Gerson Therapy — Juicing Protocol
The juicing protocol is the caloric and micronutrient backbone of the Gerson Therapy. Thirteen 8-ounce glasses of fresh raw juice per day — carrot, apple, mixed green leaf, and Gerson's signature "green juice" of romaine, endive, watercress, beet tops, red cabbage, green pepper, and apple — delivered every hour during waking hours. Gerson insisted on a two-stage press juicer (the Norwalk being the iconic example) rather than a centrifugal juicer, on the argument that grinding-then-pressing minimizes oxidation and preserves polyphenols that high-speed centrifugal blades destroy. This page walks through the protocol's structure, the published evidence for and against the high-volume juicing argument, the practical realities of preparing 13 glasses per day, and the mainstream nutritional view of where the protocol overlaps with established science (it does, substantially) and where it diverges (where the dose claim outruns the evidence).
Table of Contents
- The Thirteen Glasses — Composition and Schedule
- Press vs Centrifugal Juicer — The Oxidation Argument
- Carrot-Apple Juice — Beta-Carotene and Polyphenol Load
- The "Green Juice" — Nitrate, Folate, and Sulforaphane
- The Calf-Liver Juice Historical Component (Discontinued)
- The Dose-Response Claim and Its Mainstream Counter
- Glycemic Load, Dental Erosion, and Other Practical Concerns
- Preparation Logistics — What 13 Glasses a Day Actually Looks Like
- Key Research Papers
- Connections
- Featured Videos
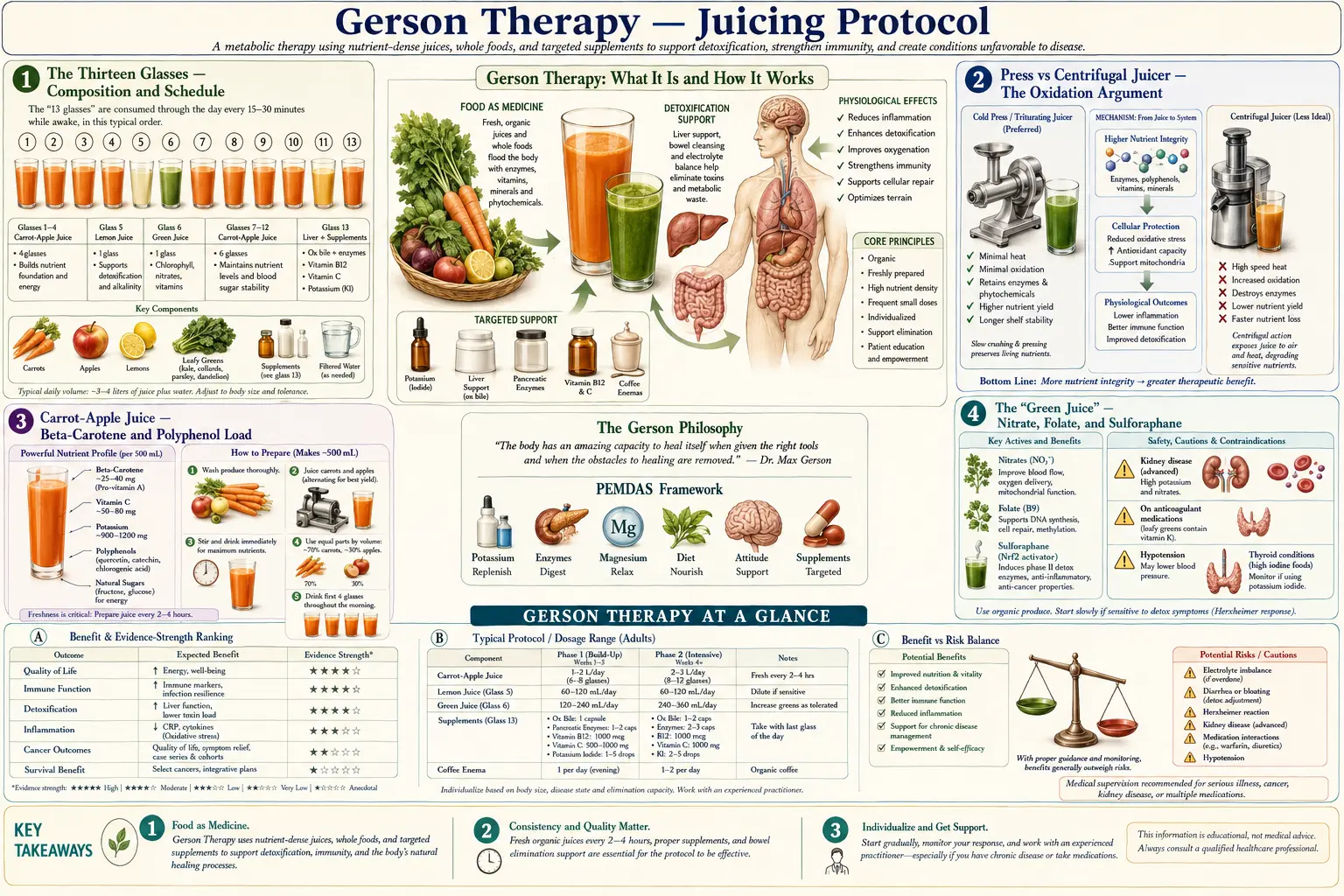
The Thirteen Glasses — Composition and Schedule
The original Gerson juicing schedule, as set out in Max Gerson's 1958 monograph A Cancer Therapy: Results of Fifty Cases, prescribes 13 8-ounce glasses of freshly prepared juice per day, taken approximately every hour during waking hours. The schedule is intentionally distributed: a juice with breakfast, one between breakfast and lunch, juice with lunch, juices between meals, juices through the afternoon, with the last glass typically at 7 PM.
The composition by glass count is the same in modern protocols followed by the Gerson Institute and the licensed Gerson clinics in Tijuana and Hungary:
- 5 glasses carrot-apple juice — the largest single component, typically 60% carrot and 40% apple by volume. Apple is included primarily for palatability and pectin, secondarily for polyphenols.
- 3 glasses straight carrot juice — the highest beta-carotene density component, traditionally argued to deliver hepatoprotective and pro-vitamin-A signaling.
- 4 glasses green juice — a mixed press of romaine, endive, watercress, red cabbage, beet tops, green pepper, with one quarter of a Granny Smith apple. This is the highest folate, nitrate, and chlorophyll-density component.
- 1 glass orange juice — only at breakfast; phased out in patients with active diarrhea or where blood glucose is a concern.
The total daily fluid load from juice alone is approximately 3 liters. Combined with the prescribed water, soup, and additional cooked-vegetable intake, total fluid load is substantial. The protocol is calorie-rich (~2,400–2,800 kcal/day from juice plus solid food), high-carbohydrate (~70% energy), low-fat (~10% energy), and essentially zero-sodium until salt is gradually re-introduced after several months.
The schedule is the operational core of the protocol. Patients who attempt the diet without the hourly juicing discipline typically describe it as ineffective; clinic-treated patients describe the hourly schedule as the single most demanding feature of the protocol — harder to maintain than the coffee enemas, the food restrictions, or the supplements.
Press vs Centrifugal Juicer — The Oxidation Argument
Gerson's requirement of a two-stage grinder-and-press juicer (rather than a centrifugal juicer) is one of the protocol's most-cited mechanical claims. The Norwalk juicer, invented in 1934, is the iconic example: vegetables are first ground into a fibrous pulp, then the pulp is wrapped in a cotton press cloth and squeezed under hydraulic pressure to extract juice.
The proponent argument is that centrifugal juicers, which spin shredded pulp at high RPM against a mesh screen, introduce three sources of polyphenol and enzyme loss:
- Oxygen entrainment — the high-speed spinning incorporates air into the juice, accelerating oxidation of polyphenols (visible as rapid browning of apple, pear, or leafy-green juice).
- Friction heat — the blade-screen interface generates thermal energy that denatures heat-labile enzymes and degrades some vitamin C and B-complex vitamins.
- Mechanical cell-wall shearing — produces less complete extraction from leafy greens (which a press handles well) and produces a different polyphenol profile.
Independent measurements have partially validated and partially complicated this argument. Press-style juicers do produce juice with measurably higher antioxidant activity (ORAC) immediately after extraction, and the difference is most pronounced for leafy greens and cruciferous vegetables. However, the difference for hard root vegetables like carrot is modest. And the practical importance of the polyphenol-preservation difference at the clinical-outcome level (rather than the test-tube level) has not been established by any randomized trial.
The mainstream nutritional view is that the press-vs-centrifugal distinction is real but small, that immediate consumption matters more than juicer type (oxidation continues post-extraction), and that the same micronutrient profile can be delivered by either device with reasonable fidelity. The Gerson Institute disagrees and continues to require the Norwalk (or equivalent two-stage press) for patients enrolling at its licensed clinics.
Carrot-Apple Juice — Beta-Carotene and Polyphenol Load
The five daily glasses of carrot-apple juice are the dominant single contributor to the protocol's beta-carotene, polyphenol, and potassium load. Quantitatively, 8 ounces of fresh-pressed carrot-apple juice (60/40) provides approximately:
- 15,000–20,000 mcg beta-carotene (equivalent to ~1,250–1,650 mcg RAE Vitamin A activity after BCMO1 conversion at the standard 1:12 ratio)
- 500–700 mg potassium
- ~80 mg vitamin C
- ~30 mcg folate
- ~25 g sugar (approximately one-third sucrose, two-thirds fructose-glucose)
- polyphenol load dominated by chlorogenic acid (from apple) and falcarinol/falcarindiol (from carrot)
Across the five-glass daily intake, the totals reach 75,000–100,000 mcg beta-carotene (~6,250–8,330 mcg RAE), 2,500–3,500 mg potassium, ~400 mg vitamin C, and ~125 g sugar from this component alone. The Vitamin A delivery is several times the RDA, and the safety margin is preserved because beta-carotene conversion to retinol is downregulated by BCMO1 feedback — the body simply stops converting once tissue retinol is replete. Adverse effects from beta-carotene overload are limited to carotenodermia (harmless orange-yellow palm and sole pigmentation, fully reversible) and the documented ATBC/CARET signal of increased lung cancer risk in smokers given isolated synthetic beta-carotene (a different molecule from the food-matrix carotenoid mix in juice).
The polyphenol load from chlorogenic acid is substantial and overlaps the apple-polyphenol literature on insulin sensitivity, endothelial function, and weak AMPK activation. The falcarinol family of polyacetylenes in carrot has been studied in cell-culture and rodent models for chemopreventive activity against colon cancer; human evidence remains limited but mechanistically interesting.
The "Green Juice" — Nitrate, Folate, and Sulforaphane
The four glasses of green juice per day deliver a profile that overlaps closely with the modern mainstream science on leafy-green vegetables, beetroot, and cruciferous intake — arguably the single component of the Gerson protocol with the strongest mainstream support, though the dose far exceeds typical dietary recommendations.
An 8-ounce glass of the canonical Gerson green juice (romaine, endive, watercress, beet tops, red cabbage, green pepper, with a quarter apple) provides approximately:
- 200–400 mg dietary nitrate (substantial proportion from beet tops; the rest from leafy greens)
- 150–250 mcg folate
- 200–400 mg potassium
- ~50 mg vitamin C
- ~150 mg calcium
- variable sulforaphane / glucoraphanin from the red cabbage and watercress fractions
- chlorophyll, lutein, and zeaxanthin in concentrated form
The nitrate load alone is clinically interesting. Across the four-glass daily intake, total dietary nitrate approaches 1,000–1,500 mg per day — comparable to the highest-nitrate experimental diets used in endothelial-function and blood-pressure studies. Dietary nitrate is enzymatically reduced (oral microbiome to nitrite, then gastric reduction to nitric oxide) and contributes to vasodilation, improved exercise tolerance, and modest reduction in blood pressure. The blood-pressure-lowering effect is well-established in randomized trials and explains part of the cardiovascular benefit associated with the DASH diet, Mediterranean diet, and dietary patterns rich in leafy greens.
The sulforaphane and isothiocyanate fraction from cruciferous components activates the NRF2 transcription factor, inducing Phase II detoxification enzymes including NQO1, HO-1, and the glutathione-S-transferase family. This is a mainstream-accepted chemopreventive mechanism studied in detail by Talalay, Fahey, and others at Johns Hopkins.
The folate density per glass is also notable. At 600–1,000 mcg folate per day from green juice alone, the protocol delivers folate well above the RDA and into the range where some clinicians caution about masking B12 deficiency (a real concern in a near-vegan protocol, addressed by Gerson's required B12 injections).
The Calf-Liver Juice Historical Component (Discontinued)
For historical accuracy: the original 1950s Gerson protocol included raw calf-liver juice, prepared by pressing fresh organic calf liver and consumed for its dense iron, copper, B12, retinol, and choline content. This component was discontinued by the Gerson Institute in 1989 after a campylobacter outbreak traced to contaminated liver caused several cases of severe infection in clinic patients.
The replacement protocol substitutes oral B12 (usually injectable hydroxocobalamin) and Lugol's iodine for the thyroid/iodine fraction that the liver had provided, along with desiccated bovine thyroid extract for the hormonal component. Some modern Gerson-aligned protocols re-introduce small amounts of grass-fed beef liver (typically as freeze-dried desiccated capsules rather than raw juice) for the same nutritional profile without the bacterial contamination risk.
The liver-juice discontinuation is worth knowing for two reasons. First, modern proponent organizations often present the protocol as if it has always been plant-only; the historical record is more complicated. Second, the discontinuation demonstrates that the Gerson Institute has, at least once, made a substantive protocol modification in response to documented safety harm — a useful counterweight to the more common critique that the protocol has been frozen since 1958.
The Dose-Response Claim and Its Mainstream Counter
The single most important argument between Gerson proponents and mainstream nutritionists is the dose-response claim. Proponents argue that the therapeutic effect comes from delivering vegetable micronutrients at a dose that is simply unreachable through normal whole-food eating — 5–7 pounds of carrots, several heads of romaine and red cabbage, dozens of apples per day. The juicing format compresses the equivalent of an entire produce aisle into a drinkable form.
The mainstream counter is that:
- The active ingredients (carotenoids, polyphenols, nitrate, sulforaphane, potassium) follow saturable absorption and saturable signaling. Once tissue concentrations reach the plateau of the dose-response curve, additional intake produces no additional benefit.
- Many of the polyphenols have low oral bioavailability (1–5% for most flavonoids), and the rate-limiting step is intestinal absorption and Phase II conjugation in the gut wall, not delivered dose. Juicing does not bypass this constraint.
- The fiber stripped away by juicing has independently documented benefit for the gut microbiome, blood glucose, and colon cancer risk. Replacing whole vegetables with their juiced equivalent removes that benefit.
- Whole-food vegetable diets with 7–10 servings per day (the DASH or Mediterranean upper range) capture most of the micronutrient benefit without the time, dental, or glycemic cost.
The honest middle position is that the high-juice protocol does deliver micronutrients at concentrations difficult to reach otherwise, that some of those concentrations probably do confer clinical benefit (the nitrate-blood-pressure effect, the sulforaphane-NRF2 effect, the potassium-stroke effect), and that the marginal benefit beyond what a well-constructed whole-vegetable diet delivers is unproven. Whether the marginal benefit is large enough to justify the protocol's operational cost is the legitimate disagreement.
Glycemic Load, Dental Erosion, and Other Practical Concerns
The juicing protocol carries three well-documented downside considerations that mainstream nutritionists raise consistently.
Glycemic load. Even pressed vegetable juice (without added fruit) elevates blood glucose more sharply than the whole-food equivalent because fiber removal removes the rate-limiting brake on sugar absorption. With apple included (Gerson's carrot-apple ratio is 60/40), the per-glass glycemic load is meaningful, and across 13 glasses per day the chronic glycemic challenge is substantial. The protocol is generally contraindicated in patients with poorly controlled type 2 diabetes for this reason.
Dental erosion. Repeated daily exposure of tooth enamel to acidic juice (apple pH 3.5; orange juice pH 3.5; mixed green juice pH 5–6) over months and years causes documented enamel erosion. The Gerson Institute's guidance is to drink through a straw, rinse with water immediately after each glass, and not brush for at least 30 minutes after drinking (to avoid mechanically scrubbing softened enamel). Patients on the protocol for years should be monitored by a dentist.
Time and ingredient cost. Strict adherence to the 13-glass daily schedule requires approximately 4–6 hours per day of food preparation when the cook is fast and equipped. The ingredient cost is also substantial — the Gerson Institute estimates 7–10 pounds of organic carrots, several heads of organic romaine and cabbage, several pounds of organic apples, and various supporting greens per patient per day. The protocol is largely impractical without dedicated caregiver labor or full-stay residence at a Gerson clinic.
None of these concerns is a refutation of the protocol's underlying nutritional logic. They are operational facts that any patient considering the protocol should know going in.
Preparation Logistics — What 13 Glasses a Day Actually Looks Like
Realism about logistics is important. A typical day on the Gerson juicing protocol involves:
- 7:00 AM — first glass (orange or grapefruit juice); breakfast preparation begins
- 8:00 AM — breakfast plus a glass of carrot-apple juice
- 9:00 AM — green juice (freshly pressed)
- 10:00 AM — carrot-apple juice
- 11:00 AM — straight carrot juice
- 12:00 PM — lunch plus green juice
- 1:00 PM — carrot-apple juice
- 2:00 PM — green juice
- 3:00 PM — straight carrot juice
- 4:00 PM — carrot-apple juice
- 5:00 PM — green juice
- 6:00 PM — dinner plus carrot-apple juice
- 7:00 PM — straight carrot juice (final glass)
Each glass must be freshly prepared — Gerson's explicit instruction is that juice should be consumed within minutes of pressing, never stored even briefly. (Modern proponents allow up to 20–30 minutes if necessary, but the freshness mandate is core.) For a household running the full protocol, this typically means juicing every hour during waking hours, which is why the protocol is most commonly attempted with dedicated caregiver support or at residential clinic.
The Gerson Institute's published guidance acknowledges this and recommends that home-based protocol attempts include either: (a) full-time caregiver support, (b) a kitchen organization that pre-stages and pre-washes produce by the meal-cycle's worth, and (c) prior 2–3 week residential training at one of the licensed clinics in Tijuana or Hungary to learn the technique. Without those supports, dropout rates are high.
Key Research Papers
- Norwalk-style press juicing and polyphenol preservation versus centrifugal extraction — PubMed: Press vs centrifugal
- Carrot juice beta-carotene and serum response — PubMed: Carrot juice serum
- Dietary nitrate from leafy greens and beetroot — blood pressure effect — PubMed: Nitrate and blood pressure
- Sulforaphane and NRF2 activation: Talalay / Fahey Johns Hopkins work — PubMed: Talalay sulforaphane NRF2
- Apple polyphenols (chlorogenic acid, quercetin) and insulin sensitivity — PubMed: Apple polyphenols
- Falcarinol and polyacetylenes from carrot — chemopreventive activity — PubMed: Falcarinol chemoprevention
- Fruit and vegetable intake and cancer incidence — EPIC cohort — PubMed: EPIC fruit/vegetable
- Juice fasting and short-term microbiome / metabolic effects — PubMed: Juice fast microbiome
- Concentrated fruit juice and dental enamel erosion — PubMed: Juice dental erosion
- Glycemic response to vegetable juice versus whole vegetable — PubMed: Juice vs whole glycemic
- BCMO1 polymorphism and beta-carotene conversion variability — PubMed: BCMO1 polymorphism
- Folate and B12 interaction — masking risk in high-folate diets — PubMed: Folate-B12 masking
Connections
- Benefits Deep Dive Hub
- Coffee Enema Component
- Mineral Density and Sodium-Potassium
- Documentary Evidence and Critique
- Gerson Therapy Main Hub
- Gerson Juicing Overview
- Gerson Juicing Recipes
- Gerson Diet Protocol
- Celery Juice (Anthony William)
- Anti-Inflammatory Diet
- Carrots
- Kale
- Vitamin A
- Potassium