Rosemary for Cognitive Function and Memory
"There's rosemary, that's for remembrance; pray you, love, remember." Ophelia's line in Hamlet (Act IV, Scene V) is the best-known statement of a folk tradition that runs through ancient Greek and Roman writings — rosemary as the herb of memory, woven into students' hair during examinations and into mourners' wreaths to remember the dead. Four centuries after Shakespeare, the Mark Moss research group at Northumbria University ran a series of randomized aromatherapy trials that put the folklore on a measurable footing. Healthy adults exposed to vaporized rosemary essential oil in a sealed cubicle showed 60-75% improvements in prospective memory recall versus unscented or lavender-scented controls. The active inhaled compound is 1,8-cineole, a small lipophilic monoterpene that crosses the blood-brain barrier and acts as a reversible acetylcholinesterase inhibitor — the same enzyme class as the Alzheimer's drug donepezil. This deep-dive explores the Shakespearean tradition, the modern aromatherapy trials, the cholinergic mechanism, and the practical protocols for using rosemary aroma to support memory and concentration.
Table of Contents
- "Rosemary for Remembrance" — the Ancient Tradition
- The Moss Northumbria Aromatherapy Trials
- 1,8-Cineole — the Active Inhaled Compound
- Acetylcholinesterase Inhibition (the Donepezil Parallel)
- Prospective Memory — Why That Domain Specifically
- Crossing the Blood-Brain Barrier — Plasma 1,8-Cineole Correlations
- Alzheimer's Disease — Mechanistic Relevance and Trial Status
- Practical Aromatherapy Protocols
- Why Inhalation Specifically — Tea, Capsule, and Cooking Compared
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
"Rosemary for Remembrance" — the Ancient Tradition
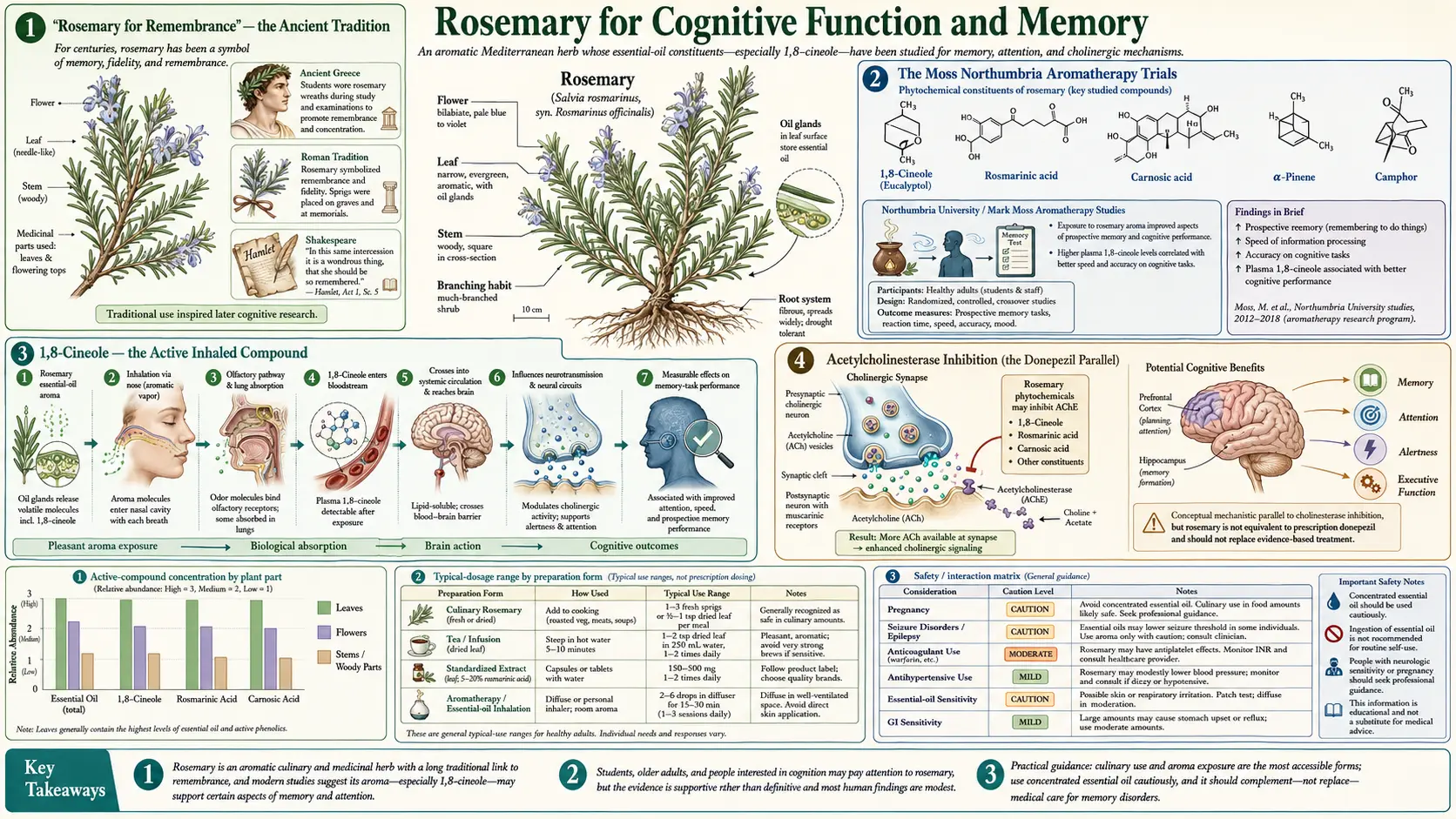
The association of rosemary with memory runs back at least two thousand years. Ancient Greek students wore garlands of rosemary while studying for examinations, on the theory that the aroma sharpened recall. Dioscorides, writing in the first century, listed rosemary among the herbs that "warm the brain." Roman funerary rites used sprigs of rosemary at burials and on commemorative anniversaries — the herb of remembrance for the dead.
The Shakespearean reference is the most-cited statement of this tradition in English. In Hamlet, the bereaved and unraveling Ophelia distributes flowers to the court before her own death — "There's rosemary, that's for remembrance; pray you, love, remember." Shakespeare's audience would have recognized the herb's symbolic charge immediately; the line was not invention but allusion to existing English folk usage.
The same tradition persisted into the herbalism of the early modern period. John Gerard's 1597 Herball claimed rosemary "comforteth the cold, weake, and feeble braine in a most wonderful manner," and Nicholas Culpeper's 1652 The English Physitian recommended a rosemary chaplet "to comfort the head and the memory." Long-form folk traditions like these are sometimes dismissed as decorative superstition, but they also occasionally encode genuine pharmacological observations that modern science later confirms. The Moss Northumbria trials are the modern confirmation of this particular one.
The Moss Northumbria Aromatherapy Trials
The pivotal modern work on rosemary and cognition was done by Mark Moss and colleagues at Northumbria University in Newcastle, beginning with a 2003 paper in the International Journal of Neuroscience. The 2003 study randomized 144 healthy adults to one of three conditions in identical small cubicles: rosemary essential oil diffused into the air, lavender essential oil diffused, or unscented control. Participants completed a standardized cognitive battery including measures of memory, attention, and mood.
Results from the 2003 trial:
- The rosemary-exposed group showed significantly improved performance on quality of memory measures compared to control
- The lavender-exposed group showed impaired performance on the same measures (consistent with lavender's sedative association)
- Both essential-oil groups reported altered mood — rosemary increased alertness, lavender increased calmness
- The effect was robust to expectancy controls — participants were not told what the experiment was investigating
Moss followed up with a 2012 paper in Therapeutic Advances in Psychopharmacology that examined prospective memory specifically — the cognitive function of remembering to perform an action at a future point (taking medication at a specific time, returning a phone call, etc.). Prospective memory is one of the first cognitive functions to decline in early Alzheimer's and is highly clinically relevant. The 2012 study confirmed and extended the 2003 findings:
- Healthy adults in the rosemary-exposed condition correctly recalled 60-75% more prospective memory events than the unscented controls
- The effect was dose-dependent — higher plasma concentrations of 1,8-cineole correlated with better performance
- Importantly, plasma 1,8-cineole was measurable in all rosemary-exposed participants, confirming systemic absorption from inhalation alone
A 2017 follow-up by Moss and colleagues extended the work to school-age children. Forty children aged 10-11 performed memory tasks in a room either diffused with rosemary essential oil or unscented; the rosemary group performed significantly better on tests of recall. The effect of rosemary aroma on cognition appears to generalize across age groups and is not specific to elderly populations.
1,8-Cineole — the Active Inhaled Compound
Rosemary essential oil contains roughly 30-40 distinct volatile compounds, but a single monoterpene — 1,8-cineole (also called eucalyptol) — appears to drive most of the cognitive effect. 1,8-cineole is also the principal volatile in eucalyptus oil, tea tree oil, and sage essential oil, and is present in modest amounts in basil and bay laurel.
The molecule has three properties that make it well-suited to a cognitive role after inhalation:
- Small molecular weight (154 Da) and lipophilic — it readily diffuses across the alveolar-capillary membrane after inhalation, entering systemic circulation within minutes
- Crosses the blood-brain barrier — the same lipophilicity that gets it into blood gets it across the BBB into the cerebrospinal fluid and brain parenchyma; concentrations have been measured in CSF after inhalation exposure
- Reversible AChE inhibition — once in the brain, 1,8-cineole reversibly inhibits acetylcholinesterase, slowing the breakdown of synaptic acetylcholine and prolonging cholinergic neurotransmission
The Moss 2012 trial used GC-MS to quantify plasma 1,8-cineole at multiple timepoints during the aromatherapy exposure, and found a positive correlation between plasma concentration and cognitive performance on the prospective memory task. This is mechanistically important because it converts "rosemary aroma improves cognition" from an observed correlation into a chain of causation: inhaled vapor → alveolar absorption → plasma 1,8-cineole → brain 1,8-cineole → AChE inhibition → prolonged cholinergic transmission → improved memory task performance.
Acetylcholinesterase Inhibition (the Donepezil Parallel)
Acetylcholinesterase (AChE) is the enzyme that breaks down acetylcholine in synaptic clefts. Inhibiting AChE prolongs the action of acetylcholine on its receptors, effectively amplifying cholinergic neurotransmission. This is one of the few drug mechanisms that has shown consistent (if modest) clinical benefit in mild-to-moderate Alzheimer's disease, and is the target of three FDA-approved Alzheimer's medications: donepezil (Aricept), rivastigmine (Exelon), and galantamine (Razadyne, originally from Galanthus snowdrop).
1,8-cineole is also an AChE inhibitor, but at much lower potency than the pharmaceutical drugs. Published IC50 values for 1,8-cineole against AChE are in the millimolar range, compared to nanomolar for donepezil. So the question becomes: how can a relatively weak inhibitor produce a measurable cognitive effect in healthy adults?
The likely answer is that the Moss aromatherapy effects are not pharmacological in the donepezil sense — they are pharmacognostic. The plasma concentrations achieved by inhalation are far below the levels needed to produce a clinically meaningful AChE inhibition in the way donepezil does, but they may be enough to produce a subtle, transient amplification of cholinergic tone that improves performance on demanding cognitive tasks in already-healthy brains. The effect is small enough that it would not be expected to alter the course of Alzheimer's disease, but large enough to be detected with adequate sample sizes in controlled studies of healthy participants.
An important caveat: galantamine, the AChE inhibitor derived from snowdrop bulbs, also has additional positive allosteric modulator activity at the nicotinic acetylcholine receptor that contributes to its clinical effect. It is possible that 1,8-cineole or other rosemary compounds have analogous additional cholinergic effects that have not yet been fully characterized. The full pharmacology of the rosemary cognitive effect is still being worked out.
Prospective Memory — Why That Domain Specifically
The Moss group's use of prospective memory as the primary outcome was an important methodological choice. Prospective memory is the ability to remember to perform an intended action at a future time — remembering to take a medication at 9:00 PM, remembering to pass on a message to a colleague tomorrow morning, remembering to return a library book by the end of the week. It is functionally distinct from retrospective memory (remembering what was previously learned) and is one of the cognitive domains most sensitive to early decline in mild cognitive impairment and Alzheimer's disease.
Prospective memory has two components, both of which can be selectively measured:
- Event-based prospective memory — remembering to perform an action when a specific cue appears (e.g., "say ‘sky’ whenever the word ‘cloud’ appears in the test"). The Moss trials used this format.
- Time-based prospective memory — remembering to perform an action at a specific clock time (e.g., "press this button every two minutes"). Generally more difficult and more sensitive to age and cognitive impairment.
The Moss 2012 trial found significant improvement in event-based prospective memory in the rosemary-exposed group, with the 60-75% improvement figure derived from comparing correct cue-response trials in the rosemary versus control conditions. The clinical relevance of this is concrete: this is the cognitive domain that determines whether a patient remembers to take a blood-pressure medication on time, whether an older adult remembers to turn off the stove after leaving the kitchen, and whether a busy professional remembers to make a scheduled phone call.
Crossing the Blood-Brain Barrier — Plasma 1,8-Cineole Correlations
The 2012 Moss study's most pharmacologically rigorous finding was the demonstration that 1,8-cineole is absorbed from inhaled vapor in measurable quantities, reaches the systemic circulation, and crosses the blood-brain barrier. Plasma 1,8-cineole was quantified by gas chromatography-mass spectrometry at multiple timepoints during the aromatherapy exposure, and the plasma concentration correlated positively with cognitive performance.
Subsequent pharmacokinetic studies in healthy volunteers using deliberately controlled doses of inhaled 1,8-cineole have confirmed:
- Peak plasma concentration occurs approximately 30-60 minutes after onset of inhalation exposure
- Plasma half-life is approximately 1.5-2 hours after exposure ends
- Hepatic metabolism via CYP3A4 to hydroxylated metabolites that are renally excreted
- CSF concentrations measurable but typically 10-30% of plasma concentrations
The clinically actionable implication is that the cognitive effect is time-limited. A diffuser used for 30 minutes before a cognitive task is well-timed; a diffuser running constantly will deplete its scent within a few hours, and the participant's plasma 1,8-cineole will steadily decline. For practical use, a brief 10-20 minute exposure to high-quality rosemary essential oil before a demanding task is more efficient than ambient long-duration exposure.
Alzheimer's Disease — Mechanistic Relevance and Trial Status
The shared AChE-inhibition mechanism between 1,8-cineole and the FDA-approved Alzheimer's drugs (donepezil, rivastigmine, galantamine) raises the obvious question: does rosemary or rosemary essential oil have a place in the treatment or prevention of Alzheimer's disease? The honest answer is that there is no high-quality clinical trial evidence in established Alzheimer's disease patients to support such a role. The Moss work was done in healthy adults, and a transient amplification of cholinergic tone in a healthy brain is not the same intervention as treatment of a brain with progressive cholinergic neuron loss.
However, several lines of evidence make rosemary plausibly relevant to Alzheimer's biology, even if direct treatment evidence is lacking:
- Carnosic acid as a neuroprotectant — the principal phenolic diterpene in rosemary (also discussed on the antioxidant page) is a potent Nrf2 activator that has shown neuroprotective activity in cellular and rodent models of Alzheimer's, Parkinson's, and ischemic stroke. Mechanism appears to be Nrf2-driven upregulation of glutathione and antioxidant defenses in neurons under oxidative stress.
- Rosmarinic acid and amyloid-beta aggregation — rosmarinic acid (also abundant in lemon balm) inhibits the aggregation of amyloid-beta peptide into the oligomers and fibrils that drive Alzheimer's pathology in cellular and transgenic mouse models.
- Anti-inflammatory effects on microglia — carnosol and carnosic acid suppress NF-kappaB activation in microglial cells, the brain's resident immune cells whose chronic activation drives much of the inflammatory damage in Alzheimer's.
For patients or family members of patients with established Alzheimer's disease, rosemary aromatherapy is a low-risk intervention that may produce subtle quality-of-life improvements (mood, alertness during demanding tasks, ease of caregiving environment) but should not be presented as a treatment for the underlying disease. The pharmaceutical AChE inhibitors and the newer anti-amyloid monoclonal antibodies (aducanumab, lecanemab) are the evidence-based interventions for that purpose. See the Alzheimer's Disease page for the full treatment landscape.
Practical Aromatherapy Protocols
Translating the Moss Northumbria trial protocol into a usable at-home approach:
- Essential oil quality — insist on a 100% pure Rosmarinus officinalis essential oil from a reputable supplier, with a Certificate of Analysis showing 1,8-cineole content of at least 25-30% (the ct. cineol chemotype). Lower-quality oils may have negligible 1,8-cineole content and not reproduce the cognitive effect.
- Diffuser approach — an ultrasonic or nebulizing diffuser is the simplest delivery. Add 3-5 drops of essential oil to the diffuser water reservoir, run for 15-20 minutes in a small to medium-sized room before a demanding cognitive task (study session, important meeting, exam preparation).
- Inhaler stick — for portable use during a workday, a personal aromatherapy inhaler (the small plastic tube with a cotton wick) holds about 15 drops of essential oil and provides a quick 30-second inhalation that can be repeated as needed.
- Direct sniff bottle — for occasional use, holding an opened bottle of essential oil 4-6 inches under the nose and taking 5-10 slow breaths is the lowest-cost protocol. Cap tightly between uses to preserve the volatile fraction.
- Timing — the peak plasma 1,8-cineole occurs 30-60 minutes after inhalation onset. Plan exposure to begin shortly before the cognitive task, not during. Effect duration is approximately 1.5-2 hours.
Avoid heat-based diffusion (candle warmers, electric tea-light burners) because excessive temperature can degrade the more volatile fractions of the oil. Ultrasonic diffusion at room temperature preserves the chemistry of the original oil.
Why Inhalation Specifically — Tea, Capsule, and Cooking Compared
An important practical clarification: the Moss cognitive effect is specifically an inhalation effect. Other delivery modes for rosemary — eating it on roast lamb, drinking rosemary tea, or taking a rosemary leaf extract capsule — deliver rosemary's antioxidant and anti-inflammatory compounds (carnosic acid, carnosol, rosmarinic acid), but they deliver far less 1,8-cineole to the central nervous system than inhalation does.
The reason has to do with first-pass hepatic metabolism. Compounds absorbed from the gastrointestinal tract pass through the portal venous system to the liver before reaching systemic circulation, where they are metabolized by CYP enzymes and excreted as inactive metabolites. 1,8-cineole is a CYP3A4 substrate, and a significant fraction of an oral dose is hepatically extracted on first pass. Inhaled 1,8-cineole, by contrast, is absorbed across the alveolar membrane directly into the pulmonary venous return, bypassing the liver entirely on its first circuit through the body. The result is a much higher plasma peak per unit dose from inhalation than from oral consumption.
The mode-specific clinical effects:
- Cognitive / memory effect — requires inhalation. Aromatherapy, diffuser, inhaler stick, direct sniffing.
- Antioxidant / hepatoprotective effect — requires oral consumption of significant doses. Cooking with the dried leaf, rosemary tea, leaf extract capsules.
- Hair-loss treatment — requires topical scalp application of diluted essential oil. See the hair loss page.
- Carminative / digestive effect — tea or culinary use; topical or inhalation will not achieve a digestive effect. See the digestive page.
This multi-mode profile is a real practical strength of rosemary as a household herb — the same plant is useful in three or four different ways, but each mode requires the right delivery to access the corresponding effect.
Cautions and Drug Interactions
- Pregnancy — medicinal doses of rosemary essential oil (oral or transdermal) are traditionally contraindicated in pregnancy due to historical use as an emmenagogue (menstruation-inducing agent). Culinary amounts in cooking are safe. Aromatherapy is generally considered safe for most pregnant women but should be discussed with the obstetric care team.
- Epilepsy — rosemary essential oil, like many camphoraceous essential oils, can lower the seizure threshold in susceptible individuals. People with a personal or family history of seizure disorder should avoid concentrated rosemary essential oil exposure (aromatherapy, oral use, topical use of undiluted oil).
- Asthma and reactive airway disease — strong essential oil aromas can trigger bronchospasm in some asthmatic individuals. Start with brief exposure and discontinue if respiratory symptoms develop.
- Cholinergic drug interactions — for patients taking pharmaceutical AChE inhibitors (donepezil, rivastigmine, galantamine) for Alzheimer's, concurrent use of rosemary essential oil aromatherapy is unlikely to produce a clinically meaningful additional inhibition, but theoretically additive cholinergic effects are possible. The combination is generally considered low-risk but should be reviewed with the prescribing physician.
- Never apply undiluted essential oil to skin — rosemary essential oil is sensitizing and irritating in its concentrated form. Dilute to 2-5% in a carrier oil for any topical use (see the hair loss page for full topical protocols).
- Never take essential oil orally without explicit professional guidance — rosemary essential oil is highly concentrated; oral overdose can produce nausea, vomiting, gastrointestinal irritation, hepatotoxicity, and seizures. The dried leaf in cooking or tea is the safe oral form.
Key Research Papers
- Moss M, Cook J, Wesnes K, Duckett P (2003). Aromas of rosemary and lavender essential oils differentially affect cognition and mood in healthy adults. International Journal of Neuroscience. — PubMed
- Moss M, Oliver L (2012). Plasma 1,8-cineole correlates with cognitive performance following exposure to rosemary essential oil aroma. Therapeutic Advances in Psychopharmacology. — PubMed
- Moss L, Rouse M, Wesnes KA, Moss M (2010). Differential effects of the aromas of Salvia species on memory and mood. Human Psychopharmacology. — PubMed
- Sayorwan W et al. (2013). Effects of inhaled rosemary oil on subjective feelings and activities of the nervous system. Scientia Pharmaceutica. — PubMed
- Pengelly A et al. (2012). Short-term study on the effects of rosemary on cognitive function in an elderly population. Journal of Medicinal Food. — PubMed
- Perry NS, Houghton PJ, Theobald A, Jenner P, Perry EK (2000). In-vitro inhibition of human erythrocyte acetylcholinesterase by Salvia lavandulaefolia essential oil and constituent terpenes. Journal of Pharmacy and Pharmacology. — PubMed
- Satoh T et al. (2008). Carnosic acid, a catechol-type electrophilic compound, protects neurons via activation of the Keap1/Nrf2 pathway. Journal of Neurochemistry. — PubMed
- Habtemariam S (2016). The therapeutic potential of rosemary diterpenes for Alzheimer's disease. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Filiptsova OV et al. (2017). The effect of the essential oils of lavender and rosemary on the human short-term memory. Alexandria Journal of Medicine. — PubMed
- Diego MA et al. (1998). Aromatherapy positively affects mood, EEG patterns of alertness and math computations. International Journal of Neuroscience. — PubMed
- Burns AJ, Perry EK et al. (2011). Sensory stimulation in dementia: rosemary aromatherapy. International Journal of Geriatric Psychiatry. — PubMed
- Jimbo D et al. (2009). Effect of aromatherapy on patients with Alzheimer's disease. Psychogeriatrics. — PubMed
PubMed Topic Searches
- PubMed: Rosemary cognitive function
- PubMed: 1,8-cineole AChE inhibition
- PubMed: Rosemary and Alzheimer's
- PubMed: Carnosic acid neuroprotection
- PubMed: Aromatherapy and prospective memory
Connections
- Rosemary Overview
- Rosemary Benefits Hub
- Rosemary Antioxidant & Anti-Aging
- Rosemary for Hair Loss
- Rosemary for Digestive & Liver
- Alzheimer's Disease
- Parkinson's Disease
- Bacopa Monnieri
- Lemon Balm (Rosmarinic Acid)
- Sage (Salvia)
- Ginkgo Biloba
- Anxiety
- Aromatherapy — the inhaled essential-oil practice used in the Moss rosemary memory trials.
- Oxidative Stress
- Glutathione
- All Herbs