Thallium Poisoning: The "Poisoner's Poison" — Symptoms, Diagnosis, and Treatment
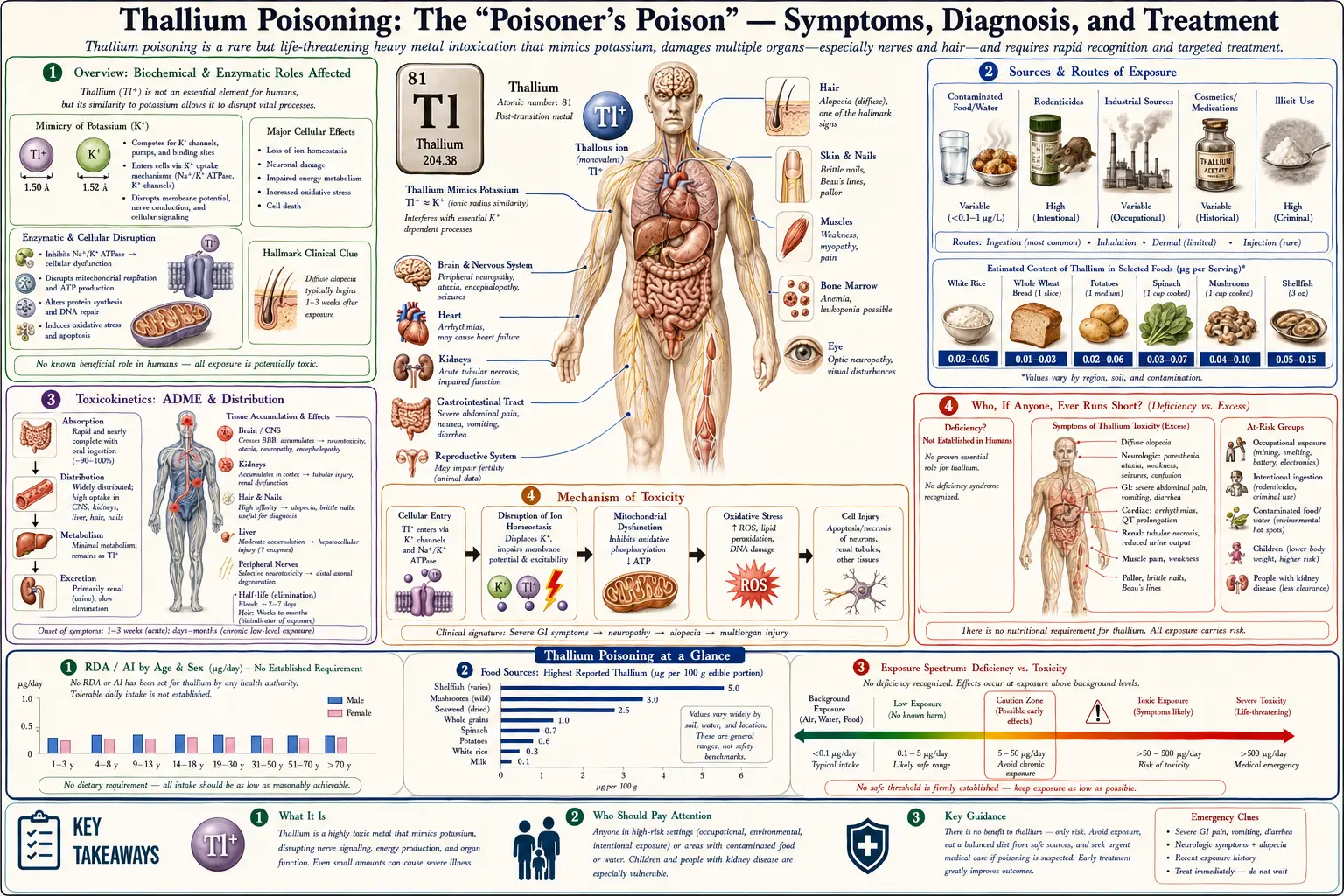
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Thallium (chemical symbol Tl) is a soft, silvery-white metal that, in its soluble salt forms, ranks among the most insidious poisons known to medicine. It earned the grim nickname "the poisoner's poison" for a simple, terrible reason: thallium salts are colorless, odorless, and very nearly tasteless when dissolved in food or drink, and the illness they cause unfolds slowly enough — and resembles so many ordinary conditions — that doctors and victims alike can easily miss the true cause for weeks. People have been quietly murdered with it, and others have used it to end their own lives, precisely because it hides so well.
If you have ever read Agatha Christie's 1961 mystery novel The Pale Horse, you have already met thallium. Christie, who trained as a pharmacy dispenser, described the poisoning so accurately — the strange tingling in the feet, the falling hair — that her fiction has more than once helped real clinicians and even alert readers recognize a genuine case that physicians had overlooked. In one famous 1977 instance a nurse suspected thallium in a sick infant after reading the novel; her hunch was correct and the child survived. Few poisons can claim to have been diagnosed by a paperback.
For most of the twentieth century thallium sulfate was sold cheaply as a rat and ant poison (rodenticide) and, in some countries, used in depilatory creams to remove unwanted hair — an early hint of one of its hallmark effects. Because the same properties that made it an effective pesticide also made it lethal and easy to misuse, the United States banned its sale to the general public in the 1960s and 1970s, and many other nations have since banned thallium-based rodenticides outright. Yet poisonings still occur today, from leftover legacy stockpiles, from contaminated illicit drugs and adulterated herbal products, from rare industrial accidents, and from the occasional deliberate act.
Why this page matters
This article is written for patients, families, and caregivers — not only for doctors. Thallium poisoning is treatable, and outcomes are dramatically better when it is caught early, but its early signs are so general (an upset stomach, aching legs) that the diagnosis is frequently delayed. Knowing that an unexplained, painful nerve illness followed a few weeks later by sudden hair loss is a recognizable pattern can, quite literally, save a life. We will walk through where exposure comes from, how the metal behaves inside the body, the step-by-step way symptoms appear, the single most important laboratory test (a 24-hour urine thallium measurement), and the specific antidote, Prussian blue, that turns this poison from a frequently fatal one into a frequently survivable one.
A note on scale: thallium is not something the average person will encounter. There is no thallium in normal food, water, or supplements at harmful levels, and you cannot "accidentally accumulate" it through everyday life the way fears about other metals sometimes suggest. Poisoning almost always means a discrete exposure — usually a single contaminated source — rather than slow lifestyle buildup, which means a real case nearly always has a findable cause once someone thinks to look for it.
2. Sources & Routes of Exposure
Thallium does not have a smell, a color, or a strong taste in solution, which is exactly why exposure so often goes unnoticed until people are already sick. Understanding where it comes from helps both with diagnosis (what to ask about) and with prevention.
Rodenticides and pesticides (the legacy source)
Thallium sulfate was the classic ingredient in rat, mouse, and ant poisons for much of the twentieth century. It was odorless, water-soluble, and cheap, and a single small dose could kill a rodent over a day or two. Those same traits made it a favored agent for deliberate human poisoning and a frequent cause of accidental poisoning in children who found brightly packaged bait. Because of this, the United States restricted thallium rodenticides in the 1960s and banned them for general use by 1972, and many other countries followed. Despite the bans, old containers persist in basements, sheds, and warehouses around the world, and thallium-based pesticides are still available in some regions, so a history of rodent baiting — especially with an old or imported product — is always worth asking about.
Deliberate poisoning
Because it is so hard to detect by taste or smell and produces a slow, mystifying illness, thallium has a long history as an instrument of homicide and suicide. Notorious criminal cases — sometimes called serial "thallium murders" — appear in the medical and true-crime literature of many countries. For clinicians and families, the practical lesson is that an otherwise unexplained thallium poisoning, particularly one affecting more than one member of a household at staggered times, should raise the possibility of intentional administration and may require involving public-health or law-enforcement authorities.
Contaminated illicit drugs and herbal products
One of the most important modern sources is contamination. Outbreaks have been traced to illicit drugs (such as adulterated heroin or cocaine) and to certain imported herbal remedies and traditional medicines that were tainted with thallium, sometimes alongside other heavy metals such as lead or arsenic. Because the people affected may not realize their products are contaminated, and may be reluctant to disclose drug use, these exposures are easy to miss. Anyone presenting with the classic thallium picture should be asked, non-judgmentally, about recreational drug use and about unregulated supplements or remedies.
Industrial and occupational exposure
Thallium has genuine industrial uses, and workers in those settings can be exposed by inhaling dust or fumes or through skin contact. Applications include electronics and semiconductors, specialty optics and infrared lenses, low-temperature thermometers, certain alloys, and the manufacture of pigments and fireworks. Thallium is also released as a byproduct when ores containing lead, zinc, or copper are smelted, and from coal combustion and cement production, which is why it can show up as an environmental contaminant near such industries. A radioactive isotope, thallium-201, is used in some cardiac stress-imaging scans, but the tiny tracer doses given for medical imaging are not a source of poisoning.
Historical medical and cosmetic use
Thallium's most famous biological effect — making hair fall out — was once put to deliberate use. Early- to mid-twentieth-century depilatory creams and "ringworm" treatments used thallium acetate to remove scalp hair, and it was also tried for the night sweats of tuberculosis. These uses caused many poisonings and have been abandoned; they remain a vivid reminder of how directly thallium attacks the hair follicle.
How thallium gets into the body
Thallium can enter the body by all three major routes. It is swallowed (the usual route in poisonings, via contaminated food, drink, or pills), inhaled as dust or fumes (the main occupational route), and absorbed through intact skin, which is unusual for a metal and adds to its danger. Once inside, by any route, soluble thallium is taken up very efficiently — a point we turn to next.
3. Toxicokinetics
"Toxicokinetics" simply means what the body does with a poison over time — how it is absorbed, where it goes, how long it lingers, and how it leaves. Thallium's behavior in these four steps explains both why it is so dangerous and why its specific antidote works the way it does.
Absorption — fast and nearly complete
Soluble thallium salts are almost completely absorbed after they are swallowed, and they are also taken up readily through the lungs and even through unbroken skin. There is very little "natural barrier" protecting you from it. This near-total absorption means that even a modest contaminated dose delivers most of its thallium into the bloodstream, which is part of why small amounts can be so harmful.
Distribution — it goes nearly everywhere
Once in the blood, thallium does not stay there for long; it moves rapidly out of the bloodstream and into tissues throughout the body. Because the thallium ion behaves chemically much like potassium (the explanation is in the next section), it follows potassium into virtually every cell, reaching the nervous system, heart, kidneys, liver, muscle, skin, and hair follicles. It even crosses the placenta, so poisoning during pregnancy can affect the fetus. This wide distribution is why thallium produces such a broad, whole-body illness rather than damage confined to one organ.
Elimination and the enterohepatic loop
Thallium leaves the body slowly. Estimates of its biological half-life — the time for the body to clear half of a given amount — generally fall on the order of one to several weeks, and it can be measured in urine and stool for a long time after exposure. The body tries to get rid of thallium through the kidneys (into urine) and through the bile and gut (into stool). Here lies a crucial problem: thallium excreted into the gut in bile is partly reabsorbed from the intestine back into the blood — a recycling process called enterohepatic recirculation. In effect, the body keeps re-swallowing its own poison, which prolongs the exposure and worsens the damage.
This recycling is not just a piece of biochemical trivia — it is the key that unlocks treatment. The antidote Prussian blue works precisely by sitting in the gut and trapping the thallium that bile keeps depositing there, so that it is carried out in the stool instead of being reabsorbed. Understanding the enterohepatic loop is therefore the bridge between how thallium harms and how we stop it.
4. Mechanism of Toxicity
Thallium is so destructive because of a chemical coincidence: the thallium ion, written Tl+, is almost exactly the same size and charge as the potassium ion (K+). Potassium is one of the most important ions in all of biology — it drives nerve signals, muscle contraction, and the basic energy machinery of every cell. Because thallium is a near-perfect potassium impostor, the body's potassium-handling systems wave it through, and thallium then jams those systems from the inside. Picture a counterfeit key that fits every lock in a building: it opens doors it should not and gets stuck in mechanisms it was never meant to touch.
Hijacking the sodium-potassium pump
Every cell relies on an enzyme called Na/K-ATPase — the "sodium-potassium pump" — to keep the right balance of these ions across its membrane. Thallium is actually taken up by this pump more avidly than potassium itself, so it is actively concentrated inside cells. Once there, it disturbs the delicate potassium gradients that nerves and muscle need to fire and recover, which helps explain the prominent nerve and heart effects.
Poisoning the cell's power plants and protein factories
Many of the cell's most potassium-dependent machines also depend on thallium being kept out. When thallium substitutes for potassium inside mitochondria — the structures that generate cellular energy — it impairs energy production and triggers a damaging cascade of oxidative stress (a flood of harmful, reactive molecules) and opening of the so-called mitochondrial permeability transition pore, which can push a cell toward death. Laboratory studies on isolated liver mitochondria have demonstrated exactly this pattern of energy failure and oxidative injury from thallium. Thallium also disrupts ribosomes, the machinery that builds proteins, again because protein synthesis normally needs potassium; this slows the cell's ability to repair and maintain itself.
Binding sulfhydryl groups and starving key vitamins
Beyond imitating potassium, thallium has a strong chemical appetite for sulfhydryl (thiol) groups — sulfur-containing chemical handles found on many proteins and enzymes. By latching onto these, thallium inactivates a wide range of enzymes that the body needs to function. It particularly interferes with enzymes that depend on riboflavin (vitamin B2) and on the cell's master antioxidant glutathione, effectively creating a functional vitamin and antioxidant shortage inside the cell. Experimental work exploring thallium-induced kidney injury has examined this riboflavin and glutathione connection. The combined result — broken pumps, failing power plants, stalled protein production, disabled enzymes, and depleted antioxidant defenses — falls hardest on tissues with the highest energy needs and the most active cells: the nerves, the heart, the gut lining, and the rapidly dividing cells of the hair follicle. That tissue-by-tissue vulnerability is exactly the pattern we see in the symptoms.
5. Symptoms & Health Effects
Thallium poisoning is famous for unfolding in a recognizable sequence over days to weeks rather than all at once. The textbook progression is: an early stomach upset, then a striking and painful nerve illness, and finally the giveaway sign of hair loss. The trouble is that each early stage looks like something common, so the pattern is often only obvious in hindsight. Severity depends heavily on the dose — large exposures can cause rapid, life-threatening illness within a day or two, while smaller chronic exposures cause a slower, more confusing picture.
Stage 1 — Early gastrointestinal upset (hours to ~2 days)
The first symptoms are usually digestive and easily mistaken for food poisoning or a stomach virus: nausea, vomiting, abdominal pain, and diarrhea — though some people instead develop constipation. These appear within hours to a couple of days of a significant exposure and then often subside, creating a deceptive lull during which the patient and even doctors may assume the worst is over. It is not.
Stage 2 — Painful ascending peripheral neuropathy (days to ~2 weeks)
Within several days, the hallmark nerve damage (peripheral neuropathy) sets in, and it is one of the most distinctive features of thallium poisoning. It typically ascends — starting in the feet and toes and moving upward — and is intensely painful, with patients describing burning feet and an exquisite, almost unbearable sensitivity in which the lightest touch, such as bedsheets resting on the legs, causes severe pain. There may be numbness, tingling, weakness, and difficulty walking. This combination of severe, painful, ascending sensory neuropathy is unusual enough that, in the right setting, it should prompt a clinician to specifically think of thallium. Cranial nerves can be affected too, sometimes causing facial weakness, double vision, or trouble swallowing.
Stage 3 — Alopecia and Mees' lines (about 1 to 3 weeks)
The single most famous sign of thallium poisoning is alopecia, or hair loss, which characteristically appears roughly one to three weeks after exposure — often just as the patient and doctors are most puzzled. Scalp hair comes out in handfuls, and the eyebrows, eyelashes, and body hair may thin as well, although a portion of the inner eyebrow is sometimes relatively spared. Because thallium poisons the rapidly dividing cells of the hair follicle, this is one of the body's earliest visible casualties. Sudden, unexplained hair loss following a recent painful nerve illness is, classically, the clue that finally points to thallium. Around the same time, horizontal white bands called Mees' lines may appear across the fingernails and toenails — a sign shared with arsenic poisoning that reflects a temporary halt in nail growth. If the patient recovers, hair usually regrows over the following months.
Other organ systems
- Autonomic nervous system: Thallium disturbs the "automatic" nerves that control involuntary functions, causing rapid heart rate, high blood pressure, dry mouth, constipation, and disturbances of sweating and salivation.
- Central nervous system and behavior: Confusion, agitation, anxiety, insomnia, tremor, seizures, hallucinations, and, in severe poisoning, declining consciousness or coma. Some survivors are left with lasting memory, cognitive, or movement problems.
- Heart: Abnormal heart rhythms and changes on the electrocardiogram (ECG) can occur, and severe poisoning can stress the heart muscle dangerously.
- Eyes: Inflammation and damage of the optic nerve can blur or dim vision and, in serious cases, threaten sight.
- Skin: Beyond hair loss, the skin may become dry and scaly, and acne-like eruptions can appear.
- Kidneys and liver: As thallium concentrates in and injures these organs, blood and urine tests may show signs of kidney or liver strain.
Acute versus chronic exposure
A single large dose (acute poisoning) tends to produce the dramatic, fast-moving sequence above, sometimes progressing to coma and death within days if untreated. Chronic, low-level exposure — for example from an ongoing contaminated source or occupational dust — can be much harder to recognize, producing fatigue, vague aches, gradual nerve symptoms, mood changes, and slowly thinning hair without an obvious starting point. In either case, the more thallium absorbed and the longer treatment is delayed, the worse the outcome, which is why early recognition is so important.
6. Diagnosis & Laboratory Testing
The hardest part of diagnosing thallium poisoning is thinking of it in the first place. Because the early illness mimics food poisoning, then a mysterious painful neuropathy, the correct diagnosis is frequently delayed by days or weeks — and standard "tox screens" and routine blood panels do not include thallium. It must be specifically requested. The good news is that once it is suspected, thallium is straightforward to confirm with the right test.
The key test: 24-hour urine thallium
The single most useful test is a measurement of thallium in the urine, ideally collected over a full 24 hours. The kidneys excrete thallium for a long time after exposure, so urine is the most reliable place to find it. To give a sense of scale: people with no meaningful exposure typically have urinary thallium below roughly 1 to 2 micrograms per liter (µg/L) — and many laboratories regard normal background levels as well under 1 µg/L — whereas a poisoned patient may show levels tens, hundreds, or even thousands of times higher, often reported in the range of hundreds to thousands of µg/L or as a 24-hour total far above the normal output of about 0.4 to 0.8 micrograms per day. Exact reference values vary by laboratory and by the method used, so results should always be interpreted against the specific lab's reported normal range and in light of the clinical picture. The crucial point for patients and families is simple: if thallium poisoning is suspected, ask whether a urine thallium level has been sent.
Blood and other samples
Blood thallium can also be measured and may confirm a recent, heavy exposure, but because thallium leaves the bloodstream quickly and moves into tissues, blood levels can fall even while the person remains seriously poisoned; a low or "normal" blood level does not rule out poisoning, especially later in the illness. Urine is generally more dependable. Hair and nails can be analyzed too: because thallium is deposited in growing hair, segmental analysis along a hair shaft can sometimes reconstruct the timing of an exposure (for instance, distinguishing a single event from repeated poisoning), which is occasionally important in forensic or criminal investigations. Stool thallium may also be elevated.
Supporting clues and a high index of suspicion
Several findings can raise suspicion before the urine result returns. The clinical pattern itself — early gastrointestinal upset, then painful ascending neuropathy, then hair loss — is the most powerful clue, and any one of these arriving in sequence should prompt the question, "Could this be thallium?" Some thallium compounds are faintly visible (radiopaque) on an abdominal X-ray if recently swallowed, which can occasionally help. Doctors will also examine the nails for Mees' lines and may use nerve conduction studies to characterize the neuropathy. None of these substitute for the laboratory measurement, but together they justify ordering it. Reviews of real cases repeatedly emphasize the same lesson: the diagnosis is missed not because the test is unavailable, but because no one orders it — so the decisive step is maintaining a high index of suspicion and specifically asking the laboratory to measure thallium.
7. Treatment & Management
Thallium poisoning is a medical emergency, and treatment should always be directed by a hospital toxicology team or a regional poison control center. The encouraging news is that, unlike many metal poisonings, thallium has a genuinely effective and well-targeted antidote. Treatment rests on three ideas: stop more thallium from being absorbed, pull the thallium already in the body out faster, and support the patient through the illness while the metal is cleared.
The specific antidote: Prussian blue
The cornerstone of treatment is Prussian blue — chemically, insoluble ferric hexacyanoferrate — taken by mouth. It is the same deep-blue pigment historically used in paints and dyes, prepared in a specially pure, medical-grade, insoluble form, and it is approved by the U.S. Food and Drug Administration (FDA) for internal contamination with thallium (and with radioactive cesium). It works by exploiting thallium's own weaknesses. As bile keeps secreting thallium into the gut (the enterohepatic recirculation described earlier), Prussian blue sits in the intestine and acts like a molecular sponge: its crystal structure normally holds potassium ions, and it readily exchanges that potassium for thallium, trapping the thallium tightly inside the pigment. The bound thallium is then carried out of the body in the stool instead of being reabsorbed. In effect, Prussian blue interrupts the recycling loop and turns the gut into a one-way exit. Because it is essentially not absorbed itself, it is generally well tolerated; the main visible side effects are constipation and harmless blue-tinted stools. It is usually given for as long as thallium continues to be excreted, guided by repeat urine and stool measurements.
Limiting further absorption
If a large amount of thallium has very recently been swallowed, doctors may give activated charcoal, which binds thallium in the gut and is sometimes used in repeated doses to help capture thallium re-entering the intestine, complementing Prussian blue. Decontamination decisions depend on timing and the patient's condition and are made case by case.
Enhancing elimination
Because the kidneys excrete thallium, keeping urine flowing well with intravenous fluids (forced diuresis) can help, with careful attention to the body's potassium balance. In severe poisoning — very high levels, kidney failure, or critical illness — doctors may add hemodialysis (or related blood-cleansing techniques such as hemoperfusion, and in some reports albumin-based liver-support systems like MARS, or plasma exchange) to physically remove thallium from the blood faster, particularly early when more of it is still circulating. These intensive measures are reserved for the sickest patients and are used alongside, not instead of, Prussian blue.
What does NOT help — an important caution
It is essential to know that the standard metal chelating drugs do not work well for thallium and can make things worse. In particular, British Anti-Lewisite (BAL, dimercaprol) — a chelator used for some other heavy metals — is not effective against thallium and may actually redistribute thallium into the brain, worsening the neurological injury. This is a critical point: a treatment that helps with lead or arsenic can be harmful here. Some related agents (such as DMSA) have been studied with mixed and generally unimpressive results and are not a substitute for Prussian blue. This is precisely why thallium poisoning should be managed by, or in close consultation with, medical toxicology — the right antidote is specific, and the wrong "metal antidote" can do harm.
Supportive care and recovery
Around the antidote, patients need attentive supportive care: pain control for the often severe neuropathy, monitoring and protection of the heart, fluid and electrolyte management (with special attention to potassium), seizure control if needed, nutritional support, and intensive care for those who become critically ill. With prompt treatment many patients survive, though recovery from the nerve damage can be slow and incomplete, and some are left with lasting neurological or cognitive effects. Hair almost always regrows. The consistent theme across the medical literature is that earlier diagnosis and earlier Prussian blue lead to better outcomes — which loops back to why recognizing the symptom pattern matters so much.
8. Prevention & Risk Reduction
Because thallium poisoning almost always comes from a specific, identifiable source rather than from everyday life, prevention is largely about avoiding those sources and acting quickly when an exposure is suspected. For the general public the practical risk is low, but a few precautions matter — especially for households with old pest-control products, workers in certain industries, and anyone using unregulated drugs or remedies.
At home
- Get rid of old rodenticides. If you have inherited an old house, shed, garage, or warehouse, do not use unlabeled or old rat and ant poisons, and dispose of any thallium-containing pesticides through a hazardous-waste program rather than the trash. Keep all pesticides locked away from children.
- Be wary of unregulated herbal products and traditional medicines, particularly imported powders, pills, or tonics that have been linked to heavy-metal contamination. Choose products from sources that test for heavy metals, and treat dramatic "detox" or cure-all claims with skepticism.
- Recognize the pattern. The most valuable household "prevention" is awareness: an unexplained illness that moves from stomach upset to painful, burning feet to sudden hair loss should prompt you to ask a doctor specifically about thallium and request a urine thallium test. Catching it early changes the outcome.
For people who use recreational drugs
Illicit drugs have been a real source of thallium poisoning through contamination. If you or someone you care for develops the symptom pattern described here, share the full history honestly with medical staff — including any drug use — without fear of judgment. That information can be the difference between a fast diagnosis and a dangerous delay.
In the workplace
- Follow occupational safety rules in industries that handle thallium — electronics and semiconductor manufacturing, specialty optics and glass, certain alloys and pigments, and metal smelting — including ventilation, dust control, protective clothing and gloves (remember thallium can cross skin), and good hygiene such as not eating or smoking in work areas and washing thoroughly before doing so.
- Use exposure monitoring where appropriate; periodic urine testing can detect a problem before it becomes dangerous. Agencies such as the U.S. Agency for Toxic Substances and Disease Registry (ATSDR) and occupational-health authorities publish guidance and exposure limits for thallium in workplace air.
Environmental awareness
At the population level, thallium can enter the environment from coal burning, cement production, and the smelting of metal ores, occasionally contaminating soil, water, or locally grown food nearby. For the vast majority of people this contributes only trace, harmless background exposure; communities near heavy industry or mining are the ones for whom environmental thallium is most relevant, and they are best served by local environmental and public-health monitoring. For everyone else, the reassuring bottom line is that thallium poisoning is uncommon, source-driven, and — when recognized — both diagnosable and treatable.
9. Related Topics
- Toxic Minerals & Heavy Metals overview — how thallium fits among the major poisonous metals.
- Heavy Metals — shared themes of absorption, testing, and treatment across metal poisonings.
- Arsenic — like thallium, causes painful neuropathy and Mees' lines on the nails.
- Lead — a classic neurotoxic metal, but one where chelators (unlike with thallium) are central to treatment.
- Mercury — another heavy metal with prominent neurological effects.
- Cadmium — a toxic metal that, like thallium, injures the kidneys.
- Barium — another metal whose ion disturbs potassium handling in nerve and muscle.
- Potassium — the essential mineral that thallium impersonates; the heart of why thallium is so toxic.
- Selenium — an essential trace mineral that is also harmful in excess.
- Zinc — an essential mineral important to antioxidant and enzyme function.
- Parkinson's Disease — a movement disorder; severe thallium poisoning can leave lasting neurological effects.
- Anemia — a context for understanding broad effects of toxins on the body and blood.
- Lab Tests — background on the urine and blood testing used to confirm metal exposure.
10. Key Research Papers
- Hoffman RS. Thallium Toxicity and the Role of Prussian Blue in Therapy. Toxicological Reviews. 2003;22(1):29-40.
- Moore D, House I, Dixon A. Thallium poisoning: diagnosis may be elusive but alopecia is the clue. BMJ. 1993;306(6891):1527-1529.
- Soave PM, Chirico F, Pallocchi M, Magnavita N. Thallium Poisoning: Case Report and Scoping Review on Diagnostic Delay and Therapeutic Outcome. Applied Sciences. 2025;15(4):1732.
- Rusyniak DE, Kao LW, Nanagas KA, Kirk MA, Furbee RB, Brizendine EJ, Wilmot PE. Dimercaptosuccinic Acid and Prussian Blue in the Treatment of Acute Thallium Poisoning in Rats. Journal of Toxicology: Clinical Toxicology. 2003;41(2):137-142.
- Thompson DF, Callen ED. Soluble or Insoluble Prussian Blue for Radiocesium and Thallium Poisoning? Annals of Pharmacotherapy. 2004;38(9):1509-1514.
- Lin G, Yuan L, Bai L, Liu Y, Wang Y, Qiu Z. Successful treatment of a patient with severe thallium poisoning in a coma using Prussian blue and plasma exchange. Medicine. 2019;98(8):e14629.
- Wallbridge T, James S, Lee R, Khan A, Bradberry S, Elamin MEMO. Successful treatment of potentially lethal dose thallium sulfate poisoning with sequential use of Prussian blue and multiple-dose activated charcoal. Clinical Toxicology. 2023;61(3):200-201.
- Eskandari MR, Mashayekhi V, Aslani M, Hosseini M. Toxicity of thallium on isolated rat liver mitochondria: the role of oxidative stress and MPT pore opening. Environmental Toxicology. 2013;30(2):232-241.
- Appenroth D, Winnefeld K. Is thallium-induced nephrotoxicity in rats connected with riboflavin and/or GSH? Reconsideration of hypotheses on the mechanism of thallium toxicity. Journal of Applied Toxicology. 1999;19(1):61-66.
- Clinical features and therapy of acute thallium poisoning (classic case series). — Search PubMed
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Thallium. U.S. Department of Health and Human Services. Read the ATSDR profile
- Centers for Disease Control and Prevention (CDC) / ATSDR. Thallium — ToxFAQs and Public Health Statement. Read the CDC/ATSDR ToxFAQs
- National Library of Medicine, MedlinePlus. Thallium poisoning (overview). Read MedlinePlus
Connections
- All Toxic Minerals
- Heavy Metals
- Arsenic
- Lead
- Mercury
- Cadmium
- Barium
- Potassium
- Selenium
- Zinc
- Parkinson's Disease
- Anemia
- Lab Tests
- All Minerals