MTHFR Gene Mutation Testing
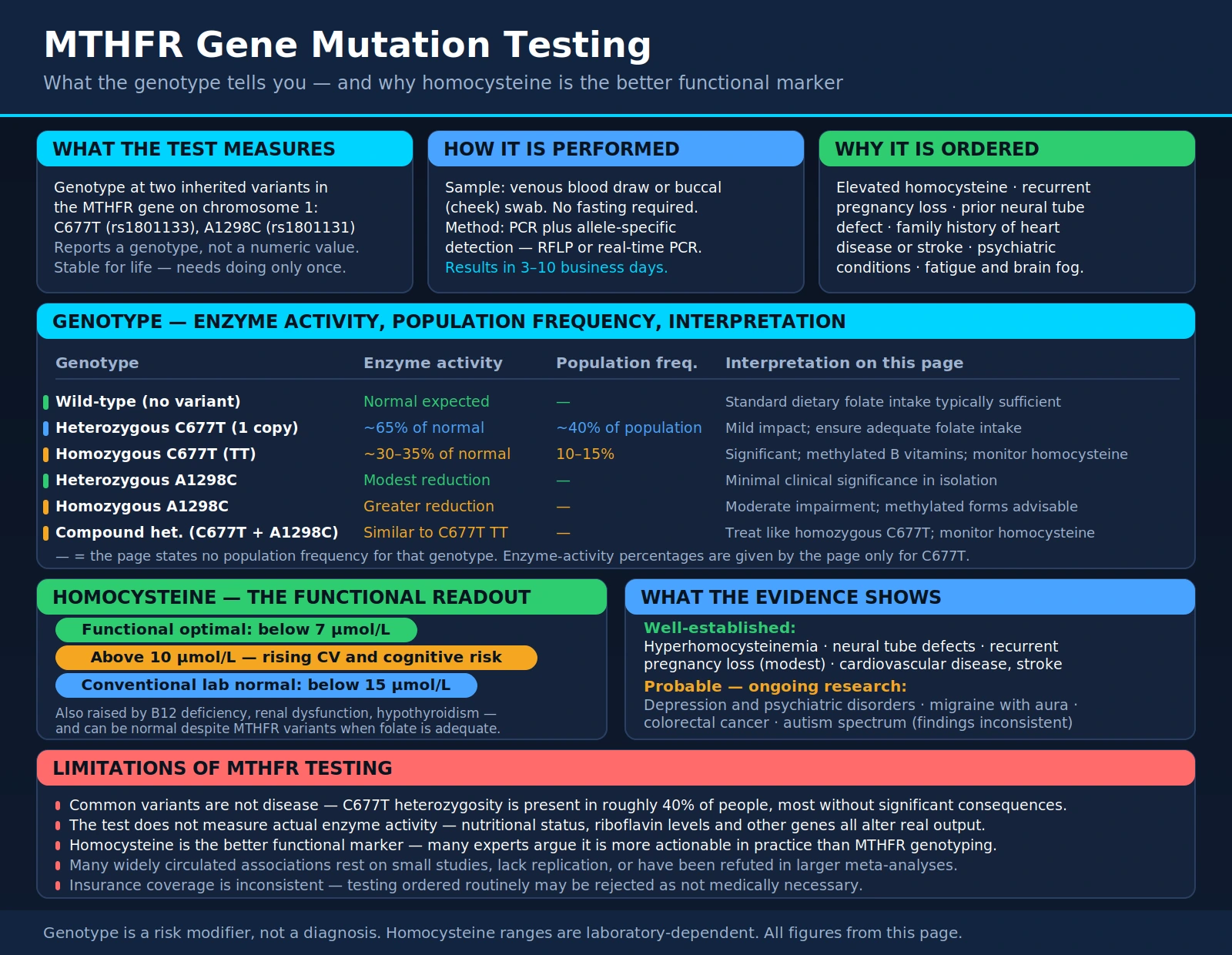
Table of Contents
- What MTHFR Gene Testing Measures
- Why MTHFR Testing Is Ordered
- How the Test Is Performed
- MTHFR Variants: C677T and A1298C
- Reference Ranges and Result Interpretation
- Conditions Associated With MTHFR Mutations
- The Methylation Cycle Explained
- The Homocysteine Connection
- How to Improve Outcomes With MTHFR Mutations
- Limitations of MTHFR Testing
- Key Research Papers
- Featured Videos
What MTHFR Gene Testing Measures
MTHFR gene testing identifies specific inherited variants in the methylenetetrahydrofolate reductase (MTHFR) gene, located on chromosome 1. The MTHFR enzyme is essential for processing folate (vitamin B9) and converting homocysteine into methionine, a process at the heart of the methylation cycle. Methylation is a fundamental biochemical reaction that occurs billions of times per second throughout the body, influencing DNA repair, gene expression, neurotransmitter production, detoxification, and immune regulation.
The test uses a blood sample or cheek swab to analyze the DNA sequence of the MTHFR gene and identify whether a person carries one or both of the two clinically significant variants: C677T and A1298C. These single-nucleotide polymorphisms (SNPs) reduce enzyme activity, meaning the body processes folate less efficiently and may accumulate homocysteine at higher-than-normal levels.
MTHFR mutations are among the most common genetic variants in humans, with heterozygous C677T occurring in approximately 40% of the general population and homozygous C677T in 10-15%. Testing is ordered when a clinician suspects elevated homocysteine, recurrent pregnancy loss, cardiovascular risk factors, or psychiatric conditions may have a genetic methylation component.
Why MTHFR Testing Is Ordered
Clinicians order MTHFR gene testing for a range of clinical indications where impaired folate metabolism or elevated homocysteine may be contributing to a patient's health problems. Common reasons include:
- Elevated homocysteine levels: Homocysteine is a cardiovascular and neurological toxin. When homocysteine is elevated on a blood test, MTHFR mutation testing helps explain why and guides supplementation with methylated B vitamins.
- Recurrent pregnancy loss: MTHFR mutations, particularly compound heterozygous or homozygous variants, are associated with increased risk of neural tube defects, placental abruption, and miscarriage due to impaired folate metabolism during embryonic development.
- Family history of cardiovascular disease or stroke: Hyperhomocysteinemia from MTHFR mutations is a recognized independent risk factor for atherosclerosis, thrombosis, and stroke.
- Psychiatric conditions: Depression, anxiety, schizophrenia, bipolar disorder, and ADHD have been linked to impaired methylation capacity in some individuals, as methylation is required for serotonin, dopamine, and norepinephrine synthesis.
- Fatigue and brain fog unresponsive to standard treatment: Methylation dysfunction can cause low energy, cognitive difficulties, and mood disturbances, particularly when standard B12 and folate supplementation (using non-methylated forms) fails to help.
- Neural tube defect in a previous pregnancy: Parents who have had a child with spina bifida or anencephaly are frequently tested for MTHFR variants to guide folate supplementation in future pregnancies.
How the Test Is Performed
MTHFR genotyping is a straightforward genetic test requiring either a venous blood draw or a buccal (cheek) swab. No fasting is required. The sample is sent to a molecular genetics laboratory where DNA is extracted and the MTHFR gene region is analyzed using polymerase chain reaction (PCR) followed by allele-specific detection methods such as restriction fragment length polymorphism (RFLP) or real-time PCR.
Results typically return within 3-10 business days. Because MTHFR variants are stable genetic traits that do not change over a person's lifetime, the test only needs to be done once. The result identifies the patient's genotype at both the C677T and A1298C positions, and reports whether they are homozygous (two copies of the variant), heterozygous (one copy), or wild-type (no variant) at each position.
MTHFR testing can also be included in broader genetic panels such as direct-to-consumer genomic tests (23andMe, AncestryDNA), though clinical laboratory testing is more accurate and appropriate for medical decision-making. Insurance coverage varies widely; many plans cover the test when ordered for specific indications such as recurrent pregnancy loss or confirmed hyperhomocysteinemia.
MTHFR Variants: C677T and A1298C
The two clinically significant MTHFR variants are:
C677T (rs1801133): This is the most studied MTHFR variant. The cytosine (C) at nucleotide position 677 is replaced by thymine (T), resulting in an amino acid change from alanine to valine in the MTHFR enzyme protein. This structural change makes the enzyme thermolabile (heat-sensitive) and reduces its activity:
- Heterozygous C677T (one copy): MTHFR enzyme activity is reduced to approximately 65% of normal. Mild impact; homocysteine may be slightly elevated, particularly when folate intake is inadequate.
- Homozygous C677T (two copies, also written TT): Enzyme activity reduced to approximately 30-35% of normal. More significant impact on folate processing and homocysteine levels. Associated with greater cardiovascular and neurological risk.
A1298C (rs1801131): The adenine (A) at position 1298 is replaced by cytosine (C). This variant has a lesser effect on enzyme thermolability but still reduces MTHFR activity:
- Heterozygous A1298C: Modest reduction in enzyme function. Clinically, isolated heterozygous A1298C is rarely associated with elevated homocysteine on its own.
- Homozygous A1298C (two copies): More significant enzyme reduction, though generally less severe than homozygous C677T.
Compound Heterozygous (one C677T + one A1298C): Carrying one copy of each variant is clinically significant and can reduce MTHFR enzyme activity to a degree similar to homozygous C677T. This combination is particularly associated with elevated homocysteine, recurrent pregnancy loss, and cardiovascular risk.
Reference Ranges and Result Interpretation
MTHFR gene testing reports genotype results rather than numeric values. Interpretation depends on which variant is detected and whether one or two copies are present:
- Wild-type (Normal): No variants detected at C677T or A1298C. Normal MTHFR enzyme function expected. Standard dietary folate intake is typically sufficient.
- Heterozygous C677T: One variant copy. Mild enzyme impairment. Ensure adequate folate intake; consider methylfolate supplementation, especially in pregnancy.
- Homozygous C677T (TT): Two copies of the variant. Significant enzyme impairment. Methylated B vitamins (methylfolate, methylcobalamin) are strongly preferred over synthetic folic acid. Monitor homocysteine levels.
- Heterozygous A1298C: One variant copy. Minimal clinical significance in isolation. Standard dietary measures usually sufficient.
- Homozygous A1298C: Two copies. Moderate enzyme impairment. Methylated supplementation advisable.
- Compound Heterozygous (C677T + A1298C): One copy of each variant. Treat similarly to homozygous C677T; use methylated B vitamins and monitor homocysteine.
Genotype results must always be interpreted in clinical context. A positive MTHFR variant does not by itself constitute a diagnosis of disease -- it is a risk modifier that should prompt assessment of homocysteine levels, folate status, B12 status, and lifestyle factors.
Conditions Associated With MTHFR Mutations
MTHFR variants have been associated with a broad range of conditions in the medical literature, though it is important to distinguish between strong, well-replicated associations and weaker or more controversial ones:
Well-established associations:
- Hyperhomocysteinemia: Elevated homocysteine is the most direct and consistently replicated consequence of significant MTHFR impairment, particularly homozygous C677T with inadequate folate intake.
- Neural tube defects: MTHFR C677T homozygosity in either the mother or fetus increases risk of spina bifida and anencephaly. This finding drove universal recommendations for folic acid supplementation in pregnancy.
- Recurrent pregnancy loss: Meta-analyses have found elevated risk in women with MTHFR mutations, though the association is modest and other thrombophilic factors are often co-present.
- Cardiovascular disease and stroke: Hyperhomocysteinemia from MTHFR mutations is associated with endothelial dysfunction, platelet activation, and atherosclerosis.
Probable associations (ongoing research):
- Depression and psychiatric disorders: Methylation is required for monoamine neurotransmitter synthesis. Impaired methylation has been linked to treatment-resistant depression; methylfolate is FDA-approved as an adjunct to antidepressant therapy.
- Migraine with aura: Several studies have found C677T homozygosity associated with migraine, possibly through elevated homocysteine or nitric oxide pathway effects.
- Colorectal cancer: Complex relationship -- low folate intake with C677T homozygosity appears to increase risk, while adequate folate may be protective.
- Autism spectrum disorder: Some studies suggest associations with folate pathway variants, though findings remain inconsistent.
The Methylation Cycle Explained
Methylation is the process of adding a methyl group (one carbon atom bonded to three hydrogen atoms, -CH3) to a molecule. This simple chemical addition activates or deactivates genes, produces neurotransmitters, detoxifies environmental chemicals, builds cell membranes, and regulates hundreds of other biological processes.
The methylation cycle involves a series of enzymatic reactions that recycle a single methyl group through four main compounds:
- Methionine: An essential amino acid that becomes the universal methyl donor S-adenosylmethionine (SAMe) when combined with ATP. SAMe donates its methyl group to over 200 different reactions throughout the body.
- SAMe (S-adenosylmethionine): After donating its methyl group, SAMe becomes S-adenosylhomocysteine (SAH), then homocysteine.
- Homocysteine: At this critical junction, homocysteine can be remethylated back to methionine (via the MTHFR enzyme using methylfolate and methylcobalamin) or irreversibly converted to cysteine via the transsulfuration pathway (requiring vitamin B6). The MTHFR enzyme controls the remethylation route.
- Tetrahydrofolate (THF): After MTHFR converts 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate (5-MTHF, or methylfolate), this active folate donates its methyl group to remethylate homocysteine back to methionine, with vitamin B12 (as methylcobalamin) as the essential cofactor.
When MTHFR is impaired, the production of methylfolate is reduced, the remethylation of homocysteine slows, SAMe levels may fall, and the entire methylation cycle operates at reduced capacity. The downstream effects touch virtually every system in the body that depends on methylation for proper function.
The Homocysteine Connection
Homocysteine is a sulfur-containing amino acid that serves as a critical junction in the methylation cycle. In normal physiology, homocysteine is rapidly recycled back to methionine through remethylation (dependent on MTHFR, methylfolate, and methylcobalamin) or converted to cysteine through transsulfuration (dependent on vitamin B6). When these pathways are impaired -- whether through MTHFR mutations, B vitamin deficiencies, poor diet, or aging -- homocysteine accumulates in the blood.
Elevated homocysteine (hyperhomocysteinemia) causes measurable harm to the cardiovascular and nervous systems through several mechanisms:
- Endothelial injury: Homocysteine directly damages the endothelial cells lining blood vessels, promoting oxidative stress, reducing nitric oxide availability, and initiating the inflammatory cascade that leads to atherosclerosis.
- Thrombosis promotion: Homocysteine enhances platelet aggregation, activates clotting factors, and suppresses anticoagulant proteins, creating a prothrombotic state that raises risk of heart attack, stroke, and venous thromboembolism.
- Neurotoxicity: At high concentrations, homocysteine is directly neurotoxic, stimulating NMDA receptors, inducing oxidative stress in neurons, and contributing to cognitive decline and dementia.
The functional optimal homocysteine level is below 7 µmol/L, though many labs list conventional normal as below 15 µmol/L. Levels above 10 µmol/L are associated with progressively increasing cardiovascular and cognitive risk. In patients with MTHFR mutations, homocysteine testing should be performed alongside MTHFR genotyping to assess actual functional impact.
How to Improve Outcomes With MTHFR Mutations
The practical clinical implication of MTHFR mutations is not that a person is inevitably destined for disease, but that they need to support their methylation pathway more deliberately. The following strategies are evidence-based and commonly recommended by functional medicine practitioners:
Use Methylated B Vitamins
The single most important intervention for people with MTHFR mutations is replacing synthetic folic acid and cyanocobalamin with their bioactive, methylated forms:
- 5-MTHF (methylfolate): This is the active form of folate that bypasses the MTHFR enzyme entirely. Brands include Metafolin and Quatrefolic. Typical doses range from 400 mcg to 5 mg daily depending on genotype and clinical context. People with homozygous C677T or compound heterozygous variants generally need higher doses.
- Methylcobalamin: The active, methylated form of vitamin B12 that serves as the cofactor for the remethylation of homocysteine. Preferred over cyanocobalamin, particularly for individuals with neurological symptoms.
- Pyridoxal-5-phosphate (P5P): The active form of vitamin B6 supports the transsulfuration pathway, providing an alternative route for homocysteine clearance.
Avoid Unmetabolized Folic Acid
Synthetic folic acid found in fortified foods and most conventional supplements requires conversion by the MTHFR enzyme to become usable. In people with impaired MTHFR function, large doses of synthetic folic acid can accumulate as unmetabolized folic acid (UMFA) in the blood, which may paradoxically inhibit folate receptors and worsen functional folate deficiency. Reading supplement and food labels to identify folic acid and replacing it with methylfolate is an important practical step.
Optimize Diet
- Increase natural food folate: Dark leafy greens (spinach, arugula, romaine), asparagus, lentils, chickpeas, avocado, and beets are rich in natural food folate, which is better absorbed than synthetic folic acid by those with MTHFR mutations.
- Prioritize protein quality: Methionine is the entry point of the methylation cycle. Adequate intake of methionine from eggs, poultry, fish, and meat supports the cycle upstream of MTHFR.
- Riboflavin (B2): Riboflavin is a cofactor that stabilizes the MTHFR enzyme. Studies have shown that riboflavin supplementation can improve homocysteine levels in C677T homozygotes, partially compensating for reduced enzyme activity. Doses of 1.6-5 mg/day have been used in research.
Lifestyle Factors
- Limit alcohol: Alcohol impairs folate absorption and increases folate excretion, worsening functional folate deficiency in people with MTHFR mutations.
- Reduce methionine excess: Very high meat intake without adequate folate can overwhelm the remethylation pathway and raise homocysteine.
- Address gut health: Intestinal absorption of folate and B12 depends on a healthy gut lining. Celiac disease, inflammatory bowel disease, or H. pylori infection can reduce B vitamin absorption and worsen functional methylation deficiency.
Limitations of MTHFR Testing
Despite widespread clinical use, MTHFR gene testing has important limitations that require thoughtful interpretation:
- Common variants do not equal disease: MTHFR variants are extremely common in the general population. The C677T heterozygous variant is present in roughly 40% of people, yet the vast majority live without significant health consequences when their diet provides adequate folate. Having a variant is a risk modifier, not a diagnosis.
- The test does not measure actual enzyme activity: Genotyping identifies which variant a person carries but does not directly measure how well their MTHFR enzyme is actually functioning in their specific physiological context. Nutritional status, riboflavin levels, and other genetic modifiers all affect actual enzyme output.
- Homocysteine is a better functional marker: Measuring serum homocysteine gives a direct readout of whether the methylation pathway is actually impaired. Many experts argue that in clinical practice, homocysteine testing is more actionable than MTHFR genotyping, since homocysteine can be elevated for reasons other than MTHFR (B12 deficiency, renal dysfunction, hypothyroidism), and can be normal despite MTHFR mutations when diet is adequate.
- Many associated conditions have weak evidence: While associations between MTHFR and various psychiatric, autoimmune, and chronic conditions are circulating widely online and in integrative medicine, many of these associations are based on small studies, lack replication, or have been refuted in larger meta-analyses. Patients should be counseled to be critical of overly broad claims.
- Insurance coverage is inconsistent: Many insurers will not cover MTHFR testing in the absence of elevated homocysteine or specific obstetric indications, and clinicians ordering it "routinely" may find it rejected as not medically necessary.
Key Research Papers
The following PubMed literature searches cover the evidence base for MTHFR gene mutation testing and its clinical applications.
- MTHFR C677T, homocysteine, and cardiovascular disease — PubMed
- MTHFR mutations, neural tube defects, and folate — PubMed
- MTHFR and recurrent pregnancy loss — PubMed meta-analysis
- Methylfolate for treatment-resistant depression — PubMed
- MTHFR A1298C compound heterozygous clinical significance — PubMed
- Riboflavin and MTHFR TT genotype homocysteine — PubMed
- Unmetabolized folic acid and MTHFR — PubMed
- MTHFR, methylation cycle, and SAMe — PubMed
- Homocysteine, stroke, and cognitive decline — PubMed
- MTHFR testing clinical guidelines and utility — PubMed
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — MTHFR Gene, Folic Acid, and Cancer
Connections
- All Lab Tests
- Homocysteine Test
- Vitamin B12 Test
- Inflammatory Markers
- Complete Blood Count (CBC)
- Folate (Vitamin B9)
- Vitamin B12
- Vitamin B6
- Riboflavin (Vitamin B2)
- Heart Disease
- Depression
- Alzheimer's Disease
- Lipid Panel