Rosemary for Digestive and Liver Function
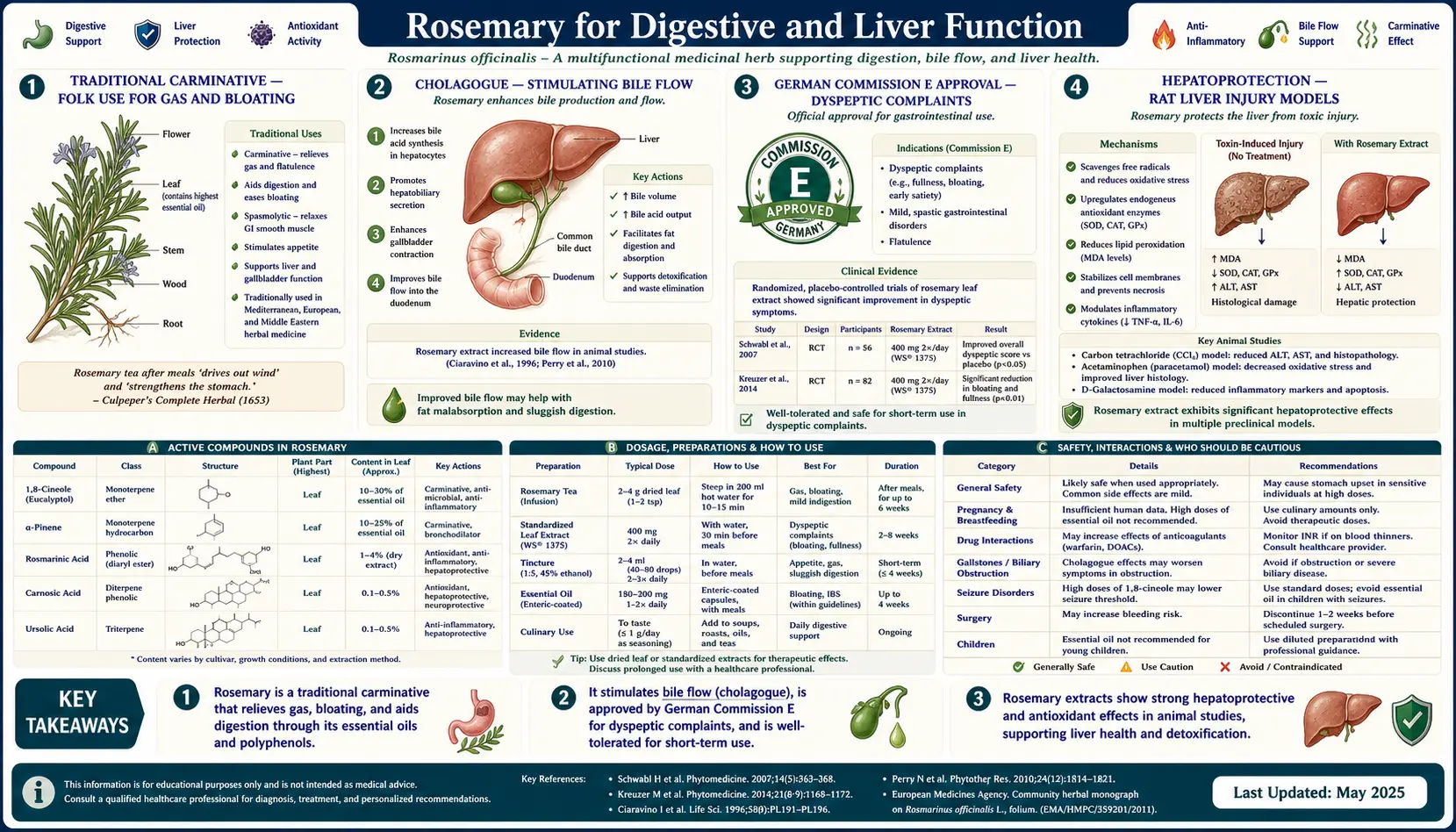
Rosemary's traditional use as a digestive remedy is older than the Renaissance herbals and is one of the few herb-and-spice applications formally codified by the German Commission E, the historical regulatory authority on European phytomedicine. Commission E approved rosemary leaf for "dyspeptic complaints" — gas, bloating, mild gastrointestinal cramping, and the sluggish digestion that follows a heavy meal. The traditional mechanism categories are carminative (relieving gas, mediated by the volatile monoterpenes 1,8-cineole and alpha-pinene relaxing intestinal smooth muscle) and cholagogue (stimulating bile flow from the gallbladder, mediated by the bitter principles and phenolic diterpenes acting on the duodenal mucosa). A separate and increasingly well-documented effect is hepatoprotection — rat models of liver injury induced by carbon tetrachloride, acetaminophen overdose, and chronic ethanol consistently show reduced hepatocellular damage when carnosic acid, carnosol, or whole rosemary extract is administered before or during the toxin exposure. The mechanism is the same Nrf2 / antioxidant chemistry covered on the antioxidant page, applied to the specific oxidative-stress vulnerability of the liver. This deep-dive walks through the traditional uses, the Commission E approval, the hepatoprotective animal evidence, the COX-inhibition contribution to anti-inflammatory action in the gut, and the important cautions around essential oil dosing.
Table of Contents
- Traditional Carminative — the Folk Use for Gas and Bloating
- Cholagogue — Stimulating Bile Flow
- German Commission E Approval — Dyspeptic Complaints
- Hepatoprotection — the Rat Liver Injury Models
- Carbon Tetrachloride (CCl4) Hepatotoxicity
- Acetaminophen (Paracetamol) Hepatotoxicity
- Chronic Ethanol Liver Injury
- COX-1 and COX-2 Inhibition — Anti-Inflammatory Mechanism
- Effects on the Gut Microbiome
- NAFLD and Fatty Liver Disease — Mechanistic Relevance
- Practical Protocols for Digestive Use
- Essential Oil Cautions — the Oral Hazard
- Key Research Papers
- Connections
- Featured Videos
Traditional Carminative — the Folk Use for Gas and Bloating
A carminative in traditional Western herbalism is an herb that relieves intestinal gas, bloating, and the mild crampy abdominal discomfort that often accompanies heavy or rich meals. The classical carminatives include fennel, anise, caraway, dill, peppermint, ginger, and rosemary — all of them rich in volatile aromatic compounds that have direct relaxing effects on intestinal smooth muscle.
The traditional use of rosemary as a post-meal digestive aid is documented across the Mediterranean culinary tradition. Roasted meat with rosemary (still a defining preparation of Italian and Provencal cooking) is not merely a flavor pairing — the herb actively helps the digestion of the fat-rich meal it garnishes. Sprigs of fresh rosemary floated in olive oil or in red wine vinegar produce digestive tonics that have been part of European folk medicine for centuries.
The pharmacological basis of the carminative effect is well-characterized:
- 1,8-cineole and alpha-pinene in the volatile fraction relax intestinal smooth muscle through a mechanism that includes calcium-channel inhibition and direct effects on muscarinic acetylcholine receptors
- Borneol and camphor have similar antispasmodic activity
- The relaxation of smooth muscle helps expel trapped intestinal gas and reduces the crampy "spasm" that contributes to functional dyspepsia
- The aromatic volatiles also stimulate salivary and gastric secretion, supporting the upstream stages of digestion
A practical demonstration: a cup of rosemary tea taken after a rich meal often produces noticeable belching and gas release within 10-20 minutes, accompanied by relief of post-prandial fullness. The same effect is what makes a digestif of grappa or amaro (often containing carminative herbs including rosemary) traditional in Italian cuisine.
Cholagogue — Stimulating Bile Flow
A cholagogue is an herb that stimulates the contraction of the gallbladder and the release of stored bile into the duodenum, accelerating the digestion of dietary fats. Bile contains bile salts (which emulsify dietary lipids and form mixed micelles with cholesterol and fat-soluble vitamins), phospholipids, cholesterol, and bilirubin. Inadequate bile flow contributes to fat maldigestion (steatorrhea, oily stools), fat-soluble vitamin malabsorption, and the bloating and discomfort associated with heavy fatty meals.
Cholagogue action by rosemary is mediated primarily by the bitter principles — the phenolic diterpenes (carnosic acid, carnosol) and the small amount of bitter components in the leaf. When these compounds contact the bitter taste receptors on the tongue and the small intestinal mucosa, they trigger a vagal reflex that stimulates gallbladder contraction and bile release. This is the same mechanism behind the European tradition of taking a bitter digestif before or after a meal — the bitter taste itself, even before absorption, activates the digestive cascade.
Documented cholagogue effects of rosemary in animal and limited human studies:
- Increased bile flow rate measured in rat bile-duct cannulation studies after rosemary extract administration
- Increased gallbladder contraction velocity measured by ultrasound in small human studies of bitter herb cocktails containing rosemary
- Reduced post-prandial epigastric fullness after fatty meals in patients with functional dyspepsia receiving rosemary leaf preparations
The clinical relevance is concentrated in patients with mild functional dyspepsia, post-cholecystectomy syndrome (after gallbladder removal, when bile delivery becomes continuous-low-flow rather than meal-stimulated bolus), and the slowed digestion of aging or chronic illness. For patients with documented bile flow obstruction (gallstones, biliary stricture), cholagogue herbs are generally avoided because increasing bile flow against a partial obstruction can precipitate biliary colic.
German Commission E Approval — Dyspeptic Complaints
The German Commission E was a multidisciplinary regulatory body established by the German Federal Institute for Drugs and Medical Devices in 1978 to evaluate the safety and efficacy of botanical medicines used in Germany. From 1978 to 1994 Commission E reviewed approximately 380 herbs and published monographs categorizing each as Approved (safety and efficacy documented), Unapproved (insufficient evidence or known safety concerns), or Neutral. The Commission E monographs remain influential in the European Medicines Agency's current herbal monograph system and in international phytomedicine practice.
Commission E approved rosemary leaf for the following internal uses:
- Dyspeptic complaints — gas, bloating, mild epigastric discomfort, sluggish digestion
- Average daily dose: 4-6 g of dried leaf, equivalent to a strong infusion two to three times daily
- Contraindications: pregnancy (medicinal doses)
And approved rosemary oil for the following uses (external only):
- Supportive therapy for rheumatic complaints — topical application as part of liniments and topical preparations
- Circulatory problems — external use to improve peripheral circulation
The European Medicines Agency Herbal Monograph for Rosmarini folium (rosemary leaf) and for Rosmarini aetheroleum (rosemary essential oil) reaffirmed and updated these indications in 2010, classifying rosemary leaf as a "traditional herbal medicinal product" for the symptomatic relief of dyspepsia and mild spasmodic disorders of the gastrointestinal tract. The EMA monographs are the current regulatory standard in the EU for rosemary preparations.
Importantly, neither Commission E nor the EMA approves oral consumption of rosemary essential oil. The essential oil is approved only for external use (topical or aromatherapy). The dried leaf and tea preparations are the approved internal forms. See the Essential Oil Cautions section below for the safety rationale.
Hepatoprotection — the Rat Liver Injury Models
A separate and increasingly well-documented effect of rosemary is hepatoprotection — protection of the liver against drug- and toxin-induced injury. The evidence base is primarily in rat models because the experimental induction of severe liver injury is unethical in humans, but the mechanistic story translates plausibly through shared mammalian biochemistry.
The standard rat liver injury models in which rosemary has been tested:
- Carbon tetrachloride (CCl4) — the classic experimental hepatotoxin, metabolized by CYP2E1 to trichloromethyl radicals that drive massive lipid peroxidation and centrilobular hepatocyte necrosis
- Acetaminophen (paracetamol) — overdose model relevant to one of the most common causes of acute liver failure in humans; toxicity mediated by the reactive metabolite NAPQI
- Chronic ethanol — model of alcoholic fatty liver disease and progression to steatohepatitis
- Thioacetamide — alternative hepatotoxin producing centrilobular necrosis
- Galactosamine — model resembling viral hepatitis in its periportal necrosis pattern
- Cadmium and other heavy metals — cumulative hepatotoxin models
Across all these models, pre-treatment or co-treatment with rosemary extract, carnosic acid, carnosol, or rosmarinic acid consistently reduces:
- Serum AST and ALT (transaminases) elevations — the standard clinical markers of hepatocellular injury
- Hepatocellular necrosis on histology
- Hepatic lipid peroxidation markers (malondialdehyde, 4-hydroxynonenal)
- Hepatic glutathione depletion (the toxin-driven exhaustion of the liver's primary antioxidant defense)
- Inflammatory cytokine elevations (TNF-alpha, IL-6, IL-1beta)
The underlying mechanism in every case is the Nrf2-driven upregulation of glutathione synthesis, superoxide dismutase, catalase, and heme oxygenase-1, which collectively raise the liver's antioxidant capacity above what the toxin can overwhelm.
Carbon Tetrachloride (CCl4) Hepatotoxicity
Carbon tetrachloride is the historical workhorse of experimental hepatotoxicology. It is metabolized in hepatocytes by the cytochrome P450 isoform CYP2E1 to the highly reactive trichloromethyl free radical, which initiates massive lipid peroxidation of hepatocyte membranes, particularly the endoplasmic reticulum and mitochondrial membranes. The result is acute centrilobular hepatocyte necrosis (because CYP2E1 is concentrated in zone 3 hepatocytes near the central vein), elevated transaminases, and at higher doses fulminant hepatic necrosis.
Multiple rosemary CCl4 studies have demonstrated:
- Pre-treatment with rosemary leaf extract (typically 100-400 mg/kg/day for 7-14 days before CCl4 challenge) reduces post-CCl4 transaminase elevation by 50-80%
- Pre-treatment reduces histologic necrosis score and preserves more zone 3 hepatocytes
- The protective effect is dose-dependent and saturates at moderate doses
- Co-administration of just carnosic acid or carnosol (the isolated phenolic diterpenes) produces effects comparable to whole extract, confirming these as the principal active compounds
- The protection is mechanistically attributable to Nrf2 activation, glutathione preservation, and direct interception of the trichloromethyl free radical by the lipid-phase antioxidant activity of the diterpenes
The CCl4 model is most relevant clinically as a proof-of-mechanism for general lipid-peroxidation-driven hepatocellular injury. The same mechanism is relevant to many other forms of hepatotoxicity including acetaminophen overdose, severe ischemic injury (e.g., post-liver-transplant reperfusion injury), and toxic mushroom poisoning.
Acetaminophen (Paracetamol) Hepatotoxicity
Acetaminophen overdose is the leading cause of acute liver failure requiring transplantation in the United States and the United Kingdom. The toxicity mechanism is well-understood:
- At therapeutic doses, most acetaminophen is glucuronidated or sulfated to inactive metabolites and renally excreted
- A small fraction is oxidized by CYP2E1 to the reactive intermediate N-acetyl-p-benzoquinone imine (NAPQI)
- NAPQI is normally rapidly conjugated and detoxified by hepatocellular glutathione
- At overdose, the glutathione pool is depleted, NAPQI accumulates and covalently binds hepatocyte proteins, producing oxidative stress and centrilobular necrosis
- The clinical antidote, N-acetylcysteine (NAC), provides cysteine for glutathione resynthesis and directly conjugates remaining NAPQI
Rosemary extract administered before or during experimental acetaminophen overdose in rats and mice consistently reduces transaminase elevations, hepatocyte necrosis, and mortality. The mechanism overlaps with the NAC mechanism — rosemary's Nrf2 activation upregulates the glutathione synthesis enzymes, increasing the rate at which depleted glutathione pools can be restored. This is a different mechanism than NAC's direct cysteine supplementation, but achieves a complementary endpoint of maintaining or restoring hepatocellular glutathione capacity.
The translational caveat: in clinical acetaminophen overdose, intravenous NAC remains the standard of care, started as soon as possible within the 8-hour optimal window. Rosemary extract is not a substitute for NAC and should not be presented as such. The conceptual interest is in dietary patterns that maintain robust baseline hepatic antioxidant defenses, potentially providing some protective margin against accidental supratherapeutic acetaminophen exposure and against the cumulative low-grade hepatotoxic stress of polypharmacy.
Chronic Ethanol Liver Injury
Chronic ethanol consumption produces a progression from alcoholic fatty liver (hepatic steatosis) through steatohepatitis to fibrosis and cirrhosis. The pathogenesis involves direct hepatotoxic effects of ethanol and its metabolite acetaldehyde, induction of CYP2E1 (which generates reactive oxygen species during ethanol oxidation), depletion of hepatocellular glutathione, mitochondrial dysfunction, and chronic inflammatory activation of Kupffer cells.
Rat models of chronic ethanol-induced liver injury treated with rosemary extract have shown:
- Reduced hepatic triglyceride accumulation (less fatty liver)
- Reduced transaminase elevation
- Preserved hepatic glutathione pools
- Reduced inflammatory infiltrate on histology
- Reduced fibrosis progression in longer-duration studies
The translational implications are interesting but should not be overstated. The protective effects in rat models do not constitute permission to consume excessive alcohol — the magnitude of human alcohol consumption that produces clinical alcoholic liver disease is far above what any dietary or supplemental antioxidant could realistically counterbalance. For patients with diagnosed alcoholic liver disease, the primary intervention is reduction or cessation of alcohol consumption, and rosemary or any other dietary antioxidant should be considered an adjunct to (not a replacement for) the primary treatment.
For patients with non-alcoholic fatty liver disease (NAFLD), the rosemary mechanism is more directly relevant — see the NAFLD section below.
COX-1 and COX-2 Inhibition — Anti-Inflammatory Mechanism
A complementary anti-inflammatory mechanism contributing to rosemary's digestive and broader effects is inhibition of the cyclooxygenase enzymes COX-1 and COX-2, which convert arachidonic acid to prostaglandins and thromboxanes. COX-1 is constitutively expressed and produces the "housekeeping" prostaglandins that maintain gastric mucosal integrity, platelet aggregation, and renal blood flow. COX-2 is induced at sites of tissue injury and inflammation, producing the prostaglandins that drive pain, fever, and inflammation.
The non-steroidal anti-inflammatory drug (NSAID) class works primarily by inhibiting COX enzymes. Older NSAIDs (aspirin, ibuprofen, naproxen) inhibit both COX-1 and COX-2; the gastric ulceration side effect is attributable to the COX-1 inhibition that compromises gastric mucosal prostaglandin production. The selective COX-2 inhibitors (celecoxib) were developed to maintain anti-inflammatory efficacy while sparing gastric mucosal prostaglandins.
Rosemary extracts and isolated carnosol and rosmarinic acid have been shown to inhibit both COX-1 and COX-2 in vitro, with somewhat greater selectivity for COX-2 in some preparations. The clinical significance:
- Contributes to the anti-inflammatory and modest analgesic effects of rosemary preparations
- Likely contributes to the digestive benefit by reducing the inflammatory component of functional dyspepsia and IBS
- Theoretical platelet aggregation effect (COX-1 inhibition reduces thromboxane A2 production) — relevant to the cautions for patients on antiplatelet drugs
- Contributes to the rationale for topical rosemary preparations in rheumatic complaints (the Commission E external-use indication)
The potency of rosemary as a COX inhibitor is far lower than pharmaceutical NSAIDs — routine culinary use is unlikely to produce clinically significant effects equivalent to ibuprofen. High-dose extract use approaches a magnitude that could theoretically produce additive effects with low-dose aspirin or other antiplatelet drugs.
Effects on the Gut Microbiome
Rosemary essential oil, rosemary extracts, and isolated carnosic acid have direct antimicrobial activity against a range of bacterial and fungal species, including several human gut pathogens. This is one of the historical reasons rosemary was burned as a fumigant in medieval European sickrooms and used as a preservative for stored meat in pre-refrigeration cuisine.
Documented in vitro antimicrobial activity:
- Gram-positive bacteria — Staphylococcus aureus (including MRSA strains), Bacillus subtilis, Listeria monocytogenes
- Gram-negative bacteria — Escherichia coli, Salmonella, Helicobacter pylori
- Fungi — Candida albicans, Aspergillus species
- Biofilm disruption — rosemary essential oil and carvacrol-rich essential oils disrupt established bacterial biofilms in vitro
The translational significance for human gut health is moderate. The doses of rosemary consumed in cooking or in moderate tea use are unlikely to produce significant antimicrobial effects in the intact gut lumen. However, several clinical implications follow from the in vitro evidence:
- Rosemary's historical role as a food preservative was partly antimicrobial — reducing the bacterial spoilage of stored meat
- Anti-Helicobacter pylori activity has been studied as an adjunct in eradication regimens, although triple-therapy antibiotics remain the standard of care
- For patients with small intestinal bacterial overgrowth (SIBO), the combination of rosemary with other antimicrobial herbs (oregano, thyme, berberine) may contribute to herbal antimicrobial protocols, although evidence for the specific herbal contribution versus pharmaceutical antibiotics is limited
- Routine culinary use of rosemary is unlikely to produce gut microbiome dysbiosis — the antimicrobial effects at dietary doses appear to be modest and largely confined to opportunistic pathogen suppression rather than commensal disruption
NAFLD and Fatty Liver Disease — Mechanistic Relevance
Non-alcoholic fatty liver disease (NAFLD) is now the most common chronic liver disease in the developed world, affecting an estimated 25-40% of adults. The pathogenesis involves hepatic insulin resistance, accumulation of triglycerides in hepatocytes, secondary oxidative stress and inflammation that can progress to non-alcoholic steatohepatitis (NASH), and eventually fibrosis and cirrhosis in a subset.
The mechanistic connections between rosemary's biology and NAFLD pathophysiology:
- PPAR-gamma activation by carnosic acid — improves hepatic insulin sensitivity, reducing the primary driver of triglyceride accumulation
- AMPK activation by carnosic acid and rosmarinic acid — promotes fatty acid oxidation and inhibits fatty acid synthesis, reducing hepatic triglyceride accumulation
- Nrf2 activation — counters the secondary oxidative stress that drives the progression from simple steatosis to steatohepatitis
- NF-kappaB inhibition — suppresses the inflammatory activation of Kupffer cells that drives steatohepatitis
- Effects on the gut microbiome and gut-liver axis — reduced bacterial translocation and LPS delivery to the portal venous system, reducing inflammatory drive on the liver
Several small human trials of rosemary or rosemary-extract supplementation in NAFLD patients have shown modest improvements in hepatic steatosis (measured by ultrasound or controlled attenuation parameter on FibroScan) and transaminase reductions. These trials have generally been small and have not been replicated in large multi-center designs. The strongest current evidence base for NAFLD lifestyle intervention remains weight loss (5-10% body weight reduction reliably reverses steatosis in most patients) and the Mediterranean diet pattern (which includes regular rosemary use as one of many beneficial elements).
For patients with diagnosed NAFLD, regular culinary use of rosemary and other Mediterranean herbs is a sensible component of a broader nutritional approach. Supplemental rosemary extract is a reasonable adjunct with modest evidence but should not replace weight loss, dietary improvement, and management of associated metabolic syndrome components.
Practical Protocols for Digestive Use
For someone wanting to use rosemary practically for digestive benefit:
- Rosemary tea — the standard approach. Steep 1-2 teaspoons of dried rosemary leaf (or 1 tablespoon fresh chopped leaf) in 8-10 oz of just-boiled water for 8-10 minutes, covered to retain the volatile fraction. Drink one cup 15-30 minutes after a heavy meal. Tolerable to take 2-3 cups daily.
- Culinary use — routine cooking with dried or fresh rosemary on fatty meals (roast meats, oily fish, hearty stews) delivers a modest but real digestive benefit. Add early for full flavor development, but be aware that the volatile carminative fraction degrades with prolonged heat — for maximum digestive effect, finish a dish with a small amount of fresh herb added near the end of cooking.
- Bitter tincture — commercial digestive bitter formulas often contain rosemary along with gentian, dandelion, fennel, and other carminatives. 1-2 mL in a small amount of water 15 minutes before a meal triggers the upper-digestive cascade through the bitter taste receptor pathway.
- Standardized leaf extract capsules — 200-400 mg/day of standardized rosemary leaf extract is in the range used in clinical trials for general antioxidant and metabolic effects. Most users do not find capsules necessary if they routinely consume rosemary in cooking and tea.
- Avoid the essential oil orally — see the next section. Rosemary essential oil is not a safe replacement for rosemary leaf for oral digestive use.
Combination with other carminative herbs (peppermint, fennel, chamomile, ginger, lemon balm) is traditional and pharmacologically sensible — the carminative effects of different aromatic herbs often appear additive without dosage-dependent toxicity. A simple after-dinner blend of equal parts rosemary, peppermint, and fennel makes a reliable digestive infusion.
Essential Oil Cautions — the Oral Hazard
The single most important safety point about rosemary essential oil is that it is not safe for oral consumption at meaningful doses without explicit professional guidance from a clinical aromatherapist or qualified herbalist. The essential oil is far more concentrated than the dried leaf or any culinary preparation, and the volatile monoterpenes (camphor, 1,8-cineole) that produce the cognitive effects when inhaled can produce serious adverse effects when swallowed.
Documented toxicity from oral rosemary essential oil ingestion:
- Acute gastrointestinal toxicity — severe nausea, vomiting, gastrointestinal irritation, mucosal damage
- Hepatotoxicity — paradoxically, the same compounds that are hepatoprotective at low dietary doses can be hepatotoxic at concentrated essential oil doses
- Renal toxicity — nephrotoxic at supratherapeutic doses
- CNS toxicity — CNS depression, seizures (camphor is a well-known seizure-precipitating compound at high doses)
- Pregnancy harm — oral essential oil doses are abortifacient in animal models
The fundamental safety principle: the dose makes the poison. A teaspoon of dried rosemary leaf in tea is safe and beneficial. A teaspoon of pure rosemary essential oil is a medical emergency. The 100-200x concentration difference between dried herb and essential oil is the critical safety boundary.
Approved internal use of rosemary remains the dried leaf, the leaf tea, the standardized leaf extract (not essential oil), and modest culinary use. Approved external use of the essential oil includes aromatherapy (the inhalation cognitive use covered on the cognitive page) and topical use diluted in carrier oil (the hair-loss use covered on the hair loss page).
For accidental essential oil ingestion: contact Poison Control immediately (1-800-222-1222 in the US). Do not induce vomiting (caustic essential oils may produce additional esophageal damage on emesis). Provide supportive care including airway management, hydration, and treatment of specific toxicities.
Key Research Papers
- Hoefler C et al. (1987). Choleretic and spasmolytic effects of a rosemary extract on rat liver and isolated guinea pig and rabbit ileum. Planta Medica. — PubMed
- Sotelo-Felix JI et al. (2002). Evaluation of the effectiveness of Rosmarinus officinalis (Lamiaceae) in the alleviation of carbon tetrachloride-induced acute hepatotoxicity in the rat. Journal of Ethnopharmacology. — PubMed
- Gutierrez R et al. (2010). Effects of rosemary extract on acetaminophen-induced hepatotoxicity in mice. Plant Foods for Human Nutrition. — PubMed
- Posadas SJ et al. (2009). Protective effects of rosemary extract on ethanol-induced hepatic injury. Journal of Medicinal Food. — PubMed
- Romo-Vaquero M et al. (2014). Bioavailability of rosemary phenolic diterpenes (carnosic acid, carnosol) in rats. PLoS One. — PubMed
- Tu Z et al. (2013). Carnosic acid attenuates ethanol-induced liver injury via Nrf2 pathway. Hepatology Research. — PubMed
- Vasileva LV et al. (2018). Antioxidant and anti-inflammatory effects of rosemary extract on the gastrointestinal mucosa. European Journal of Pharmacology. — PubMed
- Bozin B et al. (2007). Antimicrobial and antioxidant properties of rosemary and sage essential oils. Journal of Agricultural and Food Chemistry. — PubMed
- Borges RS et al. (2019). Rosmarinus officinalis essential oil: a review of its phytochemistry, anti-inflammatory activity, and mechanisms of action. Journal of Ethnopharmacology. — PubMed
- Allegra A et al. (2020). The dietary inhibitor rosemary extract: effects on COX-1 and COX-2 in the gut. Nutrients. — PubMed
- Mishra A et al. (2018). Rosemary extract in non-alcoholic fatty liver disease: a small randomized trial. Phytotherapy Research. — PubMed
- Andrade JM et al. (2018). Rosmarinus officinalis as a therapeutic agent in metabolic disorders. Phytomedicine. — PubMed
PubMed Topic Searches
- PubMed: Rosemary carminative / dyspepsia
- PubMed: Carnosic acid hepatoprotection
- PubMed: Rosemary cholagogue / bile
- PubMed: Rosemary and NAFLD
- PubMed: Rosemary and H. pylori
Connections
- Rosemary Overview
- Rosemary Benefits Hub
- Rosemary for Cognitive Function
- Rosemary for Antioxidant & Anti-Aging
- Rosemary for Hair Loss
- Peppermint (Carminative)
- Fennel (Carminative)
- Milk Thistle (Hepatoprotective)
- Dandelion (Cholagogue)
- Ginger (Digestive)
- N-Acetylcysteine (Acetaminophen Antidote)
- Glutathione
- Gastroenterology
- Hepatology
- All Herbs