Chloride: The Overlooked Essential Electrolyte
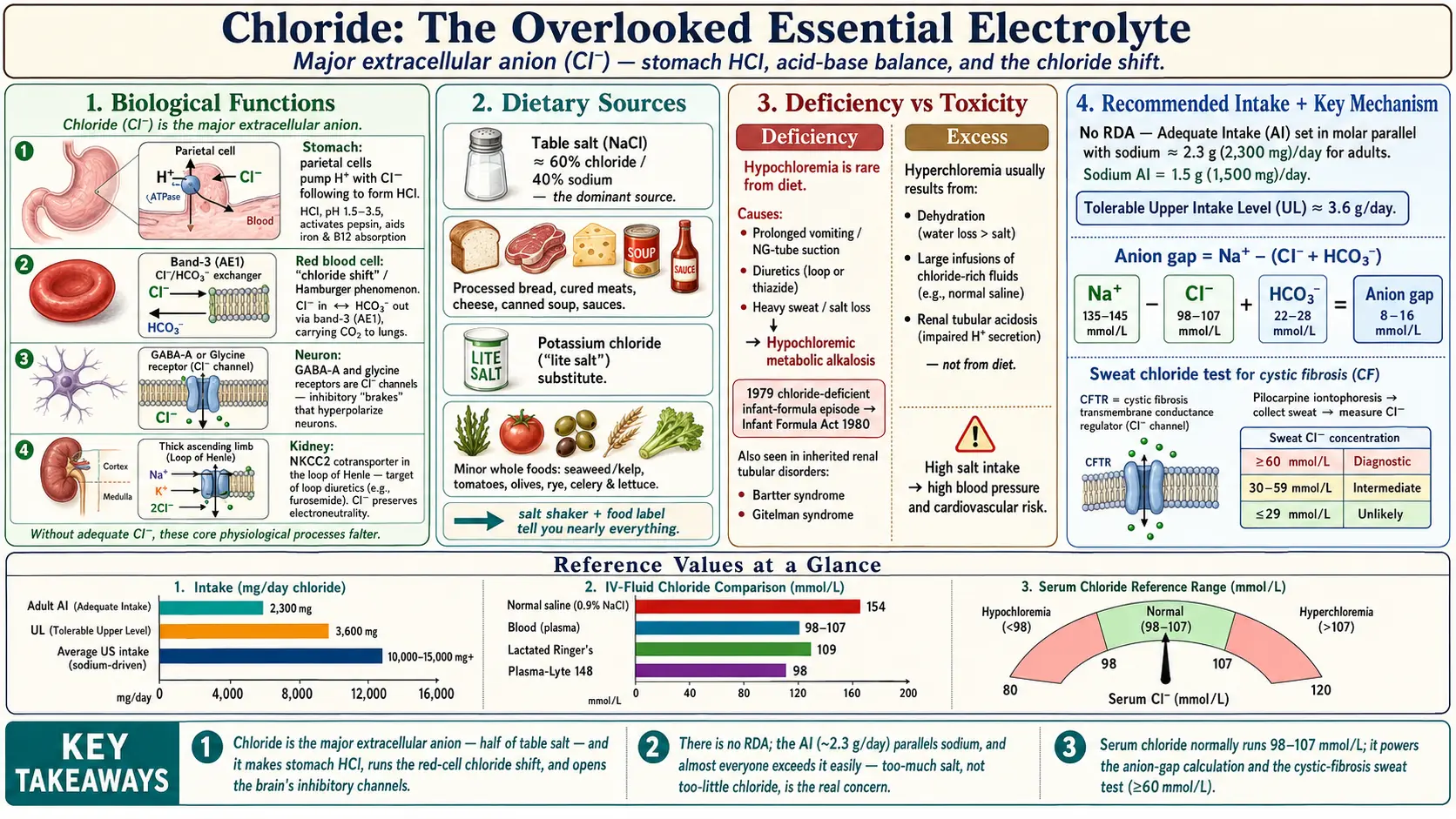
Table of Contents
- Overview
- Biological Functions
- Dietary Sources
- Deficiency
- Recommended Intake
- Supplementation & Forms
- Toxicity & Upper Limit
- Special Considerations
- Key Research Papers
- Connections
- Featured Videos
1. Overview
When people think about the minerals that keep them alive, chloride almost never makes the list. Sodium gets the headlines, potassium gets the bananas, and chloride — the other half of ordinary table salt — quietly does some of the body's most important work without ever being noticed. That is a shame, because chloride (written Cl−, a chlorine atom that has picked up one extra electron and carries a negative charge) is genuinely essential. You would not survive without it.
Chloride is the major extracellular anion — the most abundant negatively charged particle in the fluid outside your cells, including your blood plasma and the fluid that bathes your tissues. It is the counterweight to sodium, the most abundant positively charged particle in that same compartment. Because opposite charges must balance, sodium and chloride move together through much of the body's plumbing, and together they set the volume and concentration (osmolality) of your extracellular fluid. That, in turn, helps determine your blood volume and contributes to your blood pressure. Where sodium and chloride go, water follows.
But chloride is far more than sodium's silent partner. It is the acid in your stomach acid, a key player in the moment-to-moment chemistry that keeps your blood from turning too acidic or too alkaline, and the working substance of the inhibitory brakes in your nervous system. A defective chloride channel is the single molecular cause of cystic fibrosis. And the everyday hospital decision of which intravenous fluid to hang — old-fashioned "normal saline" versus a "balanced" solution — is, at its heart, a debate about how much chloride to give a sick patient.
This page lays out what chloride actually does, where it comes from (overwhelmingly, salt), why deficiency is rare but instructive when it happens, how much you need, and why the most important "chloride problems" in medicine are about balance — too much or too little relative to the body's other charged particles — rather than dietary poisoning.
2. Biological Functions
Chloride contributes to four distinct and vital systems. Understanding them is the best way to appreciate why an electrolyte most people have never thought about is something your body cannot do without.
Stomach acid: the chloride in hydrochloric acid
The acid in your stomach is hydrochloric acid (HCl), and the "chloric" half of that name is chloride. Specialized parietal cells in the stomach lining pump hydrogen ions (H+) into the stomach cavity, and chloride follows through dedicated channels to make the strong acid. The result is a stomach interior with a pH around 1.5 to 3.5 — acidic enough to do several jobs at once. It begins unfolding dietary proteins so digestive enzymes can attack them, activates pepsin (the stomach's main protein-digesting enzyme, which only works in an acidic environment), and helps liberate nutrients that are tightly bound to food. That acidic environment is important for absorbing iron and is a necessary step in releasing vitamin B12 from food protein. Stomach acid is also a frontline defense: it kills or disables many of the bacteria, viruses, and parasites that arrive with food. People who chronically suppress stomach acid — for instance with long-term acid-blocking medication — can over time see consequences for iron and B12 status, which underscores that the chloride-driven acidity is doing real physiological work.
Acid–base balance and the red-cell "chloride shift"
Your blood must hold a remarkably steady pH of about 7.35 to 7.45, and chloride is one of the levers the body uses to keep it there. The most elegant example is the chloride shift, sometimes called the Hamburger phenomenon after the physiologist who described it. As your tissues produce carbon dioxide, that CO2 diffuses into red blood cells and is rapidly converted into bicarbonate (HCO3−). To keep the inside and outside of the cell electrically balanced as bicarbonate floods out into the plasma, a chloride ion moves in to take its place — a one-for-one swap handled by a transport protein in the red-cell membrane (the band 3 anion exchanger, also called AE1). When the blood reaches the lungs and unloads CO2, the whole exchange runs in reverse. This continuous traffic of chloride in and out of red cells is a quiet, indispensable part of how your blood carries the body's CO2 to the lungs to be exhaled.
Nerve and muscle signaling: chloride channels as the body's brakes
If sodium and potassium are the accelerators of the nervous system, chloride is largely the brake. The two most important inhibitory neurotransmitter systems in the brain and spinal cord work by opening chloride channels. The GABA-A receptor (the target of substances such as benzodiazepines and many anesthetics) and the glycine receptor are both, physically, channels that let chloride flow across the nerve-cell membrane. When chloride moves into a neuron through these channels, it makes the cell harder to fire — calming, dampening, and preventing runaway electrical activity. This inhibition is what keeps the nervous system from seizing up; it is fundamental to muscle tone, coordinated movement, and a stable, regulated brain.
Kidney handling and electroneutrality
The kidneys filter the entire blood volume many times a day and must reclaim almost all of the chloride that passes through, fine-tuning the exact amount returned to the body. A central player is the sodium-potassium-chloride cotransporter (NKCC2) in the thick ascending limb of the loop of Henle, which hauls sodium, potassium, and chloride back out of the forming urine together. This transporter is the precise target of the powerful loop diuretics (such as furosemide): by blocking it, those drugs make the body excrete sodium, chloride, and water, which is how they relieve fluid overload in heart failure. Throughout the kidney, chloride moves alongside positively charged ions to preserve electroneutrality — the unbreakable rule that the total positive and negative charges in body fluid must balance. Chloride's mobility makes it the body's most important "balancing" ion.
3. Dietary Sources
Chloride is one of the easiest nutrients in the world to obtain, for one simple reason: it comes paired with sodium in table salt. Common salt is sodium chloride, and by weight it is roughly 60% chloride and 40% sodium. That means every time you eat salt — in cooking, at the table, or, far more often, hidden inside packaged and restaurant food — you are eating a large dose of chloride at the same time.
Salt and processed foods dominate
Because the modern food supply is so salt-rich, the overwhelming majority of dietary chloride comes from the same places as dietary sodium: breads, cured and processed meats, cheeses, canned soups, snack foods, sauces, condiments, and restaurant meals. There is no need to seek chloride out; if you are getting enough sodium (and almost everyone in industrialized countries gets more than enough), you are getting plenty of chloride too. For most people, the practical concern is the same one that applies to sodium — the health effects of too much salt — rather than any worry about getting enough chloride.
Salt substitutes and whole foods
A second notable source is potassium chloride, the main ingredient in most "salt substitutes" and "lite salts." These products swap some or all of the sodium for potassium while still delivering chloride, which is why they taste salty. They can be useful for people trying to lower sodium — though anyone with kidney disease or on certain blood-pressure medications should check with a clinician first, because added potassium can be risky for them. Beyond added salt, smaller amounts of chloride occur naturally in a range of whole foods, including:
- Sea vegetables such as seaweed and kelp;
- Tomatoes and tomato products;
- Olives (and many other brined or pickled foods);
- Rye and some other grains;
- Lettuce, celery, and other vegetables.
These natural sources contribute, but they are dwarfed by the chloride that arrives as salt. In practical terms, the salt shaker and the food label tell you almost everything you need to know about your chloride intake.
4. Deficiency
Because chloride is so abundant in the diet, true dietary chloride deficiency is rare in healthy people. When blood chloride does run low (hypochloremia), it is usually because too much was lost — through prolonged vomiting, nasogastric suction, diuretics, or heavy sweating — or because of an inherited salt-wasting disorder, and the body often tips toward being too alkaline as a result. For a full, patient-friendly guide to the symptoms, causes, and treatment of low chloride, see Hypochloremia (Low Chloride): Symptoms, Causes, and Recovery. The opposite problem — too much chloride in the blood — is covered in Hyperchloremia (High Chloride): What the Evidence Shows.
5. Recommended Intake
There is no Recommended Dietary Allowance (RDA) for chloride, because there was never enough evidence to set one. Instead, the U.S. National Academies define an Adequate Intake (AI) — a level judged sufficient to meet the body's needs. The chloride AI is deliberately set in parallel with the sodium AI, on a one-to-one molar (particle-for-particle) basis, because the two are consumed together as salt.
The numbers
For healthy adults, the AI for chloride is approximately 2.3 grams (2,300 mg) per day, corresponding to the adult sodium AI of 1.5 grams (1,500 mg) per day. (Chloride is the heavier of the two atoms, which is why its gram figure is larger even though the number of particles is matched.) The chloride AI declines with older age, mirroring the lower sodium AI set for older adults, and is lower for children. These are reference values for adequacy, not targets you need to chase.
Why almost no one falls short
In practice, essentially everyone in the United States and other industrialized countries meets the chloride AI easily, because typical salt intake far exceeds it. Average sodium intake in U.S. adults is around 3,400 mg per day — and the chloride that comes with that salt is correspondingly high. For the vast majority of people, then, the chloride AI is not a goal to reach but a floor they clear without trying. The genuine public-health concern with salt is the upper end of intake, not the lower — which brings us to chloride's tolerable upper limit.
6. Supplementation & Forms
Chloride is one of the very few essential minerals that almost no one needs to supplement deliberately. Because it travels with sodium in everyday salt, a normal diet supplies far more than enough, and there is no routine reason for a healthy person to take a chloride pill. When chloride is replaced, it is almost always as a treatment for a specific medical problem — managed by a clinician, alongside fluids and other electrolytes, rather than as a standalone "supplement."
How chloride is replaced when it is needed
- Sodium chloride (saline). The most common way to give chloride is as intravenous saline — salt water — used to restore fluid volume and correct sodium-and-chloride losses from vomiting, diarrhea, bleeding, or dehydration. In this setting chloride is not the explicit goal; it comes along with the sodium and water the patient needs.
- Potassium chloride (KCl). When someone is short of potassium (for example, from diuretics or vomiting), the standard replacement is potassium chloride, which conveniently restores chloride at the same time. It is given as tablets, liquid, or, in hospital, as a carefully controlled intravenous infusion. Potassium chloride is also the active ingredient in most salt substitutes.
- Other chloride salts. In specific situations a clinician may use ammonium chloride or arginine chloride to treat a chloride-deficient alkalosis, or hydrochloric acid infusions for severe cases — but these are specialized hospital interventions, not everyday remedies.
The bottom line on supplementation
For the general public, the honest message is that chloride supplementation is essentially never necessary. Chloride is managed by the body — and, when something goes wrong, by the medical team — alongside sodium, potassium, and fluid status. There is no evidence that taking extra chloride benefits a healthy person, and because chloride comes packaged with sodium, any attempt to "boost" it would mean eating more salt, which for most people is the opposite of what their health calls for.
7. Toxicity & Upper Limit
You cannot really suffer "chloride poisoning" from food: the risk of high chloride intake is essentially the risk of high salt intake, which is why the U.S. National Academies set chloride's Tolerable Upper Intake Level (about 3.6 g/day for adults) in parallel with sodium — and the practical message is that most people should eat less salt, not more. A high blood chloride level (hyperchloremia) almost never means a person ate too much; far more often it reflects dehydration, large-volume saline infusions, or an acid–base disorder. For the full evidence on high chloride, see Hyperchloremia (High Chloride): What the Evidence Shows, and for the low end see Hypochloremia (Low Chloride): Symptoms, Causes, and Recovery.
8. Special Considerations
Chloride rarely makes the news, but it sits at the center of several important issues in laboratory medicine and hospital care. Three are worth understanding.
Reading a chloride result on a blood test
Chloride is part of the standard basic metabolic panel (the "electrolytes" on routine bloodwork). The normal serum chloride range is roughly 98 to 107 mmol/L (laboratories vary slightly). A result above that range is hyperchloremia; below it is hypochloremia. On its own, a chloride value is rarely diagnostic — its real power comes from how it relates to the body's other ions, which is why clinicians read it alongside sodium and bicarbonate rather than in isolation.
The anion gap
One of the most useful calculations in all of clinical medicine leans directly on chloride: the anion gap. It is computed as the sodium concentration minus the sum of the chloride and bicarbonate concentrations:
Anion gap = Na+ − (Cl− + HCO3−)
Because the body's fluids must be electrically neutral, the gap reflects the "unmeasured" anions that the routine panel does not directly report. When a patient is acidotic, the anion gap tells the doctor a great deal about why. A high anion gap points to acids accumulating in the body (as in diabetic ketoacidosis, lactic acidosis, or certain poisonings). A normal (or "non-gap") acidosis — one in which the chloride rises to fill the space left by lost bicarbonate — points instead to causes such as severe diarrhea (which loses bicarbonate) or renal tubular acidosis. Chloride, the humble balancing ion, is what makes this diagnostic shortcut work.
Saline versus balanced crystalloids: a real clinical debate
Perhaps the most consequential modern question involving chloride is which intravenous fluid a sick patient should receive. For decades the default was 0.9% sodium chloride — misleadingly nicknamed "normal" saline. It is not, in fact, physiologically normal: it contains about 154 mmol/L of chloride, considerably more than the roughly 98–107 mmol/L in blood. Infusing large volumes of it can drive up the blood chloride and produce a hyperchloremic metabolic acidosis, a phenomenon documented in controlled human studies. The alternative is a class of balanced crystalloids — fluids such as lactated Ringer's and Plasma-Lyte — whose chloride content is closer to that of blood and which include a bicarbonate-like buffer.
The honest, evidence-based picture is that this matters, but the size of the effect is still debated. Several large trials — including the SMART and SALT-ED studies in 2018 — found modestly better kidney-related outcomes with balanced fluids than with saline in many patients, while the earlier SPLIT trial found no significant difference in acute kidney injury. The weight of evidence has nudged many hospitals toward balanced solutions as the default for routine resuscitation, with saline reserved for specific situations. For a general reader the takeaway is simple and a little surprising: the chloride content of a bag of salt water is a real clinical variable that researchers are actively studying — one more sign that this overlooked electrolyte deserves more credit than it gets.
9. Key Research Papers
- Berend K, van Hulsteijn LH, Gans ROB. Chloride: The queen of electrolytes? European Journal of Internal Medicine. 2012;23(3):203–211. doi:10.1016/j.ejim.2011.11.013
- Nagami GT. Hyperchloremia — Why and how. Nefrología. 2016;36(4):347–353. doi:10.1016/j.nefro.2016.04.001
- Hamm LL, Nakhoul N, Hering-Smith KS. Acid-Base Homeostasis. Clinical Journal of the American Society of Nephrology. 2015;10(12):2232–2242. doi:10.2215/CJN.07400715
- Scheingraber S, Rehm M, Sehmisch C, Finsterer U. Rapid Saline Infusion Produces Hyperchloremic Acidosis in Patients Undergoing Gynecologic Surgery. Anesthesiology. 1999;90(5):1265–1270. doi:10.1097/00000542-199905000-00003
- Semler MW, Self WH, Wanderer JP, et al. Balanced Crystalloids versus Saline in Critically Ill Adults (SMART). New England Journal of Medicine. 2018;378(9):829–839. doi:10.1056/NEJMoa1711584
- Self WH, Semler MW, Wanderer JP, et al. Balanced Crystalloids versus Saline in Noncritically Ill Adults (SALT-ED). New England Journal of Medicine. 2018;378(9):819–828. doi:10.1056/NEJMoa1711586
- Young P, Bailey M, Beasley R, et al. Effect of a Buffered Crystalloid Solution vs Saline on Acute Kidney Injury Among Patients in the Intensive Care Unit (SPLIT). JAMA. 2015;314(16):1701–1710. doi:10.1001/jama.2015.12334
- Ma Y, He FJ, Sun Q, et al. Joint association of urinary sodium and potassium excretion with cardiovascular events and mortality: prospective cohort study. BMJ. 2019;364:l772. doi:10.1136/bmj.l772
- Roy S 3rd, Arant BS Jr. Hypochloremic Metabolic Alkalosis in a Chloride-Deficient Infant (commentary on the 1979 formula episode). Nutrition Reviews. 1980;38(3):112–114. doi:10.1111/j.1753-4887.1980.tb05899.x
- Roy S 3rd, Arant BS Jr. Failure to Thrive and Metabolic Alkalosis: Hypochloremia–Hypokalemia Syndrome in Infants Fed a Chloride-Deficient Formula. JAMA. 1980;243(15):1554. doi:10.1001/jama.1980.03300360040024
- Farrell PM, White TB, Ren CL, et al. Diagnosis of Cystic Fibrosis: Consensus Guidelines from the Cystic Fibrosis Foundation. The Journal of Pediatrics. 2017;181S:S4–S15.e1. doi:10.1016/j.jpeds.2016.09.064
- Baumer JH. Guidelines for the performance of the sweat test for the diagnosis of cystic fibrosis. Annals of Clinical Biochemistry. 2007;44(Pt 1):25–34. doi:10.1258/000456307779596011
- National Academies of Sciences, Engineering, and Medicine. Dietary Reference Intakes for Sodium and Potassium. Washington, DC: The National Academies Press; 2019. (Chloride Adequate Intake and Tolerable Upper Intake Level are set in molar parallel with sodium.) National Academies / NCBI Bookshelf
- U.S. National Library of Medicine, MedlinePlus. Chloride in diet; Chloride blood test (serum chloride reference range and clinical interpretation). MedlinePlus — Chloride in diet
Connections
- Hypochloremia (Low Chloride)
- Hyperchloremia (High Chloride)
- All Minerals
- Sodium
- Potassium
- Magnesium
- Calcium
- Phosphorus
- Iodine
- Toxic Minerals
- Lab Tests
- Kidney Disease
- Hypertension