Copper Deficiency: Nerve Damage and Balance
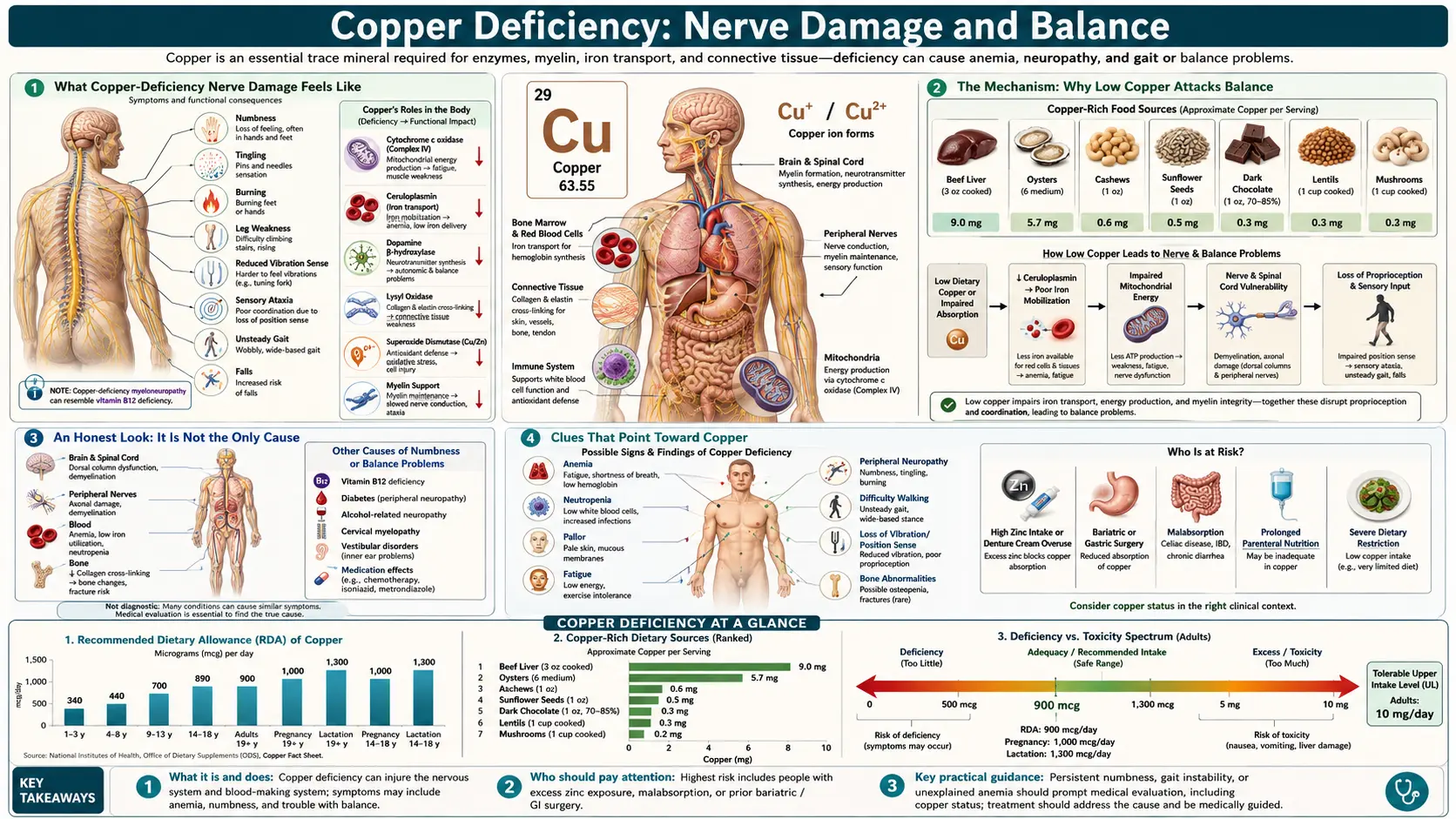
One of the most striking ways a copper deficiency can show itself is not in the blood but in the way a person walks. People describe feeling unsteady on their feet, especially in the dark or with their eyes closed; their feet feel numb, tingly, or as if they are walking on cotton; and their legs feel stiff and unreliable. Doctors call this pattern copper-deficiency myeloneuropathy — damage to both the spinal cord (myelo-) and the peripheral nerves (-neuropathy) — and it can look almost identical to the better-known nerve damage of vitamin B12 deficiency. This page explains what this kind of nerve damage feels like, why low copper specifically attacks the balance system, the other (more common) things that cause the same symptoms, the clues that point toward copper, and how it is diagnosed and treated. The single most important fact to carry away: nerve damage from copper deficiency can be halted by replacing copper, but any damage already done may not fully reverse — so it is found and treated early or not at all.
Table of Contents
- What Copper-Deficiency Nerve Damage Feels Like
- The Mechanism: Why Low Copper Attacks Balance
- An Honest Look: It Is Not the Only Cause
- Clues That Point Toward Copper
- What Drains Copper Low Enough to Hurt Nerves
- The Zinc Connection
- Getting Diagnosed
- Correcting Copper and Protecting Your Nerves
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
What Copper-Deficiency Nerve Damage Feels Like
The hallmark of copper-deficiency myeloneuropathy is a combination of numbness and unsteadiness that usually begins in the feet and creeps slowly upward over months. It is rarely sudden; people often realize in hindsight that it had been building for a long time. The most commonly reported experiences are:
- A “walking on cotton wool” feeling — the soles of the feet feel padded, distant, or wrapped, as though there were a layer between the foot and the floor. The ground does not feel solid.
- Numbness and tingling (paresthesia) — pins-and-needles, prickling, or buzzing, typically in both feet and lower legs in a symmetrical “stocking” distribution, sometimes reaching the hands in a “glove” pattern as it advances.
- Unsteadiness that is worse in the dark — this is the most telling clue. People feel reasonably steady when they can see their feet, but become wobbly washing their hair in the shower with eyes closed, walking to the bathroom at night, or in a dim room. Vision has been compensating for a balance sense that is failing.
- A wide-based, careful gait — the stance widens and the walk becomes cautious and stamping, as if testing each step. Others may notice it before the person does.
- Stiff, heavy, or “spastic” legs — because the spinal cord is involved, the legs can also feel tight, stiff, or jumpy, and reflexes at the knees and ankles may be brisk — an unusual mix of numbness and stiffness in the same person.
- Trouble with fine foot placement — tripping on curbs, catching the toes, or feeling clumsy on stairs and uneven ground.
Because the changes are gradual and often painless, they are frequently blamed on aging, arthritis, or being “out of shape.” The combination that should raise a flag is numb feet plus poor balance, especially balance that falls apart in the dark. That specific pairing is the signature of a problem in the body's position-sense pathways, and copper deficiency is one of its under-recognized causes.
The Mechanism: Why Low Copper Attacks Balance
To understand why copper matters here, it helps to know that your sense of balance does not come mainly from the inner ear — it comes from your body constantly reporting where your limbs are in space. This sense is called proprioception, and the information travels from sensors in your feet, ankles, and legs up a specific cable in the back of the spinal cord called the dorsal columns. Your brain blends this position information with vision and the inner ear to keep you upright. Close your eyes, and you are relying almost entirely on the dorsal-column signal. That is exactly why copper-deficiency balance problems get dramatically worse in the dark: the failing channel is the one that vision had been quietly covering for.
Copper is essential to keeping those nerve cables working, for two main reasons. First, copper is a required cofactor for an enzyme called cytochrome c oxidase, the final step in how mitochondria — the cell's power plants — turn oxygen into usable energy. Long nerve fibers running from the feet up the spinal cord are enormously energy-hungry; starve them of the copper-dependent machinery and the longest, most metabolically demanding fibers begin to fail first. Second, copper supports the health of myelin, the fatty insulation wrapped around nerve fibers that lets signals travel fast and cleanly. When copper runs low, this insulation degrades, and the dorsal columns and peripheral nerves — the position-sense pathway — are hit hardest.
An analogy. Picture the position-sense pathway as a long undersea telephone cable carrying a steady stream of “here is where your foot is” messages from your feet to your brain. Copper does two jobs along that cable: it runs the power stations that keep the signal strong, and it maintains the waterproof insulation around the wire. Pull copper out, and the most distant stretch of cable — the part farthest from shore, serving the feet — loses both its power and its insulation first. The messages arrive garbled or not at all. Your brain, no longer trusting the cable, leans hard on your eyes to know where your feet are. In daylight that works well enough; close your eyes and the deteriorated cable is all you have left — and you sway.
This is why the medical name is myeloneuropathy: myelopathy (the spinal-cord part, producing the stiffness, brisk reflexes, and position-sense loss) plus neuropathy (the peripheral-nerve part, producing the numbness and tingling in the feet). Both stem from the same underlying problem — nerve tissue deprived of the copper it needs to make energy and maintain insulation.
An Honest Look: It Is Not the Only Cause
It is important to be candid: numbness, tingling, and poor balance are extremely common symptoms with many causes, and copper deficiency is one of the rarer ones. Most people with these complaints do not have low copper. The far more common explanations include:
- Vitamin B12 deficiency — this is the single most important look-alike. Low B12 causes a condition called subacute combined degeneration of the spinal cord that damages the very same dorsal columns, producing a nearly identical picture of numb feet and balance loss in the dark. Copper-deficiency myelopathy was described in the medical literature precisely because it mimics B12 deficiency so closely — and the two can even occur together. Any thorough workup checks both.
- Diabetes — diabetic peripheral neuropathy is by far the most common cause of numb, tingling feet worldwide. Long-standing high blood sugar is the first thing most clinicians consider.
- Alcohol — heavy alcohol use damages peripheral nerves directly and through associated nutritional deficiencies.
- Other causes — thyroid disease, kidney disease, certain medications and chemotherapy drugs, nerve compression (such as a pinched nerve in the spine), and a long list of other neuropathies. Sometimes no cause is ever found.
So a tingling foot is not proof of copper deficiency, and it would be wrong to assume it. The value of knowing about copper is different: it belongs on the checklist of treatable causes that are easy to miss, particularly the ones that mimic B12 deficiency. The mistake that costs people is the reverse error — treating “B12-deficiency-like” nerve damage, finding the B12 is actually normal, and never going on to check copper while the real, fixable cause keeps doing damage.
Clues That Point Toward Copper
Certain features make copper deficiency more likely and should prompt a copper level to be checked, rather than assuming it is “just neuropathy”:
- A B12-like syndrome with a normal B12 level. When someone has the classic numb-feet-and-poor-balance picture of subacute combined degeneration but their vitamin B12 is normal, copper deficiency moves to the front of the line.
- An unexplained blood-count abnormality at the same time. Copper deficiency very often causes a low blood count alongside the nerve problem — anemia and a low white-cell count (especially low neutrophils). The combination of numb, unsteady feet plus an unexplained anemia or low white count is a strong hint, and is covered on the sibling page Copper Deficiency: Anemia and Low White Cells.
- A history of heavy zinc intake. Excess zinc — from supplements, multiple cold remedies, or ill-fitting-denture adhesive creams used in large amounts — is a leading cause of acquired copper deficiency (see the next section).
- Previous stomach or weight-loss (bariatric) surgery. Operations that bypass the upper small intestine, where copper is absorbed, are a well-recognized setup for copper deficiency that can appear years later.
- Other signs of copper deficiency. Brittle, lighter, or depigmenting hair and skin (see Hair and Skin Pigment) or fragile connective tissue (see Bone and Connective Tissue) add weight to the picture.
None of these is proof by itself, but two or more together — for example, balance trouble plus an unexplained anemia plus years of high-dose zinc — make copper deficiency likely enough that a simple blood test is clearly worthwhile.
What Drains Copper Low Enough to Hurt Nerves
Healthy adults rarely become copper deficient from diet alone, because copper is widely available in food (organ meats, shellfish, nuts, seeds, whole grains, and dark chocolate) and the body holds reserves. Nerve-damaging deficiency almost always points to a specific, identifiable reason:
- Excess zinc — the most common acquired cause. Zinc and copper compete for absorption, and too much zinc blocks copper uptake in the gut (the mechanism is detailed below). Sources include high-dose zinc supplements, frequent zinc lozenges, and — a classic and easily-missed culprit — large quantities of zinc-containing denture adhesive cream.
- Upper-gastrointestinal (bariatric) surgery — gastric bypass and similar weight-loss operations remove or bypass the stomach and upper small intestine, exactly where copper is absorbed. Copper deficiency can surface months to years after surgery and is a recognized cause of myeloneuropathy in this group.
- Other malabsorption — celiac disease, prior stomach surgery for other reasons, chronic severe diarrhea, and inflammatory bowel disease can all impair copper uptake.
- Long-term tube or intravenous feeding — people fed entirely by vein (total parenteral nutrition) can become deficient if copper is not adequately supplied in the formula.
- Very high iron intake — like zinc, large amounts of iron can interfere with copper absorption.
Identifying which of these is at work matters enormously, because fixing the cause is part of the cure — stopping a zinc source is very different from managing copper after bariatric surgery, and both differ from treating malabsorption.
The Zinc Connection
The relationship between zinc and copper deserves its own section, because excess zinc is the cause people most often stumble into without realizing it. Zinc and copper are absorbed in the same part of the small intestine and effectively compete. When zinc intake is high, the cells lining the gut ramp up production of a copper-trapping protein called metallothionein. Metallothionein binds copper tightly inside those gut cells; instead of passing into the bloodstream, the bound copper is shed back into the gut as the cells are naturally sloughed off — carrying the copper out of the body. Sustained over months, this quietly starves the body of copper while zinc levels stay high or even elevated.
This is more than a theoretical worry. The medical literature includes a memorable line of cases in which people developed disabling myeloneuropathy from using large amounts of zinc-containing denture adhesive cream over long periods — the zinc absorbed from the cream was enough to drive copper down and damage the spinal cord. High-dose zinc supplements taken for colds, immunity, or skin, and zinc lozenges used frequently, can do the same. This is also why the zinc-excess and copper-deficiency stories are two sides of one coin: the topic is covered from the zinc side on Zinc Toxicity: Copper Deficiency and from the toxicity hub at Zinc Toxicity.
The practical takeaways are simple. Zinc is an essential nutrient and ordinary dietary or modest supplemental amounts are not the problem — the danger is chronic high doses. If you take zinc, keep the dose sensible and time-limited, do not stack multiple zinc products at once, switch to a low- or zinc-free denture adhesive and use only a thin amount, and if you must take high-dose zinc long term under medical advice, your clinician may monitor copper. When copper is being replaced to treat nerve damage, removing the zinc source is an essential part of the fix — replacing copper while excess zinc continues will not work.
Getting Diagnosed
The good news is that confirming copper deficiency is straightforward and inexpensive once someone thinks to look for it. The core tests are simple blood draws:
- Serum copper — the direct measure; it is low in deficiency.
- Ceruloplasmin — the main copper-carrying protein in blood, which is also low in copper deficiency and helps confirm the picture. (Copper and ceruloplasmin are explained in depth on The Relationship Between Hemoglobin and Ceruloplasmin and on Copper, Hemoglobin and Ceruloplasmin.)
- Serum zinc — checked at the same time, because a high zinc level points straight to the cause.
- A complete blood count (CBC) — to look for the anemia and low white-cell count that so often accompany copper-deficiency nerve damage.
- Vitamin B12 — essentially always checked alongside, because the two conditions look so alike and can coexist.
Copper and ceruloplasmin are specialized tests and are not part of a routine Comprehensive Metabolic Panel, so they have to be ordered specifically — which is exactly why the diagnosis is missed when no one thinks of copper. Beyond blood work, a neurologist may confirm the pattern of nerve damage with nerve conduction studies and an MRI of the spine, which can show a characteristic bright signal in the dorsal columns of the cervical spinal cord — the same MRI appearance seen in B12 deficiency, reinforcing how closely the two mimic each other. The point for patients is reassuring: if copper is on the radar, a few targeted tests settle the question quickly.
Correcting Copper and Protecting Your Nerves
Treatment has two equally important halves: replace the copper and remove whatever was draining it. Done together, they reliably stop the deficiency from progressing.
- Remove the cause first and foremost. If excess zinc is the driver, stopping the zinc source — high-dose supplements, frequent lozenges, or zinc-laden denture cream — is essential. Replacing copper while zinc continues to block its absorption simply does not work.
- Copper supplementation. Copper is replaced with oral copper (often as copper gluconate or copper sulfate) under medical guidance; doses are higher at first to refill stores, then lowered for maintenance. When the deficiency is severe or the gut cannot absorb well, copper can be given intravenously to correct it faster. Blood copper and ceruloplasmin are rechecked to confirm levels are rising.
- Food matters for the long run. Once stores are restored, copper-rich foods help keep them there: shellfish (especially oysters), organ meats such as liver, nuts and seeds (cashews, sunflower and sesame seeds), whole grains, legumes, and dark chocolate. The food sources are detailed on Copper Food Sources.
- Monitor and be patient. Blood counts (the anemia and low white count) usually recover well and fairly quickly once copper is replaced. The nerve recovery is the part to be realistic about.
Here is the honest and most important expectation to set: replacing copper halts the progression of the nerve damage and stabilizes most people, and some regain function — but neurological recovery is often partial, and damage already done to the spinal cord may not fully reverse. The degree of recovery depends heavily on how long the deficiency went unrecognized. This is precisely why the symptoms above are worth taking seriously early: the window in which treatment can protect function is real, but it does not stay open indefinitely. Copper deficiency is one of those conditions where finding it sooner genuinely changes the outcome.
For broader context on copper's role in the nervous system, see Copper and Neurological Health and the Copper overview.
When to Seek Care / Red Flags
Copper-deficiency nerve damage develops slowly, so it is usually a matter for a prompt (not emergency) medical evaluation. See a clinician without delay if you have:
- Numbness, tingling, or a “walking on cotton” feeling in both feet that has been building over weeks to months — especially if it is climbing up the legs.
- New unsteadiness or frequent stumbling, particularly in the dark or when your eyes are closed (showering, getting up at night).
- Numb, unsteady feet together with an unexplained anemia or low white-cell count — the combination that especially points toward copper.
- Nerve symptoms after weight-loss (bariatric) or other upper-gut surgery, or in anyone using large amounts of zinc supplements or zinc-containing denture cream.
- Nerve symptoms that were attributed to B12 deficiency but did not improve, or where the B12 level turned out to be normal — ask specifically about checking copper.
Treat it as more urgent — seek care promptly the same day — if balance loss is worsening quickly, if you are having falls, or if weakness, numbness, or unsteadiness is climbing rapidly up the body, since fast-progressing spinal-cord and nerve symptoms always warrant urgent assessment to rule out other serious causes. The recurring theme is the same throughout this page: copper-deficiency nerve damage is treatable, but the recovery you can expect depends on catching it early — so unexplained numb feet and failing balance are worth investigating rather than waiting out.
Key Research Papers
- Kumar N (2006). Copper Deficiency Myelopathy (Human Swayback). Mayo Clinic Proceedings;81(10):1371-1384. — DOI: 10.4065/81.10.1371
- Kumar N, Gross JB Jr, Ahlskog JE (2004). Copper deficiency myelopathy produces a clinical picture like subacute combined degeneration. Neurology;63(1):33-39. — DOI: 10.1212/01.wnl.0000132644.52613.fa
- Kumar N, Crum B, Petersen RC, Vernino SA, Ahlskog JE (2004). Copper Deficiency Myelopathy. Archives of Neurology;61(5):762-766. — DOI: 10.1001/archneur.61.5.762
- Jaiser SR, Winston GP (2010). Copper deficiency myelopathy. Journal of Neurology;257(6):869-881. — DOI: 10.1007/s00415-010-5511-x
- Winston GP, Jaiser SR (2008). Copper deficiency myelopathy and subacute combined degeneration of the cord — why is the phenotype so similar? Medical Hypotheses;71(2):229-236. — DOI: 10.1016/j.mehy.2008.03.027
- Halfdanarson TR, Kumar N, Li CY, Phyliky RL, Hogan WJ (2008). Hematological manifestations of copper deficiency: a retrospective review. European Journal of Haematology;80(6):523-531. — DOI: 10.1111/j.1600-0609.2008.01050.x
- Hedera P, Peltier A, Fink JK, Wilcock S, London Z, Brewer GJ (2009). Myelopolyneuropathy and pancytopenia due to copper deficiency and high zinc levels of unknown origin II: the denture cream is a primary source of excessive zinc. NeuroToxicology;30(6):996-999. — DOI: 10.1016/j.neuro.2009.08.008
- Zittel S, Ufer F, Gerloff C, Münchau A, Rosenkranz M (2014). Severe myelopathy after denture cream use — is copper deficiency or excess zinc the cause? Clinical Neurology and Neurosurgery;121:17-18. — DOI: 10.1016/j.clineuro.2014.03.013
- Arnold AJ, Tkach A, Wile DJ (2019). Copper deficiency myeloneuropathy in a patient with previous bariatric surgery. Canadian Medical Association Journal;191(31):E866. — DOI: 10.1503/cmaj.190168
- Rapoport Y, Lavin PJM (2016). Nutritional Optic Neuropathy Caused by Copper Deficiency After Bariatric Surgery. Journal of Neuro-Ophthalmology;36(2):178-181. — DOI: 10.1097/wno.0000000000000333
- National Institutes of Health, Office of Dietary Supplements. Copper — Health Professional Fact Sheet. — ods.od.nih.gov
PubMed Topic Searches
- PubMed — Copper deficiency myeloneuropathy
- PubMed — Copper deficiency myelopathy and subacute combined degeneration
- PubMed — Zinc-induced copper deficiency, neurological
- PubMed — Copper deficiency after bariatric surgery
- PubMed — Denture-cream zinc and copper-deficiency neuropathy
Connections
- Copper Deficiency Symptom Hub
- Copper Deficiency: Anemia & Low White Cells
- Copper Deficiency: Bone & Connective Tissue
- Copper Deficiency: Hair & Skin Pigment
- Copper Overview
- Copper Toxicity (Excess)
- Copper and Neurological Health
- Hemoglobin and Ceruloplasmin
- Copper Food Sources
- Zinc
- Zinc Toxicity
- Zinc Toxicity: Copper Deficiency
- Iron
- Vitamin B12
- Peripheral Neuropathy
- Comprehensive Metabolic Panel