Barium Toxicity: Soluble Salts, Hypokalemia, and Muscle Paralysis
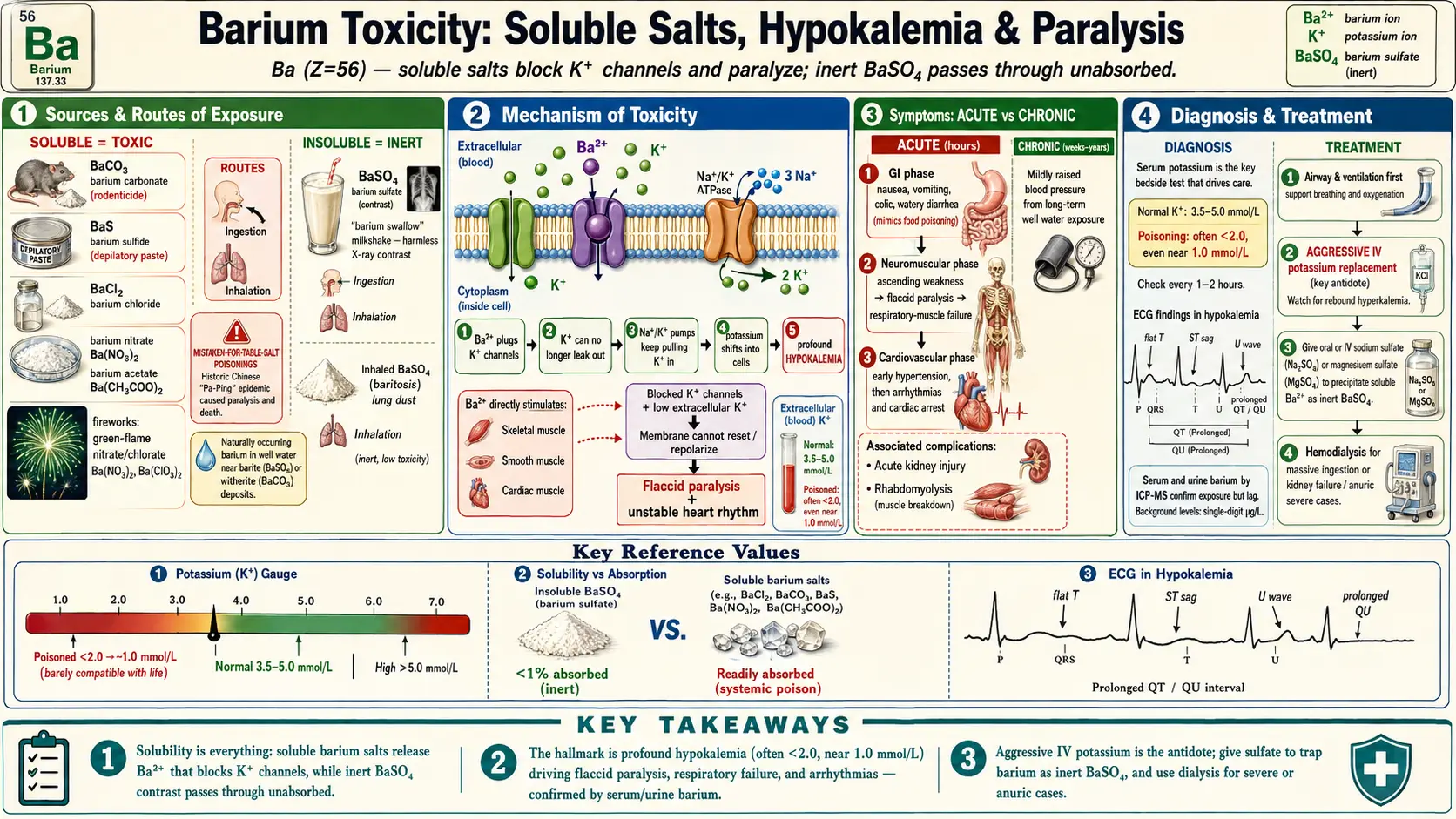
Table of Contents
- Overview
- Sources & Routes of Exposure
- Toxicokinetics
- Mechanism of Toxicity
- Symptoms & Health Effects
- Diagnosis & Laboratory Testing
- Treatment & Management
- Prevention & Risk Reduction
- Related Topics
- Key Research Papers
- Connections
- Featured Videos
1. Overview
Barium is a soft, silvery alkaline-earth metal (chemical symbol Ba, atomic number 56) that sits just below calcium and strontium on the periodic table. It is never found free in nature, and it is the chemistry of its compounds — not the metal itself — that decides whether a given form of barium is harmless or potentially lethal. This single idea, solubility determines toxicity, is the most important thing to understand about barium: it is why a hospital can ask you to drink a thick white barium milkshake for an X-ray while a chemist treats a few grams of a different barium salt as a deadly poison.
The dividing line is whether the compound dissolves in water and stomach acid. Barium sulfate (BaSO4), the contrast agent used in the familiar “barium swallow” and “barium enema,” is so insoluble that it passes through the gut essentially unabsorbed and is excreted in the stool; the body never sees free barium ions, so it is treated as biologically inert. By contrast, the soluble barium salts — chloride, carbonate, acetate, nitrate, hydroxide, and sulfide — release the barium ion (Ba2+) into the bloodstream, and that ion is a powerful systemic toxin.
What makes soluble barium dangerous in a way few poisons are is its effect on potassium. The barium ion blocks the channels that normally let potassium leave cells, producing one of the most dramatic drops in blood potassium seen in clinical medicine. That falling potassium, combined with barium’s direct effects on muscle, drives a progressive flaccid paralysis that can shut down the muscles of breathing and destabilize the heart — a patient can go from vomiting to near-total paralysis within hours. Crucially, this is one of the rare poisonings where the most life-threatening problem, profound hypokalemia, is also directly treatable: by giving potassium back faster than the barium can drive it out of the blood.
Barium poisoning is uncommon but not a historical curiosity. It still occurs through rodenticides, depilatory (hair-removal) products, occasional contamination of food and water, self-harm, and industrial accidents. Several of the worst recorded events were mass poisonings from soluble barium mistaken for ordinary table salt. Because the early symptoms mimic common food poisoning, recognizing barium toxicity often depends on a clinician thinking of it — and on a basic potassium test that returns an impossibly low number.
2. Sources & Routes of Exposure
Most people will never knowingly handle a soluble barium salt, yet barium compounds are surprisingly widespread in industry and in a handful of consumer products. Understanding where the dangerous forms turn up is the first step in avoiding them and in recognizing a poisoning when it happens.
Rodenticides and pesticides
Barium carbonate (BaCO3) has a long history as a rat and mouse poison and is still encountered in some parts of the world. Although barium carbonate is only modestly soluble in plain water, it dissolves readily in the acid of the stomach, releasing toxic barium ions after ingestion. Because the powder is white, odorless, and tasteless, it has repeatedly been swallowed by accident, used in self-harm, or added to food with intent to harm. Several of the published fatal and near-fatal cases involve barium carbonate taken this way.
Depilatory and cosmetic products
Barium sulfide (BaS) and related sulfides have been used in depilatory (hair-removal) pastes and powders because they break down the protein structure of hair. These products are a recognized cause of poisoning, particularly when applied to large areas, used in excess, or accidentally ingested — including by children who reach for a brightly packaged tube. Classic case reports describe hypokalemia and weakness after misuse of barium sulfide depilatories.
Contaminated food and water (mass poisonings)
The most striking episodes in the medical literature are outbreaks of mass poisoning caused by soluble barium contaminating food or salt. In China, a condition historically called “Pa-Ping” disease — a sudden epidemic paralysis — was eventually traced to table salt contaminated with barium chloride or carbonate. Similar events have followed when barium salts were mistaken for cooking salt, baking soda, or other kitchen staples. Naturally occurring barium can also reach drinking water where groundwater passes through barium-rich mineral deposits (such as barite and witherite), and well water near such formations is the most likely route of chronic, low-level exposure for the general public.
Industrial, occupational, and pyrotechnic sources
Barium compounds are used to make glass, ceramics, paints, lubricating-oil additives, drilling muds for oil and gas wells, and rubber. Fireworks and pyrotechnics rely on barium nitrate and barium chlorate to produce green flames. Workers in welding, smelting, mining, and barium-chemical manufacturing can inhale barium-containing dust and fumes. Inhalation of fine insoluble barium sulfate dust over years produces baritosis, a benign dust-deposition disease of the lungs (a pneumoconiosis) that shows up dramatically on chest X-rays but causes little or no impairment and tends to fade once exposure stops — a useful reminder that even the inhaled insoluble form behaves very differently from soluble barium taken by mouth.
Medical contrast (the important exception)
The barium sulfate used for gastrointestinal imaging is the one form most people will ever meet, and it is safe precisely because it is not absorbed. Its recognized hazards are mechanical rather than chemical: if the suspension is aspirated into the lungs, or if it leaks into the abdominal cavity through a perforation of the bowel, it can cause serious inflammation. These risks are about where the inert powder ends up, not about barium poisoning the way soluble salts do.
3. Toxicokinetics
Toxicokinetics describes what the body does to a poison — how it is absorbed, where it goes, and how it leaves. For barium, every step is governed once again by solubility, and the contrast between the soluble and insoluble forms could hardly be sharper.
Absorption
Soluble barium salts are absorbed from the gastrointestinal tract after ingestion and from the lungs after inhalation of soluble dust or fume. The fraction absorbed from the gut varies with the compound and stomach acidity, but enough crosses into the blood to cause systemic poisoning within minutes to a few hours. Insoluble barium sulfate, by design, is barely absorbed at all — well under one percent — which is exactly why it can be swallowed in large amounts for imaging without harm. This is the pivot on which barium’s whole toxicology turns: the same element is a contrast medium or a poison depending only on whether it can reach the bloodstream.
Distribution and storage in bone
Once in the blood, the barium ion behaves chemically much like calcium and strontium, its alkaline-earth neighbors. It distributes to soft tissues and is then taken up into bone, where it can be deposited in the mineral lattice in place of calcium. The skeleton becomes a long-term reservoir, and the great majority of barium in a chronically exposed person resides there — which is why barium and calcium are so often discussed together.
Elimination
Absorbed barium is cleared mainly by the kidneys into the urine, with an additional contribution from the gut into the feces. Because excretion is comparatively slow, anything that impairs kidney function — including the acute kidney injury that severe barium poisoning can itself cause — allows barium to linger and worsens the poisoning. This is one reason doctors may turn to dialysis in serious cases: it removes barium directly and compensates for failing kidneys. The unabsorbed barium sulfate from a contrast study simply passes through the bowel and is excreted unchanged, occasionally causing nothing worse than temporary constipation.
4. Mechanism of Toxicity
To understand why barium causes paralysis, it helps to picture what potassium normally does inside a living cell. Cells keep a high concentration of potassium inside and a low concentration outside, and they constantly let a little potassium “leak” back out through specialized openings called potassium channels. That steady outward trickle is what sets the cell’s resting electrical state and keeps nerves and muscles ready to fire on command. Potassium leaving the cell is, in effect, what lets a muscle relax and reset between contractions.
Blocking the potassium channels
The barium ion (Ba2+) is almost exactly the right size to plug many of these potassium channels. When barium blocks them, potassium can no longer trickle out of the cell at its normal rate. Because the cellular pumps keep actively pulling potassium in while the exit is blocked, potassium piles up inside cells and is stripped out of the bloodstream. The blood level of potassium can fall to extraordinary depths — values low enough that they look like a laboratory error. This is the central event of barium poisoning, and the term for it is hypokalemia (low blood potassium).
From hypokalemia to paralysis
The catch is that nerves and muscles depend on that potassium gradient to work. With the channels jammed and blood potassium collapsing, muscle cells can no longer reset properly after firing, so they progressively fail to respond — producing weakness that climbs from the limbs toward the trunk and, most dangerously, the muscles that drive breathing. The result is a flaccid (floppy) paralysis that can closely mimic neurological emergencies such as Guillain-Barré syndrome or hypokalemic periodic paralysis. The difference is that here the cause is a blocked channel plus a treatable electrolyte derangement, not nerve disease — which is why the right diagnosis changes everything.
Direct effects on muscle and heart
Barium does not act through potassium alone. It is also a direct stimulant of muscle tissue of every type — skeletal, smooth, and cardiac. In the gut this contributes to the early cramping, vomiting, and diarrhea; in blood vessels it can transiently raise blood pressure. In the heart, the combination of barium’s direct action and the profound hypokalemia is especially dangerous, because low potassium destabilizes the heart’s electrical rhythm and predisposes it to arrhythmias, including life-threatening ones. So the poisoned patient faces two convergent threats at once: paralysis of the breathing muscles and an unstable heart, both driven by the same disturbance of potassium and both able to cause death if not corrected quickly.
5. Symptoms & Health Effects
Barium poisoning is best understood in two very different pictures: the acute emergency that follows swallowing or inhaling a soluble salt, and the chronic effects of long-term low-level exposure. They share almost nothing in their presentation, and confusing the two is a common source of error.
Acute poisoning — a fast, stepwise collapse
Acute soluble-barium poisoning tends to unfold in a recognizable sequence, often over just a few hours:
- Gastrointestinal phase (first): nausea, vomiting, abdominal cramping or colic, and watery diarrhea begin soon after ingestion. Because these are the symptoms of ordinary food poisoning, the true cause is easy to miss at this stage. A burning sensation in the mouth and throat and excess salivation may accompany it.
- Neuromuscular phase: as blood potassium falls, muscle weakness appears — classically starting in the limbs and spreading. Tingling, twitching, and difficulty moving give way to a flaccid paralysis. The danger point is reached when the muscles of breathing weaken, producing shortness of breath and, ultimately, respiratory failure.
- Cardiovascular phase: blood pressure may rise early because of barium’s direct effect on vessels, then fall as the patient deteriorates. The heart rhythm becomes unstable. Arrhythmias, conduction disturbances, and cardiac arrest can occur, especially as potassium reaches dangerous lows.
- Other systemic effects: severe cases can be complicated by acute kidney injury, which further impairs the body’s ability to clear the barium, and by metabolic disturbances beyond potassium, including low phosphate. Profound muscle damage (rhabdomyolysis) has been reported.
The hallmark laboratory finding that ties this picture together is profound hypokalemia. A patient who looks like they have a stomach bug but turns out to have a startlingly low potassium — and then begins to weaken — should raise immediate suspicion of barium, particularly if there is any access to rodenticides, depilatories, or industrial chemicals.
Chronic exposure — a quieter, contested picture
Long-term, low-level intake of soluble barium, most plausibly from drinking water near barium-rich geology, has been studied chiefly for effects on the cardiovascular system. Some community studies linked higher barium in public water supplies to modestly higher blood pressure, although the overall human evidence is mixed and the doses involved in poisoning are far higher than anything from regulated water. Health agencies set drinking-water limits partly on this basis and have generally not found strong evidence that barium at typical environmental levels causes cancer.
Baritosis — the lung-only, benign exception
Years of inhaling fine insoluble barium sulfate dust (an occupational exposure in barite mining and processing) produces baritosis. On a chest X-ray the dense barium particles create striking white nodules throughout the lungs, which can look alarming. Yet baritosis is classed as a benign pneumoconiosis: it usually causes little or no breathing impairment, and the X-ray changes tend to regress after exposure ends. It is included here to underline the central theme — because this barium is insoluble and stays put rather than entering the blood, it does none of the systemic damage that a soluble salt would.
6. Diagnosis & Laboratory Testing
The single most useful principle in managing barium poisoning is this: you confirm the diagnosis with barium levels, but you manage the patient by potassium and the heart. Waiting for a barium result before acting can be fatal, because the dangerous physiology — collapsing potassium, weakening breathing muscles, an irritable heart — can be measured and treated immediately at the bedside.
Confirming exposure: serum and urine barium
Barium can be measured directly in blood (serum or whole blood) and in urine, typically by a technique called inductively coupled plasma mass spectrometry (ICP-MS) at a reference laboratory. Results are usually reported in micrograms per liter (µg/L) or micrograms per deciliter (µg/dL). Background barium in unexposed people is very low — on the order of single-digit micrograms per liter or less — so a markedly elevated level confirms exposure. Because these assays are sent out and take time, they serve mainly to confirm and document the poisoning rather than to guide minute-to-minute care. A 24-hour urine collection can help gauge total body burden and ongoing elimination.
The test that actually drives treatment: serum potassium
The decisive bedside test is serum potassium (K+). Normal blood potassium sits roughly between 3.5 and 5.0 millimoles per liter (mmol/L). In serious barium poisoning it can plunge well below 2.0 mmol/L, sometimes to values near 1.0 mmol/L that are barely compatible with life. Because barium keeps driving potassium into cells, the level can fall fast and can rebound just as fast once treatment begins. For that reason, potassium must be checked frequently — often every hour or two during the acute phase — so that replacement keeps pace and does not overshoot into dangerous high-potassium territory as the barium is cleared. Magnesium and phosphate should be monitored alongside, since they often fall too.
Continuous heart monitoring: the ECG
Every seriously poisoned patient needs continuous electrocardiographic (ECG) monitoring, because severe hypokalemia leaves a characteristic and dangerous signature on the heart tracing. Low potassium classically produces flattened or inverted T waves, a sagging ST segment, and the appearance of prominent U waves, often with a lengthening of the measured QT/QU interval. These changes warn of an electrically unstable heart that is prone to dangerous rhythms. Watching the ECG in real time lets the team see the heart recover as potassium is restored, and catch deterioration before it becomes arrest.
Putting it together and ruling out mimics
The diagnosis is usually made by combining the history (access to a barium source, a suggestive exposure), the clinical sequence (gut symptoms followed by ascending weakness), and the laboratory hallmark of profound, hard-to-explain hypokalemia, later confirmed by elevated barium levels. Doctors will also weigh the conditions barium can imitate — Guillain-Barré syndrome, hypokalemic periodic paralysis, organophosphate poisoning, and other causes of acute weakness — because the treatments differ sharply. A useful clue is that in barium poisoning the paralysis tracks the falling potassium and reverses as potassium is replaced.
7. Treatment & Management
Treatment of barium poisoning is logical once the mechanism is clear, and it is one of the more satisfying poisonings to manage because the central antidote — potassium — directly counteracts the toxin. Care has three aims: support breathing and circulation, give back the potassium barium is stealing, and remove or neutralize the barium still in the body. None of this is a substitute for emergency medical care; the steps below describe what a hospital does, not a home remedy.
Airway, breathing, and circulation first
Because barium can paralyze the muscles of respiration, the first priority is the airway and breathing. Patients who are weakening may need oxygen and, if respiratory muscles fail, mechanical ventilation until the poisoning is reversed. Heart rhythm and blood pressure are supported and continuously watched. These supportive measures buy the time during which the specific treatments take effect.
Aggressive potassium replacement — the key antidote
The cornerstone of treatment is aggressive replacement of potassium, usually given intravenously and titrated against frequent blood measurements. Restoring blood potassium does two things at once: it corrects the immediate threat to the heart and breathing, and it helps overcome barium’s block of the potassium channels, allowing muscle and nerve function to recover. Because potassium can rebound sharply once the barium begins to clear, replacement demands close monitoring to avoid swinging from dangerous lows to dangerous highs (hyperkalemia) — a transition that has been documented in barium cases and is itself hazardous.
Limiting absorption: sulfate to trap the barium
A clever, mechanism-based step is to give a sulfate — typically oral or intravenous sodium sulfate or magnesium sulfate. Sulfate reacts with the soluble barium still in the gut (and, to a degree, in the blood) to form insoluble barium sulfate, the same inert compound used for imaging. By converting the dangerous soluble form into the harmless insoluble form, sulfate stops further absorption and renders that barium safe to excrete. This turns barium’s defining chemistry against itself. Standard gut-decontamination measures may also be considered early after a large ingestion, guided by a poison center.
Enhanced elimination: hemodialysis in severe cases
For massive ingestions, for patients not responding to potassium replacement, or for those who develop acute kidney failure (which cripples the body’s normal route of barium excretion), hemodialysis can remove barium from the blood directly and simultaneously manage the failing kidneys and the electrolytes. Hemodialysis has been used successfully in serious barium poisonings and is an important option when the basic measures are not enough. Throughout, management is best coordinated with a poison control center and clinical toxicology specialists, who can tailor potassium targets, sulfate use, and the threshold for dialysis to the individual case.
8. Prevention & Risk Reduction
Because soluble barium poisoning is almost always the result of an identifiable product or exposure, it is highly preventable. The practical measures fall into a few common-sense categories.
Keep dangerous products out of reach and out of the kitchen
The recurring theme in mass poisonings is mistaken identity — a white barium salt swallowed because it was confused with table salt, baking soda, or flour. The single most effective safeguard is to never store industrial or pesticide chemicals in food containers or near food, and to keep barium-containing rodenticides and depilatory products clearly labeled, sealed, and well away from children. Depilatory pastes containing barium sulfide should be used strictly as directed, never on broken skin or over large areas, and kept where small children cannot reach a tube.
Protect against occupational exposure
For people who work with barium compounds — in chemical manufacturing, glass and ceramics, oil-field drilling muds, pyrotechnics, welding, or barite mining — risk is controlled through engineering controls (ventilation and dust suppression), appropriate respiratory protection, and good hygiene practices that keep dust off the hands, face, and food. Following workplace exposure limits and not eating or smoking in dusty areas substantially reduces both the acute risk from soluble dusts and the long-term, if benign, accumulation that causes baritosis.
Water, environmental sources, and informed choices
For the general public, the most realistic exposure is naturally occurring barium in private well water drawn from barium-rich geology. People on private wells can have their water tested, and regulated public water systems are required to keep barium below health-based limits set by agencies such as the U.S. EPA and the World Health Organization. Where levels are high, suitable filtration can reduce barium. None of these everyday sources approach poisoning levels, but testing offers reassurance and catches the rare problem well.
If exposure is suspected
If someone may have swallowed a soluble barium salt, this is a medical emergency: contact emergency services and a poison control center immediately rather than waiting for symptoms, because deterioration can be rapid. Early recognition — and an early potassium measurement — is what most often makes the difference between a frightening but survivable poisoning and a fatal one.
9. Related Topics
- Toxic Minerals — overview of poisonous mineral elements and how they harm the body.
- Heavy Metals — lead, mercury, arsenic, and cadmium exposure and testing.
- Lead Poisoning — another classic metal toxicity with overlapping diagnostic principles.
- Arsenic Exposure — a water-borne toxic element with global public-health impact.
- Potassium — the electrolyte at the center of barium’s toxicity and its treatment.
- Calcium — the alkaline-earth metal barium mimics, including in bone.
- Magnesium — co-monitored electrolyte; magnesium sulfate is used to precipitate barium.
- Sodium — relevant to the “mistaken-for-salt” mass poisonings and to sodium sulfate therapy.
- Lab Tests — serum and urine testing, electrolyte panels, and the ECG.
- Cardiomyopathy — context for the cardiac arrhythmias driven by severe hypokalemia.
- Kidney Disease — impaired kidneys slow barium clearance and worsen poisoning.
- All Minerals — the full library of essential and toxic mineral pages.
10. Key Research Papers
- Wu J, Liu Z. Clinical features and management strategies of acute soluble barium poisoning: a review of case reports. Postgraduate Medicine. 2025;137(5):338–343.
- McNeill IR, Isoardi KZ. Barium poisoning: an uncommon cause of severe hypokalemia. Toxicology Communications. 2019;3(1):88–90.
- Tao H, Man Y, Shi X, Zhu J, Pan H, Qin Q, Liu S. Inconceivable hypokalemia: a case report of acute severe barium chloride poisoning. Case Reports in Medicine. 2016;2016:2743134.
- Sigue G, Gamble L, Pelitere M, et al. From profound hypokalemia to life-threatening hyperkalemia: a case of barium carbonate poisoning. Archives of Internal Medicine. 2000;160(4):548–551.
- Ananda S, Shaohua Z, Liang L. Fatal barium chloride poisoning. American Journal of Forensic Medicine & Pathology. 2013;34(2):115–118.
- Leong W, Li C, Long Y, et al. Non-fatal acute barium carbonate poisoning following suicidal ingestion: a case report. SAGE Open Medical Case Reports. 2025;13:2050313X241311316.
- Wetherill SF, Guarino MJ, Cox RW. Acute renal failure associated with barium chloride poisoning. Annals of Internal Medicine. 1981;95(2):187–188.
- Gould DB, Sorrell MR, Lupariello AD. Barium sulfide poisoning: some factors contributing to survival. Archives of Internal Medicine. 1973;132(6):891–894.
- Brenniman GR, Kojola WH, Levy PS, Carnow BW, Namekata T. High barium levels in public drinking water and its association with elevated blood pressure. Archives of Environmental Health. 1981;36(1):28–32.
- Doig AT. Baritosis: a benign pneumoconiosis. Thorax. 1976;31(1):30–39.
- Compton A. Poisoning by barium carbonate. The Lancet. 1946;247(6391):287.
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Barium and Barium Compounds. U.S. Department of Health and Human Services. ATSDR ToxProfile (PDF).
- World Health Organization. Barium in Drinking-water: Background Document for Development of WHO Guidelines for Drinking-water Quality. WHO. WHO drinking-water document.
- Centers for Disease Control and Prevention (CDC), National Center for Environmental Health. Barium — Biomonitoring and toxic substances information. CDC. ATSDR/CDC public-health statement.
Connections
- All Toxic Minerals
- Heavy Metals
- Lead Poisoning
- Arsenic Exposure
- Potassium
- Calcium
- Magnesium
- Sodium
- Lab Tests
- Cardiomyopathy
- Kidney Disease
- All Minerals