidence for chronic IBD is positive but more modest. The dose-response appears to plateau above approximately 0.3 g/kg/day — higher doses are not clearly more effective.
Glycine, Proline, and Collagen Co-Factors
While glutamine gets the most attention, the other amino acids concentrated in bone broth and collagen also matter for gut healing. Glycine (the smallest amino acid, ~30% of collagen by weight) is a primary substrate for glutathione synthesis (alongside cysteine and glutamate), is an inhibitory neurotransmitter that supports sleep and reduces anxiety, and is the amino acid most depleted by chronic stress and inflammation. Proline and its hydroxylated derivative hydroxyproline are collagen-specific amino acids that the body uses to rebuild the connective tissue scaffolding of the gut wall.
Glycine has emerged in recent nutrition research as a likely conditionally essential amino acid — endogenous synthesis appears inadequate to meet collagen synthesis demand in many adults consuming typical Western diets. The free glycine in bone broth (~1-2 g per cup) plus the gelatin-bound glycine extracted from collagen contributes 3-5 g per cup. Isolated glycine powder is inexpensive, slightly sweet, and easily added to coffee, tea, or smoothies (typical dose 3-10 g/day).
Vitamin C is the required cofactor for the hydroxylation of proline and lysine residues in collagen synthesis. Without adequate Vitamin C, newly synthesized collagen is structurally defective — the classic scurvy presentation. Most patients on a basic gut-healing protocol get adequate Vitamin C from non-starchy vegetables and small amounts of allowed fruit, but a supplemental dose of 500-1,000 mg/day is reasonable insurance during active gut repair.
Marine and Bovine Collagen Peptide Alternatives
Hydrolyzed collagen peptides (sold as Vital Proteins, Great Lakes Wellness, Sports Research, Further Food, and many other brands) are bone-broth nutrition in convenient powder form. Collagen is extracted from cow hides (bovine) or fish skin and scales (marine), partially hydrolyzed into shorter peptide fragments and free amino acids, and spray-dried to a flavorless powder.
Approximate amino acid profile per 20 g serving of hydrolyzed bovine collagen:
- ~18 g protein
- 5-6 g glycine
- 2.5-3 g proline
- 2.5-3 g hydroxyproline
- ~1 g glutamine/glutamic acid (much less than bone broth or isolated glutamine)
The trade-off: collagen peptides deliver concentrated glycine and proline (better than bone broth on a per-gram-protein basis) but much less glutamine. For optimal gut healing, the practical combination is collagen peptides + isolated glutamine + occasional bone broth, or bone broth as the primary base supplemented with isolated glutamine for higher dosing.
Marine collagen has slightly higher bioavailability in some studies but is more expensive. Bovine collagen sourced from grass-fed cattle is the most cost-effective option for daily use. Patients with shellfish allergy should specifically verify marine collagen source (most is from white fish skin, but some is from shellfish-derived sources).
Clinical Applications (IBD, IBS, NSAID Enteropathy, Critical Illness)
- Postinfectious IBS — the strongest clinical signal. After acute gastroenteritis (Norovirus, Salmonella, Campylobacter, Giardia), a subset of patients develop persistent diarrhea, urgency, and bloating that meet criteria for IBS-D. Glutamine 5 g three times daily for 8 weeks has Level 1 evidence (Zhou 2018) for normalizing gut permeability and symptoms in this population.
- Inflammatory bowel disease (Crohn's, ulcerative colitis) — bone broth and glutamine are reasonable adjuncts to conventional therapy. The evidence base is modest but consistent. Use as part of comprehensive gut healing including dietary modification, probiotic strain selection, and trigger avoidance.
- NSAID enteropathy — chronic NSAID use (ibuprofen, naproxen, aspirin) damages the small intestinal mucosa in approximately 70% of chronic users (capsule endoscopy studies). Glutamine and bone broth help repair the damage, but trigger removal is the necessary first step (see Avoiding Triggers page).
- Critical illness / ICU patients — glutamine-supplemented enteral or parenteral nutrition is part of standard ICU nutrition support in many settings. Reduces infection rates, gut barrier failure, and hospital length of stay.
- Athletes with exercise-induced gut permeability — long-duration endurance exercise (marathons, ultramarathons) produces transient gut barrier dysfunction with endotoxemia. Glutamine 10 g before and after long efforts is commonly used among endurance athletes; small studies show reduction in markers of gut permeability.
- Post-bariatric surgery — gastric bypass patients have altered amino acid digestion and absorption; bone broth and free amino acids may be useful adjuncts in the post-operative healing period.
- Cancer patients on chemotherapy — chemotherapy-induced mucositis (of the gut and oral cavity) responds modestly to glutamine supplementation; this is the basis for swish-and-swallow glutamine protocols in oncology nursing.
- Chronic SIBO — bone broth and glutamine support gut barrier repair after antibiotic or herbal antimicrobial protocols. See the dedicated SIBO page for the broader protocol.
Cautions and Contraindications
- Histamine intolerance / mast cell activation syndrome — long-simmered bone broth is high in histamine and tyramine. Use meat stock (3-hour simmer max), freeze in single portions, or substitute isolated glutamine + collagen peptides.
- Bipolar disorder or seizure history — high-dose glutamine (above 20-30 g/day) has been anecdotally associated with mood destabilization or seizure activity, presumably through conversion to glutamate. Patients with bipolar disorder, seizure disorder, or significant anxiety should start at low dose and avoid the very high doses sometimes used in athletic protocols.
- Hepatic encephalopathy — in advanced liver disease, the urea cycle is impaired and glutamine breakdown produces ammonia. High-dose glutamine in hepatic encephalopathy can worsen the encephalopathy. Avoid in advanced cirrhosis.
- Renal failure — standard general-protein-restriction cautions apply. Discuss with nephrology before adding significant supplemental glutamine.
- Heavy metal concentration in bone broth — concerns have been raised about lead concentration in bone broth from conventionally raised livestock. Studies are mixed; the absolute lead content of well-made bone broth from grass-fed cattle is generally low. Source from clean providers (grass-fed, pasture-raised, ideally with USDA Organic certification) particularly if consuming daily long-term.
- Glutamate sensitivity — a small subset of patients are sensitive to glutamate (the deamidated metabolite of glutamine) and report headaches or neurological symptoms with high-dose glutamine. Reduce dose or discontinue.
- Pregnancy — bone broth is generally considered safe and beneficial in pregnancy. Isolated high-dose L-glutamine supplementation in pregnancy lacks formal safety data; conservative dosing only under specialist guidance.
Key Research Papers
- Zhou Q et al. (2018). Randomised placebo-controlled trial of dietary glutamine supplements for postinfectious irritable bowel syndrome. Gut. — PubMed
- van der Hulst RR et al. (1993). Glutamine and the preservation of gut integrity. Lancet. — PubMed
- Wischmeyer PE et al. (2014). Parenteral glutamine supplementation in critical illness: a systematic review. Crit Care. — PubMed
- Rao R, Samak G (2012). Role of glutamine in protection of intestinal epithelial tight junctions. J Epithel Biol Pharmacol. — PubMed
- Benjamin J et al. (2012). Glutamine and whey protein improve intestinal permeability and morphology in patients with Crohn's disease. Dig Dis Sci. — PubMed
- Newsholme P (2001). Why is L-glutamine metabolism important to cells of the immune system. J Nutr. — PubMed
- Wang B et al. (2015). Glutamine and intestinal barrier function. Amino Acids. — PubMed
- Achamrah N et al. (2017). Glutamine and the regulation of intestinal permeability: from bench to bedside. Curr Opin Clin Nutr Metab Care. — PubMed
- Li N et al. (2004). Glutamine deprivation alters intestinal tight junctions via a PI3-K/Akt mediated pathway in Caco-2 cells. J Nutr. — PubMed
- Coqueiro AY et al. (2019). Glutamine as an anti-fatigue amino acid in sports nutrition. Nutrients. — PubMed
- Daly JM et al. (1992). Enteral nutrition with supplemental arginine, RNA, and omega-3 fatty acids in patients after operation. Surgery. — PubMed
- Hou Y et al. (2017). Composition of human collagen peptides and intestinal absorption. J Agric Food Chem. — PubMed
PubMed Topic Searches
- PubMed: Glutamine and tight junctions
- PubMed: Bone broth composition
- PubMed: Collagen peptide clinical trials
- PubMed: Glycine and glutathione
- PubMed: Glutamine in critical care
Connections
- Gut Healing Overview
- Gut Healing Benefits Hub
- GAPS Diet
- Probiotic Strains for Repair
- Avoiding Triggers
- Glutamine
- Glycine
- Proline
- Bone Broth
- Irritable Bowel Syndrome
- Crohn's Disease
- SIBO
- Vitamin C (Collagen Cofactor)
- Organ Meats
- Immune Boosting