Vagal Tone and HRV — Resonance Breathing and Autonomic Balance
Heart-rate variability (HRV) is the beat-to-beat variation in the interval between consecutive heartbeats. Despite the colloquial image of the heart as a metronome, the healthy heart never beats at a perfectly fixed interval — the spaces between beats expand and contract with respiration, baroreflex activity, and autonomic tone. HRV is the single best non-invasive biomarker of autonomic balance, has documented prognostic value in cardiovascular disease and post-MI mortality, and is the foundation of the modern field of HRV biofeedback. Resonance-frequency breathing — typically around 5.5 to 6 breaths per minute — maximizes HRV amplitude, strengthens vagal tone, and produces measurable improvements in anxiety, blood pressure, and cognitive performance. This page documents the physiology of vagal tone, the polyvagal model, HRV measurement, resonance breathing protocols, and the clinical evidence base.
Table of Contents
- What Is Vagal Tone
- HRV Physiology — Respiratory Sinus Arrhythmia
- HRV Metrics — RMSSD, HF, SDNN, and Coherence
- The Polyvagal Model (Porges)
- Resonance Frequency — The 5.5 Breaths Per Minute Sweet Spot
- HRV Biofeedback — The Lehrer Protocol
- How to Measure HRV (Devices and Methods)
- Clinical Evidence — Anxiety, Hypertension, Performance, Longevity
- What Affects Vagal Tone Beyond Breathing
- Cautions and Interpretation Pitfalls
- Key Research Papers
- Connections
- Featured Videos
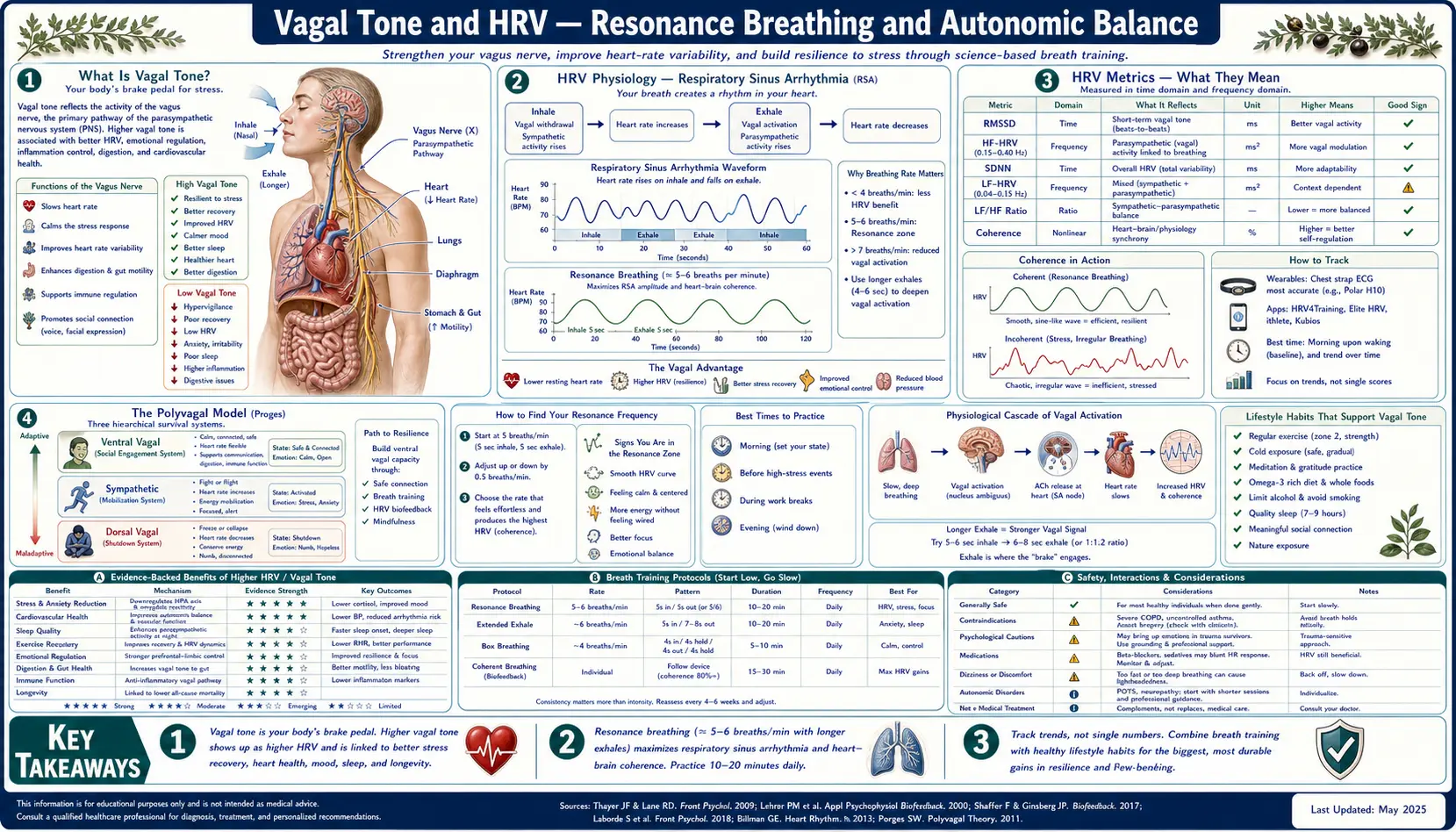
What Is Vagal Tone
The vagus nerve (cranial nerve X) is the principal parasympathetic nerve of the body. It originates in the medulla oblongata and innervates the heart, lungs, gastrointestinal tract down to the splenic flexure, liver, pancreas, kidneys, larynx, and several other structures. "Vagal tone" refers to the steady tonic firing of this nerve onto its targets, with high vagal tone signaling a body in homeostatic, parasympathetic-dominant, "rest and digest" mode and low vagal tone signaling a body in chronic sympathetic activation, stress, or autonomic dysfunction.
Vagal tone has been linked in epidemiological studies to:
- All-cause mortality — lower vagal tone (measured as HRV) is associated with higher mortality independent of other risk factors
- Cardiovascular mortality — the Framingham Heart Study and subsequent cohorts documented that low HRV predicts cardiac death
- Sudden cardiac death after myocardial infarction — the foundational use case for HRV measurement in cardiology
- Diabetes mellitus — cardiovascular autonomic neuropathy (low HRV) is an early marker
- Depression and anxiety disorders — both are associated with reduced HRV
- Cognitive function — higher resting HRV correlates with better executive function and prefrontal cortex thickness
- Inflammation — lower vagal tone is associated with higher CRP, IL-6, and TNF-alpha through the cholinergic anti-inflammatory pathway
The Tracey 2002 Nature paper (PMID 12490960) established the vagus nerve as the principal anti-inflammatory neural circuit through the cholinergic anti-inflammatory pathway — vagal acetylcholine release at the spleen activates alpha-7 nicotinic acetylcholine receptors on macrophages and suppresses NF-kappaB-driven cytokine production. This is the mechanism by which vagal tone has systemic anti-inflammatory effects.
HRV Physiology — Respiratory Sinus Arrhythmia
The most prominent contributor to short-term HRV is respiratory sinus arrhythmia (RSA) — the rhythmic acceleration of heart rate during inspiration and deceleration during expiration. This is not noise; it is a regulated physiological pattern with both efficiency and homeostatic functions:
- During inspiration, intrathoracic pressure drops, venous return increases, and stroke volume momentarily rises. Heart rate increases to push the higher volume forward.
- During expiration, the opposite occurs. Heart rate slows to match the reduced preload.
- RSA matches alveolar ventilation to pulmonary perfusion across the breath cycle, improving ventilation-perfusion (V/Q) matching and gas exchange efficiency by an estimated 5-10%.
- RSA amplitude is a direct readout of vagal (parasympathetic) tone — the vagus nerve is what slows the heart on expiration. Without vagal innervation (e.g., heart transplant patients), RSA disappears.
The amplitude of RSA depends on breath rate. At rapid shallow breathing (15-20 breaths per minute, the modern desk-worker default), RSA is suppressed because the breath cycle is too fast for the vagal arc to fully respond. At slow deep breathing (5-7 breaths per minute), RSA is amplified to maximum, with peak-to-trough heart rate swings of 20-40 bpm observable on a continuous HRV trace.
This is the reason slow breathing has such reliable autonomic effects: the slow breath rate aligns with the latency of the baroreceptor reflex arc and the cardiac vagal response time, producing a coherent, resonantly amplified oscillation.
HRV Metrics — RMSSD, HF, SDNN, and Coherence
Several different mathematical measures are used to quantify HRV, each capturing a different aspect:
- RMSSD (root mean square of successive differences) — the most-used short-term HRV metric. The standard deviation of beat-to-beat interval differences. Reflects high-frequency (vagally mediated) variability. Standard measurement window: 5 minutes at rest, or overnight. Typical adult values: 30-60 ms. Trends matter more than absolute numbers.
- HF-HRV (high-frequency power, 0.15-0.4 Hz) — the frequency-domain equivalent of RMSSD. Direct measure of parasympathetic / vagal tone. Reported in ms2.
- LF-HRV (low-frequency power, 0.04-0.15 Hz) — reflects both sympathetic and baroreflex activity. Often reported as the LF/HF ratio (a marker of sympathovagal balance, though this interpretation is contested).
- SDNN (standard deviation of NN intervals) — the standard deviation of all R-R intervals over a measurement window. Reflects total variability, not specifically vagal. Useful for 24-hour Holter recordings.
- pNN50 — percentage of successive interval differences greater than 50 ms. Correlates strongly with RMSSD; reflects vagal tone.
- Coherence ratio — the HeartMath-specific metric, capturing the proportion of HRV power concentrated at the resonance frequency (around 0.1 Hz). Higher coherence indicates entrained resonant breathing.
The Shaffer and Ginsberg 2017 Frontiers in Public Health overview (PMID 29034226) provides the authoritative reference summary of HRV metrics, normative values, and measurement methods. For practical use, RMSSD measured each morning on a consumer wearable is sufficient for tracking individual training response over weeks.
The Polyvagal Model (Porges)
Stephen Porges's polyvagal theory (formalized in his 2007 Biological Psychology paper, PMID 17049418) reframes the vagus nerve not as a single anti-stress system but as a three-tier autonomic hierarchy with distinct evolutionary origins:
- Ventral vagal complex (the "social engagement" system) — the youngest evolutionary layer, mammalian-specific. The myelinated ventral vagal branch innervates the heart, larynx, pharynx, and facial muscles. When active, supports social engagement, calm cardiac function, vocal prosody, facial expressiveness, eye contact, and middle-ear sensitivity for human voice frequencies. This is the "safe and connected" state.
- Sympathetic nervous system — the older evolutionary layer, the fight-or-flight mobilization system. Activated when safety cues are absent or threat is detected. Increases heart rate, blood pressure, respiration, glucose mobilization.
- Dorsal vagal complex (the immobilization system) — the oldest evolutionary layer, shared with reptiles. The unmyelinated dorsal vagal branch produces freeze, faint, dissociation, conservation withdrawal. Activated under inescapable life threat. Drops heart rate, blood pressure, metabolic rate.
The clinical implication of polyvagal theory is that the goal of autonomic regulation is not simply "reduce sympathetic, increase parasympathetic" — because the dorsal vagal state is also parasympathetic but is the freeze state, not the calm state. The goal is access to the ventral vagal "safe and connected" state.
Practical applications of polyvagal-informed practices include:
- Slow deep breathing with extended exhale — engages ventral vagal
- Humming, chanting, gargling, singing — directly activate ventral vagal innervation of the larynx
- Cold-water face immersion — activates the diving reflex via the trigeminal-vagal pathway
- Eye-contact and social warmth — the polyvagal-favored stimulus for ventral vagal activation
- Body movement and physical exercise — sequentially shifts through sympathetic activation to parasympathetic recovery, training autonomic flexibility
Resonance Frequency — The 5.5 Breaths Per Minute Sweet Spot
The Vaschillo 2006 study (PMID 16838124) established the modern concept of cardiovascular resonance frequency in HRV biofeedback. The key findings:
- Every individual has a specific breathing frequency at which their HRV oscillation reaches maximum amplitude.
- For most adults this resonance frequency is between 4.5 and 6.5 breaths per minute.
- The resonance frequency is determined by individual anatomy — tall individuals tend to have lower resonance frequencies (slower required breath rate), short individuals higher.
- Breathing at the resonance frequency for sustained periods produces measurably larger autonomic and clinical effects than breathing at neighboring frequencies.
The practical resonance-frequency breathing protocol:
- Sit upright. Optional: connect a HRV biofeedback device (Polar H10 with HRV4Training app, EmWave Pro, or similar).
- Begin breathing at 6 breaths per minute (5-second inhale, 5-second exhale, no holds). This is the median resonance frequency.
- If a biofeedback device is available, monitor HRV amplitude. Adjust breath rate up or down by 0.5 breaths per minute to find the rate that produces maximum HRV amplitude. That rate is your personal resonance frequency.
- Without a device, 5.5 breaths per minute (5.5-second inhale, 5.5-second exhale) is a reasonable starting estimate for most adults.
- Practice at your resonance frequency for 10-20 minutes once or twice daily.
The Steffen 2017 Frontiers in Public Health study (PMID 28890890) found that just one session of resonance-frequency breathing improved HRV measures, lowered blood pressure, and improved mood compared to control conditions.
HRV Biofeedback — The Lehrer Protocol
HRV biofeedback (HRVB) is the structured clinical application of resonance-frequency breathing with real-time feedback. The protocol was developed largely by Paul Lehrer (Rutgers) and Richard Gevirtz (Alliant International) and is sometimes called "The Lehrer Protocol." Standard structure:
- Session 1 — resonance frequency assessment. The patient breathes at 6.5, 6, 5.5, 5, and 4.5 breaths per minute for several minutes each while connected to an HRV biofeedback device. The frequency producing maximum LF-power and peak-to-trough heart rate swing is identified as the patient's personal resonance frequency.
- Sessions 2-10 — the patient practices breathing at their resonance frequency, typically for 20-minute clinic sessions plus 20-minute daily home practice with a portable device or app.
- Outcome measures — HRV amplitude at baseline (off-protocol breathing) is tracked across weeks. The training adaptation is increased baseline parasympathetic tone, not just acute session effect.
The Lehrer 2003 Psychosomatic Medicine study (PMID 12883107) was foundational, demonstrating that HRVB training increased baroreflex gain and peak expiratory flow. Subsequent meta-analyses (Goessl 2017, PMID 28478782; Pagaduan 2019, PMID 31309366) have established efficacy in anxiety, sport performance, depression, and stress-related disorders.
How to Measure HRV (Devices and Methods)
Practical options for measuring HRV outside the laboratory:
- Chest-strap ECG (Polar H10, Wahoo TICKR X) — the gold standard for consumer use. R-R interval accuracy approaches laboratory ECG. Pairs with apps (HRV4Training, Elite HRV, EliteHRV, Polar Flow). Best option for serious tracking. ~$80-100.
- Optical photoplethysmography (PPG) wearables — Apple Watch, Garmin, Fitbit, Oura Ring, Whoop. Optical sensors detect pulse rather than electrical heart activity. Accuracy is reasonable for nighttime measurement during sleep (when motion artifact is minimal), poor during exercise or daytime activity. Most consumer fitness wearables now report nightly HRV.
- Smartphone camera apps (HRV4Training Camera, Welltory) — use the phone's camera flash and lens against fingertip to detect pulse. Reasonable accuracy for morning baseline measurement.
- Dedicated HRV biofeedback devices (HeartMath emWave Pro, Mind Media NeXus) — designed specifically for biofeedback training. Best option for HRVB clinical training.
Recommended measurement protocol for individual tracking:
- Same time each day — first thing in the morning, before getting out of bed, before coffee.
- Same posture — supine or seated, consistently.
- 5 minutes of quiet breathing without intervention — this is your baseline. Do not breathe at resonance frequency during measurement, as this artificially inflates HRV.
- Track the 7-day rolling average — individual days vary substantially based on sleep quality, alcohol intake, prior-day training load, hormonal cycle.
- Look for trends over weeks and months. A sustained downward trend signals overtraining, sleep deprivation, illness, or chronic stress.
Clinical Evidence — Anxiety, Hypertension, Performance, Longevity
The clinical evidence for HRV biofeedback and resonance-frequency breathing covers several domains:
- Anxiety disorders — the Goessl 2017 meta-analysis (PMID 28478782) found significant reductions in self-reported anxiety across 24 HRVB studies. Effect sizes were comparable to first-line cognitive behavioral therapy interventions.
- Hypertension — the Lin 2012 study (PMID 22468936) demonstrated significant systolic and diastolic blood pressure reductions in pre-hypertensive adults after 10 weeks of HRVB. The mechanism is improved baroreflex gain.
- Sport performance — the Pagaduan 2019 meta-analysis (PMID 31309366) showed HRVB improved performance measures across 11 studies in athletic populations, particularly in disciplines requiring precise motor control (shooting, golf, gymnastics).
- Depression — multiple RCTs have shown HRVB improves depressive symptoms in mild-to-moderate depression, including a notable Karavidas 2007 trial on resistant depression.
- Post-MI mortality — HRV remains a standard prognostic measure in cardiac rehabilitation, with low HRV at hospital discharge an independent predictor of subsequent mortality and reinfarction.
- Asthma — Lehrer et al. demonstrated that HRVB reduced asthma medication requirements in moderate-severity adult asthma over 10-week training.
- Cognitive function — Thayer and Lane's 2009 Neuroscience & Biobehavioral Reviews paper (PMID 18771686) summarized the "neurovisceral integration" framework linking vagal tone to prefrontal cortical function. Higher HRV correlates with better executive function across multiple cognitive tests.
- Longevity — epidemiological studies including Framingham have documented HRV as an independent predictor of all-cause mortality. The mechanism likely combines cardiovascular protection, anti-inflammatory effects, and broader autonomic resilience.
What Affects Vagal Tone Beyond Breathing
While paced breathing is the most powerful single voluntary intervention for vagal tone, several other factors substantially affect baseline HRV:
- Aerobic exercise — the strongest non-breathing intervention. Endurance athletes characteristically have very high HRV due to high vagal tone at rest. The cardiovascular adaptation to consistent moderate-intensity aerobic exercise raises HRV over months.
- Sleep — HRV during deep slow-wave sleep is the highest of any time of day and is a marker of restorative sleep quality. Sleep deprivation acutely lowers HRV.
- Alcohol — even one or two drinks acutely lowers nighttime HRV by 20-30% for the night following. Heavy drinking has chronic depressive effects on vagal tone.
- Cold exposure — cold-water face immersion specifically activates the diving reflex, producing immediate bradycardia and vagal activation. Regular cold-shower or ice-bath practice raises baseline HRV.
- Meditation — multiple meditation styles (transcendental meditation, mindfulness, focused attention) raise HRV similarly to paced breathing alone.
- Singing, chanting, humming, gargling — engage the ventral vagal innervation of the larynx and produce measurable acute vagal activation.
- Heat exposure (sauna) — produces a post-session parasympathetic rebound similar to exercise. Regular sauna use is associated with cardiovascular benefits.
- Connection and social warmth — positive social interaction activates the ventral vagal "social engagement" system per polyvagal theory.
- Diet quality, omega-3 fatty acid intake, blood glucose stability — all influence HRV through reduced systemic inflammation and improved metabolic flexibility.
For more on related interventions, see Cold Therapy, Meditation, and Sauna.
Cautions and Interpretation Pitfalls
- HRV is not a diagnostic tool — it is a trend indicator. A single reading is largely meaningless. The 7-day or 4-week rolling average compared to individual baseline is what carries signal.
- HRV cannot be compared between individuals — absolute HRV varies enormously with age, sex, baseline cardiovascular fitness, body size, and genetics. A 35-year-old endurance athlete with RMSSD 80 ms and a 70-year-old sedentary office worker with RMSSD 25 ms are not directly comparable.
- Optical PPG accuracy is limited during the day — consumer wearable HRV measurements during waking hours often have substantial error from motion artifact. Nighttime measurements are more reliable.
- Atrial fibrillation invalidates standard HRV interpretation — the irregularly irregular rhythm produces high HRV values that do not reflect vagal tone.
- Beta-blockers and other heart-rate-affecting medications confound HRV — standard interpretation assumes intact autonomic-cardiac coupling.
- HRV biofeedback can be over-emphasized — for most people, simply practicing slow paced breathing daily produces 80% of the benefit of a structured HRVB protocol. Do not let the lack of a device prevent practice.
- Apple Watch and Oura nighttime HRV trends are useful for tracking; absolute numbers should be interpreted cautiously and not compared to ECG-derived clinical norms.
Key Research Papers
- Lehrer PM, Gevirtz R (2014). Heart rate variability biofeedback: how and why does it work? Frontiers in Psychology, 5:756. PMID: 25101026. — PubMed: 25101026
- Vaschillo EG, Vaschillo B, Lehrer PM (2006). Characteristics of resonance in heart rate variability stimulated by biofeedback. Applied Psychophysiology and Biofeedback, 31(2):129-42. PMID: 16838124. — PubMed: 16838124
- Porges SW (2007). The polyvagal perspective. Biological Psychology, 74(2):116-43. PMID: 17049418. — Search PubMed
- Thayer JF, Lane RD (2009). Claude Bernard and the heart-brain connection: further elaboration of a model of neurovisceral integration. Neuroscience & Biobehavioral Reviews, 33(2):81-8. PMID: 18771686. — PubMed: 18771686
- Shaffer F, Ginsberg JP (2017). An overview of heart rate variability metrics and norms. Frontiers in Public Health, 5:258. PMID: 29034226. — PubMed: 29034226
- Lehrer PM, Vaschillo E, Vaschillo B, Lu SE, Eckberg DL, Edelberg R, Shih WJ, Lin Y, Kuusela TA, Tahvanainen KU, Hamer RM (2003). Heart rate variability biofeedback increases baroreflex gain and peak expiratory flow. Psychosomatic Medicine, 65(5):796-805. PMID: 12883107. — Search PubMed
- Steffen PR, Austin T, DeBarros A, Brown T (2017). The Impact of Resonance Frequency Breathing on Measures of Heart Rate Variability, Blood Pressure, and Mood. Frontiers in Public Health, 5:222. PMID: 28890890. — PubMed: 28890890
- Goessl VC, Curtiss JE, Hofmann SG (2017). The effect of heart rate variability biofeedback training on stress and anxiety: a meta-analysis. Psychological Medicine, 47(15):2578-2586. PMID: 28478782. — PubMed: 28478782
- Pagaduan JC, Chen YS, Fell JW, Wu SSX (2019). Systematic Review and Meta-Analysis on the Effect of Heart Rate Variability Biofeedback on Sport Performance. Applied Psychophysiology and Biofeedback, 45(4):343-356. PMID: 31309366. — Search PubMed
- Lin G, Xiang Q, Fu X, Wang S, Wang S, Chen S, Shao L, Zhao Y, Wang T (2012). Heart rate variability biofeedback decreases blood pressure in prehypertensive subjects. Journal of Alternative and Complementary Medicine, 18(2):143-52. PMID: 22468936. — Search PubMed
- Tracey KJ (2002). The inflammatory reflex. Nature, 420(6917):853-9. PMID: 12490960. — Search PubMed
- Pavlov VA, Tracey KJ (2012). The vagus nerve and the inflammatory reflex — linking immunity and metabolism. Nature Reviews Endocrinology, 8(12):743-54. PMID: 23169440. — PubMed: 23169440
PubMed Topic Searches
- PubMed: HRV biofeedback resonance frequency
- PubMed: Polyvagal theory
- PubMed: Vagal tone and inflammation
- PubMed: Respiratory sinus arrhythmia
Connections
- Breathwork (Main Hub)
- Breathwork Benefits
- Wim Hof Method
- Box Breathing and Resilience
- Pranayama Traditions
- Meditation
- Cold Therapy
- Sauna
- Heart Rate Variability Testing
- Hypertension
- Heart Disease
- Anxiety
- Depression
- Type 2 Diabetes
- All Remedies