Zinc Toxicity: Copper Deficiency, Anosmia, and Metal Fume Fever
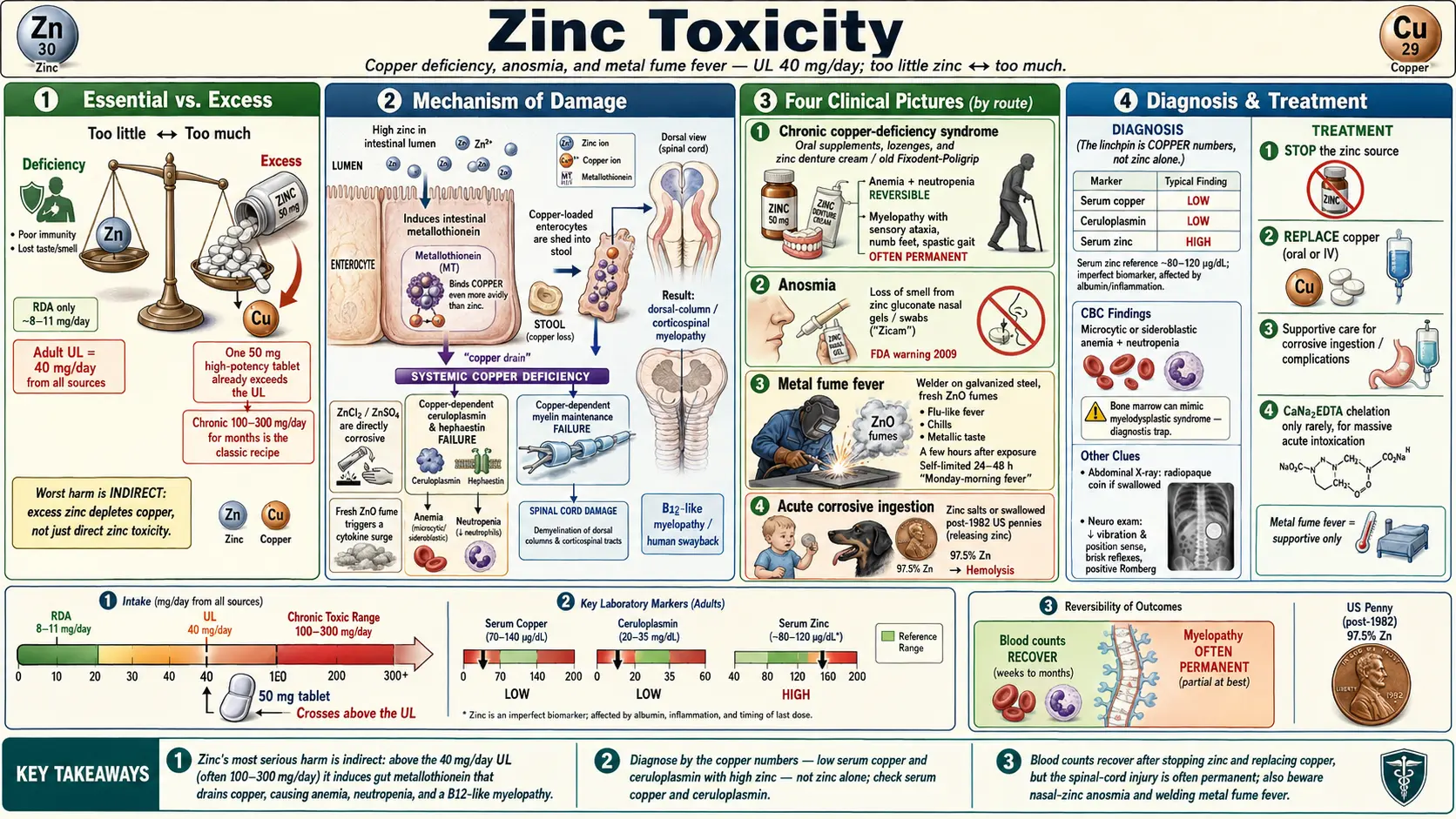
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Zinc is an essential trace mineral — the human body uses it in roughly a thousand enzymes and in the “zinc-finger” proteins that switch genes on and off. Our companion page, Zinc (essential trace mineral), covers why we need it for immunity, wound healing, taste, smell, and growth. This page is its mirror image: what happens when there is too much. Zinc has a relatively wide safety margin compared with metals like lead or mercury, but “wide” is not “infinite,” and the ways zinc harms the body are unusual, frequently missed, and sometimes permanent.
The single most important fact about zinc toxicity is that its most damaging form rarely looks like poisoning at all. Chronic excess zinc does its worst harm indirectly, by driving copper out of the body. The result is a syndrome of zinc-induced copper deficiency: anemia, a falling white-cell count, and a slowly progressive injury to the spinal cord that mimics the vitamin B12 deficiency disease known as subacute combined degeneration. People develop numb feet, an unsteady “sensory” gait, and weakness — and because the zinc source (often a supplement or a denture cream) seems harmless, the cause can go unrecognized for months or years. By then the spinal-cord damage may be irreversible.
Zinc causes several other distinct problems that this page explains in plain terms with the real numbers and mechanisms behind them:
- Chronic copper-deficiency syndrome — anemia, neutropenia, and an often-irreversible myelopathy (“human swayback”), classically from over-supplementation or zinc-laden denture adhesive cream.
- Anosmia (loss of smell) — linked to zinc gluconate nasal gels and swabs, which the U.S. Food and Drug Administration (FDA) warned against in 2009.
- Metal fume fever — a self-limited, flu-like illness from inhaling freshly formed zinc-oxide fume during welding or cutting galvanized steel.
- Acute corrosive injury — from swallowing zinc salts (zinc chloride, zinc sulfate) or ingesting zinc-rich objects such as post-1982 U.S. pennies.
The good news is that the chemistry that makes zinc dangerous also points to the cure: stop the zinc source and, where copper has been depleted, replace the copper. Blood counts usually recover. The nervous-system injury is the part that may not. That asymmetry — reversible blood, often-permanent nerve damage — is the through-line of this entire page and the strongest argument for catching zinc excess early.
2. Sources & Routes of Exposure
Excess zinc reaches people by three very different routes — swallowing it, inhaling it, or applying it to the nasal lining — and each route produces a different illness. Knowing the source is half the diagnosis, because the laboratory clues only make sense once you know what someone has been taking, breathing, or applying.
Oral overexposure (supplements, lozenges, denture cream)
For adults, the Tolerable Upper Intake Level (UL) for zinc is 40 mg/day from all sources combined, set by the U.S. National Academies and used by the National Institutes of Health Office of Dietary Supplements. The UL is the daily intake unlikely to cause harm in most people; the recommended dietary allowance is only about 8–11 mg/day, so a single “high-potency” zinc tablet (often 50 mg) already exceeds the safe ceiling. Chronic intakes well above the UL — commonly 100–300 mg/day taken for months “for immunity” — are the classic recipe for copper deficiency.
Three oral sources dominate the case literature:
- High-dose zinc supplements: capsules and “immune support” combinations taken daily for long periods.
- Zinc lozenges: intended for short-term use during a cold, but sometimes consumed by the bagful for weeks, easily delivering hundreds of milligrams per day.
- Zinc-containing denture adhesive cream: the landmark, almost counter-intuitive source. Older formulations of popular fixative creams (certain Fixodent and Poligrip products) contained zinc. People who over-applied them and swallowed the excess — often because poorly fitting dentures made them use more — absorbed substantial daily zinc, producing copper-deficiency myeloneuropathy. This was documented in case series and led to litigation; manufacturers subsequently reformulated to zinc-free versions.
Inhalation (zinc-oxide fume and zinc-chloride smoke)
The lungs face two separate zinc hazards that must not be confused:
- Zinc-oxide (ZnO) fume is produced when galvanized (zinc-coated) steel is welded, cut, brazed, or melted. The hot metal vaporizes and the vapor instantly oxidizes into ultrafine particles that are easy to breathe deep into the lungs. This causes metal fume fever — unpleasant but self-limited.
- Zinc-chloride (ZnCl2) smoke comes from military and industrial smoke grenades (“HC” smoke). This is a far more dangerous exposure that can cause severe chemical pneumonitis and acute respiratory distress syndrome (ARDS) — a true medical emergency, not a passing fever.
Object ingestion (pennies, especially in toddlers and dogs)
U.S. pennies minted after 1982 are about 97.5% zinc with only a thin copper plating. Stomach acid corrodes that exposed zinc core, releasing absorbable zinc salts. Swallowed pennies are a recognized cause of zinc toxicity in toddlers and are an especially common emergency in dogs, who readily eat coins. In both, the released zinc can trigger destruction of red blood cells (hemolysis). Other zinc objects — nuts, bolts, hardware, and zinc-cored game tokens — behave the same way.
3. Toxicokinetics
“Toxicokinetics” simply means what the body does with a substance after exposure: how much gets in, where it goes, and how it leaves. With zinc, the entry-and-exit story is the whole plot, because the body controls zinc mainly at the gut wall — and that same control point is exactly where excess zinc sabotages copper.
Absorption and the gut “gatekeeper”
Zinc is absorbed across the lining of the small intestine. Healthy people absorb a higher fraction of zinc when their intake is low and a smaller fraction when intake is high — a built-in dimmer switch. The key molecule is metallothionein, a small, sulfur-rich protein inside intestinal cells (enterocytes). A high zinc intake induces the cell to make more metallothionein. This protein grabs metal ions, and here is the crucial twist: metallothionein binds copper even more avidly than it binds zinc.
Distribution and storage
Once absorbed, zinc travels in blood largely bound to albumin and to a smaller protein, with a fraction on alpha-2-macroglobulin. It distributes into virtually every tissue — muscle and bone hold the largest pools — and serves as a structural or catalytic cofactor in enzymes and DNA-binding proteins. Because so much zinc is locked inside cells doing essential work, the amount circulating in serum at any moment is small and easily perturbed, which is why (as the Diagnosis section explains) serum zinc is an imperfect snapshot of true body status.
Elimination — and how copper gets dragged out
Most zinc leaves the body in feces, partly as unabsorbed dietary zinc and partly via secretions back into the gut. This is where chronic toxicity does its damage. When excess zinc forces intestinal cells to overproduce metallothionein, that protein sequesters copper from food right inside the enterocyte. Enterocytes have a short life span and are continuously shed into the gut lumen. The copper-loaded, metallothionein-rich cells slough off and are lost in the stool — carrying their captured copper with them. Over weeks to months, this steady mucosal “copper drain” depletes the body of copper even when the diet contains plenty. The dose and duration matter: brief high intakes do little, but sustained intakes above the 40 mg/day UL — especially the 100–300 mg/day range — reliably tip the balance toward copper deficiency.
For inhaled zinc oxide, the kinetics are entirely different: the illness is driven by the ultrafine particles deposited in the lung within hours of exposure, not by accumulated body burden, which is why metal fume fever appears the same day and clears within a day or two.
4. Mechanism of Toxicity
Zinc injures the body through three distinct mechanisms, matched to its three routes of exposure. Understanding them explains why the same element can cause a slow neurological decline in one person, a one-day fever in another, and a chemical burn in a third.
Mechanism 1: Copper–zinc antagonism (the chronic, dangerous one)
This is the mechanism behind nearly all serious, long-term zinc harm. As described above, high zinc induces intestinal metallothionein, which preferentially binds copper and is shed in the stool, producing copper deficiency. Copper is itself essential, so depleting it disables copper-dependent systems:
- Blood formation: Copper is required by enzymes that load iron onto transferrin and incorporate it into hemoglobin (such as the ferroxidase ceruloplasmin and hephaestin). Without copper, the marrow cannot use iron properly, producing a microcytic or sideroblastic anemia, and white-cell production falters, causing neutropenia (low neutrophils) and broader leukopenia.
- The nervous system: Copper-dependent enzymes maintain the myelin sheaths and metabolic machinery of the spinal cord. Copper deficiency damages the dorsal columns and corticospinal tracts — the same pathways injured in vitamin B12 deficiency — producing a myelopathy with sensory ataxia, a stiff “spastic” gait, and tingling or numbness (paresthesias). The clinical resemblance to B12 deficiency is so close that the syndrome is described as mimicking subacute combined degeneration; in animals an analogous copper-deficiency gait disorder is historically called “swayback,” hence the human nickname.
Mechanism 2: Direct corrosive and irritant action of zinc salts
Concentrated zinc salts — zinc chloride and zinc sulfate — are directly caustic to tissue. Swallowed in quantity (a soldering-flux exposure, a strong supplement solution, or acid releasing zinc from a swallowed coin), they chemically burn the lining of the mouth, esophagus, and stomach, causing intense pain, vomiting, and gastrointestinal bleeding. Inhaled or splashed, zinc chloride is corrosive to the airway and skin. This is a chemistry effect, not a copper effect, and it acts within minutes to hours.
Mechanism 3: Irritant/immunologic response to zinc-oxide fume
Freshly generated zinc-oxide particles are extremely fine and chemically reactive. Inhaled deep into the lung, they trigger an inflammatory and immune response — a surge of signaling molecules (cytokines) — that produces the fever, chills, and muscle aches of metal fume fever several hours after exposure. The reaction is self-limited because the body clears the particles and resolves the inflammation within a day or two, but it recurs with each new exposure. (Aged or weathered zinc oxide is far less potent; it is the freshly formed fume that matters.)
5. Symptoms & Health Effects
Because zinc harms the body in such different ways, its symptoms form four distinct clinical pictures. Recognizing which one you are looking at — and asking the right history question — is what makes the diagnosis.
Chronic copper-deficiency syndrome (the most serious)
This develops insidiously over months in someone taking high-dose zinc supplements, overusing zinc lozenges, or swallowing zinc-containing denture cream. The blood and the nervous system are affected, often together:
- Hematologic: fatigue, pallor, and breathlessness from anemia (typically microcytic or sideroblastic), plus a low white-cell count (neutropenia / leukopenia) that can raise infection risk. The bone-marrow appearance and low counts can be mistaken for a primary marrow disorder such as myelodysplastic syndrome — a diagnostic trap, because the “cure” here is copper, not chemotherapy.
- Neurologic (the often-irreversible part): numbness and tingling in the feet, a wide-based unsteady gait that worsens in the dark or with eyes closed (sensory ataxia), leg stiffness and weakness (spastic features), and difficulty with balance. This myelopathy resembles vitamin B12 deficiency clinically and is the most feared consequence because, unlike the blood changes, it may only partly reverse even after treatment — the spinal-cord injury can be permanent.
Anosmia from intranasal zinc
People who used zinc gluconate nasal gels or swabs (marketed to shorten colds; the best-known brand was Zicam) have reported anosmia — partial or complete loss of the sense of smell — sometimes beginning with a burning sensation on application and sometimes lasting long-term. The mechanism is direct zinc toxicity to the delicate olfactory neuroepithelium high in the nose. In 2009 the FDA warned consumers to stop using certain zinc-containing intranasal cold products because of this risk. (This is specific to putting zinc into the nose; ordinary oral zinc does not do this — in fact, dietary zinc deficiency can blunt smell and taste, the opposite problem covered on the essential-zinc page.)
Metal fume fever
Hours after welding, cutting, or brazing galvanized steel, the worker develops a flu-like illness: fever, chills, muscle aches, headache, a metallic taste in the mouth, dry cough, and a general “coming down with something” feeling. It is benign and self-limited, typically resolving in 24–48 hours with rest and fluids. A characteristic feature is tolerance that fades over a weekend: symptoms hit hardest on the first shift back, earning the folk names “Monday-morning fever,” “brass-founders’ ague,” and “galvo flu.” It recurs with each fresh exposure. The danger is misattributing it to a contagious flu and missing the workplace cause — or, more seriously, confusing it with the far worse zinc-chloride smoke-bomb inhalation, which instead causes progressive chemical pneumonitis and ARDS over hours to days and can be fatal.
Acute oral zinc-salt poisoning and penny ingestion
Swallowing corrosive zinc salts (zinc chloride or zinc sulfate) causes rapid nausea, repeated vomiting, severe epigastric (upper-abdominal) pain, and gastrointestinal bleeding from the chemical burn; very large ingestions can produce systemic effects including organ injury. Ingested zinc objects, especially post-1982 pennies, release zinc as stomach acid attacks them, and a notable consequence is hemolysis — destruction of red blood cells — producing anemia and, in dogs (the most common victims), dark urine, jaundice, vomiting, and collapse. In toddlers, a retained zinc coin similarly warrants prompt evaluation and removal.
6. Diagnosis & Laboratory Testing
Zinc toxicity is diagnosed by combining a careful exposure history with the right blood tests — and the single biggest mistake is measuring zinc alone. Because the hallmark injury is copper deficiency, the diagnosis lives in the copper numbers as much as in the zinc number.
The history is the most powerful test
Before any blood is drawn, the decisive clues come from asking:
- Are you taking a zinc supplement or a multi-ingredient “immune” product — and at what dose, for how long? (Remember the 40 mg/day UL; intakes of 100–300 mg/day are red flags.)
- Do you use denture adhesive cream, and how much — one application or several tubes a week?
- Are you using zinc lozenges heavily, or a zinc nasal product?
- Do you weld, cut, or braze galvanized steel (for fume fever), or could a child or pet have swallowed a coin?
In a person with unexplained anemia, low neutrophils, or a B12-like myelopathy whose B12 level is normal, these questions frequently crack the case.
Core blood panel: zinc, copper, ceruloplasmin, and a CBC
The essential workup pairs zinc with the copper markers and a blood count:
- Serum zinc — typically elevated above the reference range (often reported around ~70–120 micrograms per deciliter, µg/dL, in adults; high results support exposure but do not, by themselves, diagnose the syndrome).
- Serum copper — low. This is the linchpin. In zinc-induced copper deficiency, serum copper falls, often markedly.
- Ceruloplasmin — the main copper-carrying protein in blood; usually low, mirroring the copper deficiency and supporting the diagnosis.
- Complete blood count (CBC) — shows anemia (frequently microcytic, i.e., small red cells) and neutropenia / leukopenia. A bone-marrow examination, if done, may show characteristic features and ringed sideroblasts — and is what most often gets the diagnosis confused with a primary marrow disorder.
Note on units: laboratories may report copper and zinc in µg/dL or in micromoles per liter (µmol/L); the conversion factor differs for each metal, so always read the result against the issuing lab’s own reference range rather than memorizing a single cutoff.
Why serum zinc can mislead
Serum zinc is an imperfect biomarker. Most body zinc is inside cells, so the blood level reflects only a small, shifting fraction. It falls during inflammation or infection (zinc moves into tissues as part of the acute-phase response) and tracks with serum albumin, the protein that carries most circulating zinc — so a low albumin can drag the zinc reading down independently of true status. Hemolysis of the sample or zinc contamination from collection tubes can falsely raise it. The practical lesson: interpret zinc alongside copper, ceruloplasmin, the CBC, albumin, and a marker of inflammation — never in isolation.
Diagnosing the other zinc syndromes
Metal fume fever is a clinical diagnosis — the timing (hours after fume exposure), the self-limited course, and the occupational history are the diagnosis; routine bloods are nonspecific and zinc levels are not required to confirm it. Intranasal-zinc anosmia is likewise recognized from the history (a zinc nasal product, often with a burning sensation) plus formal smell testing. Penny ingestion is confirmed with an abdominal X-ray to locate the radiopaque coin, alongside a CBC and hemolysis markers (and in veterinary cases the same approach in dogs).
7. Treatment & Management
Treatment follows directly from the mechanism, and the first step is always the same: find and stop the zinc source. Everything else depends on which syndrome is present and how far it has progressed.
Stop the source — then replace copper
For chronic zinc-induced copper deficiency, the two pillars are removal and repletion:
- Discontinue the zinc — stop the supplement, switch off the zinc lozenges, change to a zinc-free denture cream, or remove whatever the source is. As long as the zinc keeps coming, copper cannot recover.
- Replace copper. Most patients are treated with oral copper (copper salts such as copper gluconate or copper sulfate), with intravenous copper reserved for severe deficiency or when the gut cannot absorb reliably. Copper status, blood counts, and zinc levels are monitored, and copper is continued until they normalize and stabilize.
The outcomes split sharply — and patients deserve an honest picture. The hematologic abnormalities usually recover: the anemia and the low white-cell counts typically correct over weeks once copper is restored. The neurologic myelopathy, however, is often only partly reversible. Treatment usually halts progression and may bring some improvement, but established spinal-cord damage frequently leaves lasting deficits. This is precisely why early recognition matters so much: the window to prevent permanent disability is before the nerve injury is entrenched.
Acute corrosive ingestion
Swallowed zinc chloride or zinc sulfate is a corrosive emergency managed with supportive care: airway protection, intravenous fluids, pain control, anti-nausea treatment, and careful evaluation of the burned esophagus and stomach (endoscopy may be needed). Inducing vomiting is avoided because it re-exposes the burned tissue. For a swallowed zinc coin, the object is generally removed (endoscopically) rather than left to keep dissolving and releasing zinc, and the patient is watched for hemolysis. In dogs, prompt removal of the coin plus supportive care (including transfusion for severe hemolysis) is standard veterinary practice.
When is chelation used?
Chelation — giving a drug that binds the metal so it can be excreted — is rarely needed for zinc, in sharp contrast to lead or mercury poisoning. The mainstay is removing the source and, for chronic cases, repleting copper. Chelation with calcium disodium EDTA (CaNa2EDTA) is reserved for massive acute zinc intoxication with high blood levels and systemic toxicity, used under specialist or poison-center guidance.
Metal fume fever and intranasal-zinc injury
Metal fume fever needs only supportive care — rest, fluids, and fever-reducers — because it is self-limited and resolves in a day or two; the real intervention is preventing the next episode through workplace controls (below). Distinguishing it from zinc-chloride smoke inhalation is critical, because the latter requires aggressive respiratory care and monitoring for ARDS. For intranasal-zinc anosmia, the product is stopped immediately; smell may recover partially, but some cases are long-lasting, so management centers on stopping exposure and, when needed, formal evaluation by an ear-nose-throat specialist.
In every scenario, contacting a regional poison control center is reasonable for dosing, monitoring, and decontamination advice.
8. Prevention & Risk Reduction
Almost every case of serious zinc toxicity is preventable, because almost every source is something a person chooses to take, breathe, or apply. The practical safeguards differ by route.
Use supplements within the safe ceiling
- Respect the 40 mg/day adult UL for total zinc from supplements and fortified foods. Most people meet their needs (about 8–11 mg/day) from diet alone; routine high-dose zinc is unnecessary and risky.
- Use zinc lozenges only short-term for a cold — days, not weeks — and count the milligrams; many products deliver large doses if used frequently.
- If long-term higher-dose zinc is genuinely required, it is usually paired with monitoring of copper status under medical supervision, and sometimes with copper supplementation, specifically to head off deficiency.
- Check denture adhesive labels. Choose zinc-free formulations, apply the smallest effective amount, and have ill-fitting dentures adjusted so you are not tempted to over-apply cream (the behavior behind the original myeloneuropathy cases).
Avoid zinc nasal products
Do not use zinc gluconate nasal gels or swabs to treat colds. The FDA’s 2009 warning followed reports of lasting loss of smell, and the benefit was never worth that risk. Oral zinc lozenges (used briefly) do not carry this anosmia hazard.
Control welding and cutting fume
For anyone working with galvanized steel, metal fume fever is prevented the same way as other fume hazards:
- Local exhaust ventilation to capture fume at the source, plus good general ventilation in the work area.
- Respiratory protection appropriate to the task when ventilation alone is insufficient.
- Where feasible, removing the zinc coating from the weld zone beforehand, and positioning the body to keep the head out of the rising plume.
- Recognizing that benign metal fume fever and dangerous zinc-chloride smoke exposure are different problems — smoke-device incidents need immediate medical evaluation, not reassurance.
Keep zinc objects away from children and pets
Store coins, hardware, and zinc-cored items out of reach of toddlers, and be especially vigilant with dogs, who swallow pennies readily. Prompt veterinary or pediatric attention for a suspected swallowed coin — before extensive hemolysis develops — is the single best preventive step once ingestion has happened.
9. Related Topics
- Zinc (essential trace mineral) — the companion page on why the body needs zinc; this toxicity page is its deliberate counterpart and contrast.
- Copper — the mineral driven out of the body by excess zinc; copper biology explains every feature of the deficiency syndrome.
- Copper Toxicity — the opposite end of the copper–zinc balance, where copper is the metal in excess.
- Iron Overload — another trace-metal excess affecting blood and organs, useful for contrast.
- Selenosis — toxicity of another essential trace mineral with a narrow safe range.
- Heavy Metals — overview of metal toxicology, where chelation (rarely needed for zinc) is central.
- Iron — essential mineral whose handling depends on copper, linking copper deficiency to anemia.
- Selenium — essential trace mineral, companion to the selenosis toxicity page.
- Anemia — the blood disorder that copper deficiency from zinc excess can cause.
- All Toxic Minerals — the full library of mineral-toxicity pages on this site.
- All Minerals — the complete minerals section, essential and toxic.
- Lab Tests — background on the serum zinc, copper, ceruloplasmin, and CBC tests used to diagnose this condition.
10. Key Research Papers
- Fosmire GJ. Zinc toxicity. American Journal of Clinical Nutrition, 1990;51(2):225–227. doi:10.1093/ajcn/51.2.225
- Willis MS, Monaghan SA, Miller ML, et al. Zinc-induced copper deficiency: a report of three cases initially recognized on bone marrow examination. American Journal of Clinical Pathology, 2005;123(1):125–131. doi:10.1309/V6GV-YW2Q-TYD5-C5PJ
- Kumar N, Gross JB Jr, Ahlskog JE. Copper deficiency myelopathy produces a clinical picture like subacute combined degeneration. Neurology, 2004;63(1):33–39. doi:10.1212/01.WNL.0000132644.52613.FA
- Nations SP, Boyer PJ, Love LA, et al. Denture cream: an unusual source of excess zinc, leading to hypocupremia and neurologic disease. Neurology, 2008;71(9):639–643. doi:10.1212/01.WNL.0000312375.79881.94
- Jaiser SR, Winston GP. Copper deficiency myelopathy. Journal of Neurology, 2010;257(6):869–881. doi:10.1007/s00415-010-5511-x
- Lazarchick J. Update on anemia and neutropenia in copper deficiency. Current Opinion in Hematology, 2012;19(1):58–60. doi:10.1097/MOH.0b013e32834da9d2
- Alexander TH, Davidson TM. Intranasal zinc and anosmia: the zinc-induced anosmia syndrome. The Laryngoscope, 2006;116(2):217–220. doi:10.1097/01.mlg.0000191549.17796.13
- Greenberg MI, Vearrier D. Metal fume fever and polymer fume fever. Clinical Toxicology, 2015;53(4):195–203. doi:10.3109/15563650.2015.1013548
- Hsu HH, Tzao C, Chang WC, et al. Zinc chloride (smoke bomb) inhalation lung injury: clinical presentations, high-resolution CT findings, and pulmonary function test results. Chest, 2005;127(6):2064–2071. doi:10.1378/chest.127.6.2064
- Bothwell DN, Mair EA, Cable BB. Chronic ingestion of a zinc-based penny. Pediatrics, 2003;111(3):689–691. doi:10.1542/peds.111.3.689
- Luttgen PJ, Whitney MS, Wolf AM, Scruggs DW. Heinz body hemolytic anemia associated with high plasma zinc concentration in a dog. Journal of the American Veterinary Medical Association, 1990;197(10):1347–1350. doi:10.2460/javma.1990.197.10.1347
- National Institutes of Health, Office of Dietary Supplements. Zinc — Health Professional Fact Sheet (Tolerable Upper Intake Level and copper-deficiency risk). ods.od.nih.gov/factsheets/Zinc-HealthProfessional
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Zinc. U.S. Department of Health and Human Services. atsdr.cdc.gov/toxprofiles/tp60.pdf
- U.S. Food and Drug Administration. Warning on Zicam Intranasal Zinc Cold Remedies and the Risk of Anosmia (consumer/public health advisory, June 2009). fda.gov — drug safety information
- U.S. Centers for Disease Control and Prevention / National Institute for Occupational Safety and Health (NIOSH). Welding fume and metal fume fever (zinc oxide) — occupational safety guidance. cdc.gov/niosh/topics/welding
Connections
- Zinc Toxicity (Excess Zinc) — the same excess written for the supplement user rather than the toxicologist, with per-symptom deep-dive pages on nausea, copper deficiency, and weakened immunity.
- Zinc (essential)
- Copper
- Copper Toxicity
- Iron Overload
- Selenosis
- Heavy Metals
- Iron
- Selenium
- Anemia
- All Toxic Minerals
- All Minerals
- Lab Tests