Molybdenum Deficiency: What the Evidence Shows
Here is the honest bottom line, stated up front: dietary molybdenum deficiency is essentially unknown in healthy people. Molybdenum is a genuinely essential trace mineral — your body uses it to build a small helper molecule that four enzymes depend on — but it is so widespread in ordinary food, and the body conserves it so efficiently, that no one eating a normal mixed diet has ever been shown to run short. In the entire medical literature there is essentially one well-documented case of acquired deficiency, and it happened to a hospitalized man fed for months only through a vein with a formula that contained no molybdenum. The only other way the human body comes up short of usable molybdenum is not a dietary problem at all but a rare inherited disorder, molybdenum cofactor deficiency, in which a person cannot manufacture the helper molecule no matter how much molybdenum they eat. So if you have arrived here worried that your fatigue, headaches, or food sensitivities mean you are "low in molybdenum," the most useful thing this page can tell you is that this is almost certainly not the explanation — and it points you toward the far more common causes worth checking instead. This page explains what the evidence actually shows, why true deficiency is so vanishingly rare, the handful of edge cases where it does occur, and what (very little) you actually need to do about molybdenum.
Table of Contents
- What the Evidence Actually Says
- Why Deficiency Is Essentially Never Seen
- Who, If Anyone, Actually Becomes Deficient
- Molybdenum Cofactor Deficiency: The Genetic Disorder
- When It Is Almost Certainly Not Molybdenum
- What You Actually Need to Do
- Related Nutrients & Pages
- Key Research Papers
- Connections
- Featured Videos
What the Evidence Actually Says
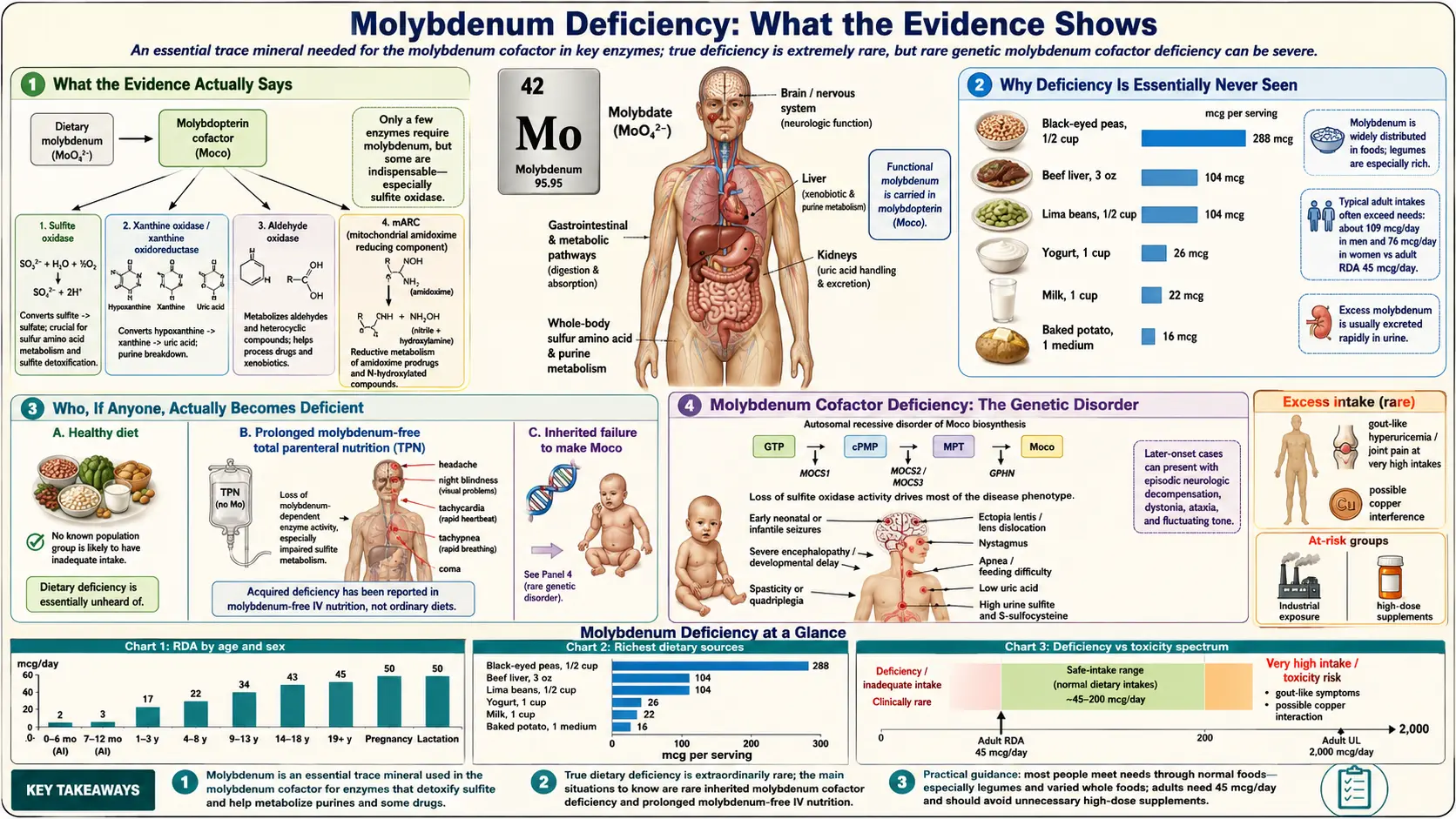
Let us be candid, because honesty serves you better than reassurance here: there is no recognized dietary molybdenum deficiency syndrome in humans. Major nutrition authorities say so plainly. The U.S. Institute of Medicine, when it set the Recommended Dietary Allowance for molybdenum at 45 micrograms a day for adults, noted that a naturally occurring deficiency had never been documented in otherwise healthy people. The NIH Office of Dietary Supplements states the same thing in its molybdenum fact sheet, and the European Food Safety Authority reached the identical conclusion when it reviewed the evidence for dietary reference values in 2013: there was not enough deficiency to define a requirement from, so the figures had to be estimated from balance and kinetic studies instead.
This is unusual. For most essential nutrients — iron, vitamin D, vitamin B12, magnesium, potassium — we know what running short looks like because shortage is common and the deficiency syndrome is well described. Molybdenum is the rare exception. It is unmistakably essential — remove the ability to use it and a person cannot survive infancy — yet ordinary dietary shortfall simply does not happen at a level that makes anyone sick. Both things are true at once, and the gap between them is the whole story of this page.
A few numbers make the point concrete:
- The requirement is tiny. The adult RDA is just 45 micrograms per day — micrograms, not milligrams. That is roughly one twenty-thousandth of a gram.
- Typical intake comfortably exceeds it. Surveys of Western diets put average molybdenum intake in the range of about 75 to 250 micrograms a day — several times the requirement — with legumes, grains, and nuts contributing most of it.
- The body adapts across an enormous range. Careful kinetic studies by Novotny and Turnlund, in which volunteers were fed intakes spanning from 22 up to nearly 1,500 micrograms a day, showed the body simply ramps urinary excretion up or down to keep stores stable. When intake is low, the kidneys conserve; when it is high, they dump the excess. This built-in thermostat is precisely why both deficiency and toxicity are rare.
So the most accurate framing is not "molybdenum deficiency is hard to get" but rather "molybdenum deficiency from diet does not occur in healthy people, and what little we know about acquired deficiency comes from a single famous medical case and from a rare genetic disorder that has nothing to do with how much molybdenum you eat."
Why Deficiency Is Essentially Never Seen
To understand why a genuinely essential mineral almost never runs short, it helps to know what molybdenum actually does — because the answer explains both why we need it and why we need so little.
Molybdenum itself is not the working part. The body uses it to build a small organic helper molecule called the molybdenum cofactor (often abbreviated Moco), a pterin-based scaffold that cradles a single molybdenum atom. Think of molybdenum as one rivet and the cofactor as the finished hinge: the rivet is useless on its own, and the hinge cannot work without it. Building that cofactor is a multi-step biochemical assembly line, elegantly mapped out in reviews by Mendel and Leimkühler. Once built, the cofactor slots into the active site of just four human enzymes:
- Sulfite oxidase — by far the most important. It performs the final step of breaking down the sulfur-containing amino acids (the ones in protein), converting toxic sulfite into harmless sulfate. This is the enzyme whose loss does real damage.
- Xanthine oxidase — breaks down purines into uric acid, part of recycling the building blocks of DNA.
- Aldehyde oxidase — helps process certain drugs and other compounds in the liver.
- Mitochondrial amidoxime-reducing component (mARC) — a more recently described enzyme involved in detoxification and nitrogen handling.
Now the key insight. These enzymes need only a trace of cofactor to do their jobs, and the cofactor is recycled rather than consumed. So the daily molybdenum requirement is minuscule. At the same time, molybdenum is naturally abundant in the plant foods that form the base of nearly every human diet — it is taken up from soil by legumes and grains in particular — so even a modest, monotonous diet delivers many times what the four enzymes need. Layer on top of that the kidney's conservation reflex (when intake drops, excretion drops to match), and you have a nutrient that is almost impossible to run out of through eating.
This is the difference between molybdenum and, say, iron or vitamin D. Iron is lost steadily through bleeding and turnover and is poorly absorbed, so shortfall is common. Vitamin D depends on sunlight that many people do not get. Molybdenum has no comparable drain and no comparable bottleneck. The combination of a tiny need, a generous and reliable food supply, and an efficient kidney thermostat is why — outside of artificial feeding and genetics — the deficiency simply has nowhere to come from.
Who, If Anyone, Actually Becomes Deficient
There are, in practice, only two situations in which the human body ends up short of usable molybdenum. Neither is something an ordinary person eating ordinary food can fall into.
1. Long-term total parenteral nutrition (TPN) without molybdenum. This is the source of the single most-cited human deficiency case, reported by Abumrad and colleagues in 1981. A man with a severe bowel disorder, Crohn's disease, was fed for many months entirely through a vein (TPN), on a formula that had not been supplemented with molybdenum. Over time he developed a striking picture: a fast heart rate and breathing, headache, night blindness, irritability, and ultimately a coma-like state. Blood tests showed he could not properly process sulfur-containing amino acids — exactly what you would predict if sulfite oxidase had run short of its cofactor. The crucial detail, and the reason the case is famous, is what fixed it: giving him supplemental molybdate (a molybdenum salt) reversed the entire syndrome. This was the experiment of nature (and necessity) that proved molybdenum is essential for humans. It is also, tellingly, essentially the only well-documented case of acquired dietary deficiency in the medical literature. Modern TPN formulas now routinely include trace molybdenum precisely so this never happens again, which is why even this edge case has become vanishingly rare.
2. People on prolonged, exclusive medical feeding more generally. The broader lesson is that the only realistic route to acquired molybdenum shortfall is total dependence on an artificial feeding source that omits it — long-term intravenous nutrition, or in principle a sole-source formula deliberately stripped of the mineral. Because clinical nutrition is now standardized to include trace elements, this is managed by dietitians and pharmacists as a matter of routine. It is not a scenario that arises from eating real food, however restricted or unbalanced that diet might be.
What you will not find on this list is anything resembling a normal human circumstance: not vegetarian or vegan diets, not low-protein diets, not aging, not common illnesses, not heavy exercise, not "poor soil." Molybdenum's abundance in plant foods means plant-forward diets, if anything, tend to be higher in it. There is no recognized population at dietary risk.
Molybdenum Cofactor Deficiency: The Genetic Disorder
The second — and far more serious — way a person can lack usable molybdenum is not about diet at all. It is a rare inherited disease called molybdenum cofactor deficiency (MoCD). Here the problem is not a shortage of the mineral but a broken assembly line: a mutation in one of the genes that build the cofactor (MOCS1, MOCS2, MOCS3, or GPHN) means the body cannot manufacture the cofactor even when molybdenum is plentiful. The rivet is there; the factory that turns it into a working hinge is not. The genetics of this disorder have been mapped in detail by Reiss and colleagues.
Because the cofactor is missing, all of the cofactor-dependent enzymes fail at once — most damagingly sulfite oxidase. Sulfite then accumulates to toxic levels, and because sulfite is harmful to the developing brain, MoCD typically appears within the first days of life as a devastating condition: severe seizures that do not respond to usual medications, feeding difficulty, exaggerated startle, and rapidly progressive brain injury. It is, sadly, often fatal in infancy. This is a genuinely rare disease — on the order of a few hundred reported cases worldwide — and it is the reason molybdenum's essentiality is taught at all in medicine: the catastrophe of having no usable cofactor stands in sharp contrast to the complete absence of any everyday dietary problem.
There is, importantly, a hopeful development. MoCD comes in subtypes, and the most common, type A, is caused by failure of an early step in cofactor synthesis that produces a precursor called cyclic pyranopterin monophosphate (cPMP). Because the missing precursor can be made and given as a drug, researchers tested replacing it directly. A prospective cohort study published in The Lancet in 2015 by Schwahn, Schwarz and colleagues showed that early treatment of MoCD type A with synthetic cPMP (fosdenopterin) dramatically reduced the toxic sulfite buildup and improved survival and neurological outcomes — a striking result for a previously untreatable disease, and one that led to an approved therapy. It is worth being clear about the boundary here: this is a treatment for a specific genetic enzyme defect in affected newborns. It has nothing to do with dietary molybdenum, and it is not relevant to anyone without this diagnosis. But it is a genuinely encouraging story and the most important recent advance in this corner of medicine.
When It Is Almost Certainly Not Molybdenum
If you searched your way here because a website, a supplement label, or a wellness video suggested that "molybdenum deficiency" might explain how you feel, it is worth saying gently and directly: based on everything above, that is almost certainly not what is going on. Symptoms commonly attributed to low molybdenum on the internet — fatigue, brain fog, headaches, sensitivity to sulfites in wine or food, mood changes, "trouble detoxifying" — are real experiences, but they are not features of any documented dietary molybdenum deficiency, and they have far more common and more checkable causes. Naming a symptom does not make it proof of a particular shortage; molybdenum, in particular, is one of the least likely culprits there is.
The more useful question is what else could be behind common symptoms. A few examples of explanations actually worth pursuing with a clinician:
- Persistent fatigue — far more often traces to iron deficiency or anemia, low vitamin B12 or vitamin D, thyroid problems, poor sleep, depression, or simply doing too much. A basic blood panel sorts most of this out. See Iron.
- Headaches — have their own large differential (tension, migraine, dehydration, caffeine, sleep, blood pressure) that has nothing to do with trace minerals.
- Sensitivity to sulfites in wine, dried fruit, or processed food — is a recognized reaction in some people, but it is an issue of sulfite intolerance, not of a molybdenum shortage; loading up on molybdenum supplements is not an established remedy and is not without its own risk.
- Digestive complaints and bloating — have common, treatable explanations of their own; for one example see SIBO.
This page exists, in part, to redirect a worry. The honest and most helpful message is that molybdenum is a solved problem for essentially everyone, and that energy spent worrying about it is better spent on the genuinely common deficiencies and conditions that a simple visit and a routine blood test can identify.
What You Actually Need to Do
For the overwhelming majority of people, the practical answer is wonderfully short: nothing special. If you eat any reasonably varied diet, you are getting several times the molybdenum you need, and there is no test to chase and no supplement to buy. Still, a few low-key, accurate pointers:
- Food more than covers it. Molybdenum is concentrated in lentils and other legumes, beans, peas, whole grains, nuts, and to a lesser degree in eggs and leafy vegetables. A single serving of beans or lentils can supply more than a full day's requirement. There is no need to eat these for their molybdenum — you will get plenty incidentally — but they are excellent foods for many other reasons.
- Supplements are generally unnecessary. Because deficiency does not occur from diet, routine molybdenum supplementation has no established benefit for healthy people. Standalone molybdenum supplements exist and are sold for various unproven claims; there is no good reason for most people to take them, and the mineral does have a tolerable upper intake level (set at 2,000 micrograms a day for adults) above which excess can cause problems. More is not better here. See the Molybdenum Toxicity page for the other end of the range.
- There is no routine blood test worth requesting. Molybdenum is not part of standard panels, and a level is not something a healthy person needs measured. (For context on what routine bloodwork actually covers, see the Comprehensive Metabolic Panel.)
- If you are fed only intravenously, long-term, that is the one situation where molybdenum genuinely matters — and it is already handled for you. Modern parenteral nutrition includes trace elements, including molybdenum, by design; your medical team manages this. You do not need to do anything beyond following their plan.
- If a newborn in your family has been diagnosed with molybdenum cofactor deficiency, that is an entirely different and serious situation requiring specialist metabolic care — not a dietary issue, and not something addressed by ordinary supplements. The treatment story for type A above is genuinely hopeful; the right path is an expert metabolic team.
In short: enjoy your beans and lentils, skip the molybdenum supplement, and direct any real symptoms to the common causes that a doctor can actually find and fix.
Related Nutrients & Pages
Molybdenum's biology connects it to a few other minerals worth a brief mention, mainly because the relationships occasionally come up:
- Copper. The clearest interaction runs in the other direction — high molybdenum intake can interfere with copper, not the reverse. In grazing livestock, molybdenum-rich pasture famously causes copper deficiency, and a molybdenum-copper-sulfur compound (tetrathiomolybdate) is even used medically to lower copper in Wilson's disease. For humans eating normal diets this is not a practical concern, but it is the reason molybdenum and Copper are discussed together.
- Sulfur. Because molybdenum's most important enzyme (sulfite oxidase) sits at the end of sulfur-amino-acid metabolism, molybdenum and Sulfur handling are biochemically linked — which is exactly why the rare cofactor disorder causes a toxic buildup of sulfite.
- Iron and zinc. When people worry about a trace-mineral shortfall, the deficiencies actually worth checking are usually Iron and sometimes Zinc — both of which, unlike molybdenum, do produce recognized human deficiency states.
- The molybdenum overview. For the full picture of what molybdenum is, where it comes from, and its role in the body, see the main Molybdenum page and its Benefits deep dive.
Key Research Papers
- Abumrad NN, Schneider AJ, Steel D, Rogers LS (1981). Amino acid intolerance during prolonged total parenteral nutrition reversed by molybdate therapy. The American Journal of Clinical Nutrition;34(11):2551-2559. — DOI: 10.1093/ajcn/34.11.2551
- Novotny JA (2011). Molybdenum Nutriture in Humans. Journal of Evidence-Based Complementary & Alternative Medicine;16(3):164-168. — DOI: 10.1177/2156587211406732
- Novotny JA, Turnlund JR (2007). Molybdenum Intake Influences Molybdenum Kinetics in Men. The Journal of Nutrition;137(1):37-42. — DOI: 10.1093/jn/137.1.37
- EFSA Panel on Dietetic Products, Nutrition and Allergies (2013). Scientific Opinion on Dietary Reference Values for molybdenum. EFSA Journal;11(8):3333. — DOI: 10.2903/j.efsa.2013.3333
- Mendel RR, Leimkühler S (2014). The biosynthesis of the molybdenum cofactors. JBIC Journal of Biological Inorganic Chemistry;20(2):337-347. — DOI: 10.1007/s00775-014-1173-y
- Reiss J (2000). Genetics of molybdenum cofactor deficiency. Human Genetics;106(2):157-163. — DOI: 10.1007/s004399900223
- Reiss J, Hahnewald R (2010). Molybdenum cofactor deficiency: Mutations in GPHN, MOCS1, and MOCS2. Human Mutation;32(1):10-18. — DOI: 10.1002/humu.21390
- Schwahn BC, Van Spronsen FJ, Belaidi AA, Bowhay S, Christodoulou J, et al. (2015). Efficacy and safety of cyclic pyranopterin monophosphate substitution in severe molybdenum cofactor deficiency type A: a prospective cohort study. The Lancet;386(10007):1955-1963. — DOI: 10.1016/S0140-6736(15)00124-5
- Johannes L, Fu CY, Schwarz G (2022). Molybdenum Cofactor Deficiency in Humans. Molecules;27(20):6896. — DOI: 10.3390/molecules27206896
PubMed Topic Searches
- PubMed — Molybdenum: human deficiency and nutrition
- PubMed — Molybdenum cofactor deficiency
- PubMed — Molybdenum and total parenteral nutrition
- PubMed — Sulfite oxidase deficiency
- PubMed — Cyclic pyranopterin monophosphate (fosdenopterin) therapy
Connections
- Molybdenum Overview
- Molybdenum Toxicity
- Molybdenum Benefits Hub
- Copper
- Sulfur
- Iron
- Zinc
- Comprehensive Metabolic Panel
- Lentils
- Eggs
- SIBO
- Neurology (Wilson's Disease & more)