Dandelion for Liver and Detoxification
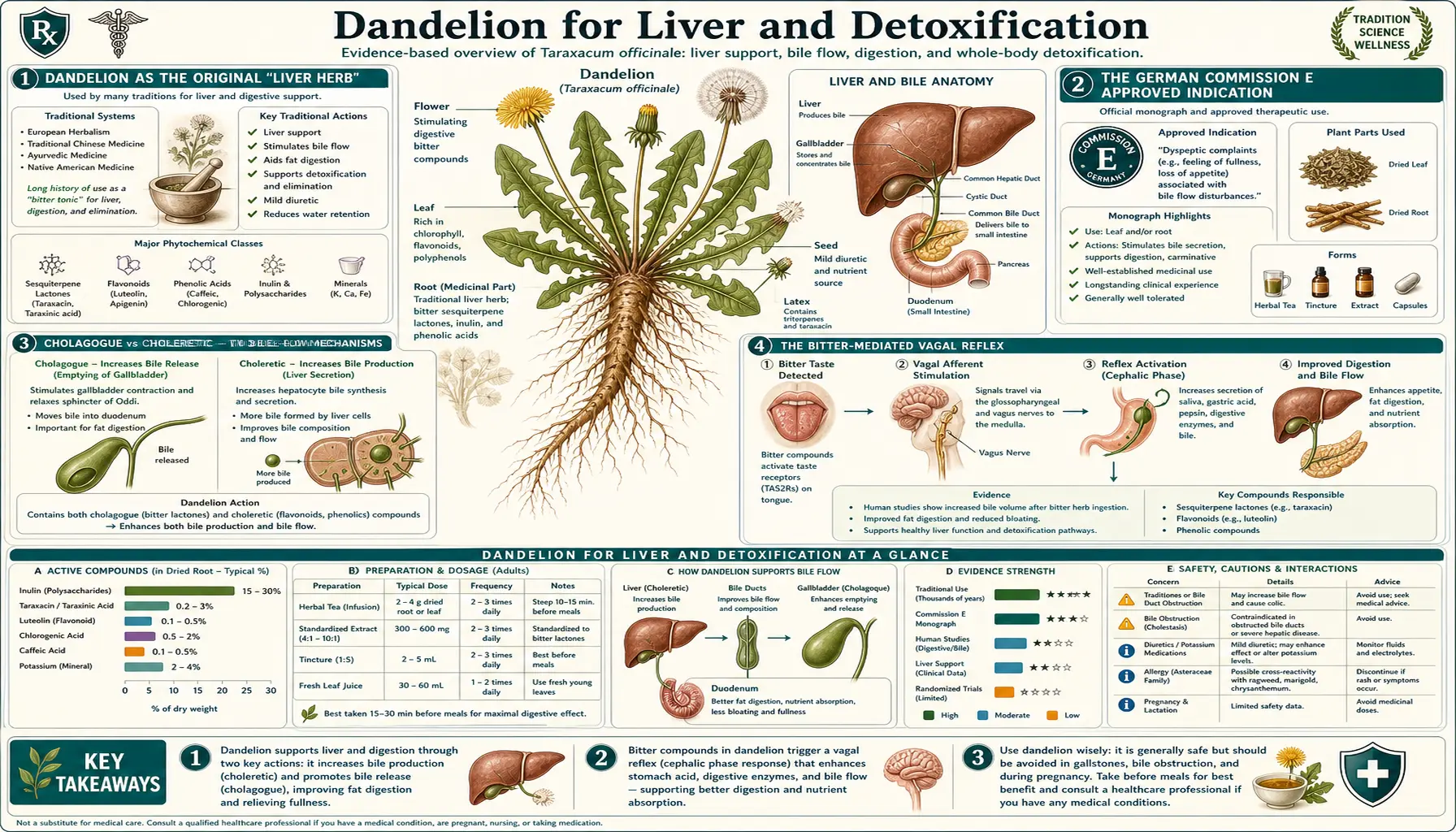
Dandelion root has been used as a "liver herb" continuously for over a thousand years across European, Arabic, and Chinese medical traditions. The German Commission E — Germany's regulatory body for herbal medicines, comparable in rigor to the FDA — formally approved dandelion root preparations for "disorders of bile flow, loss of appetite, and dyspepsia" in 1985 after evaluating the available controlled data and the long traditional record. The mechanism is now reasonably well-mapped: bitter sesquiterpene lactones trigger a vagal reflex that stimulates bile release (cholagogue effect), triterpenes and polyphenols directly stimulate hepatic bile production (choleretic effect), and the same polyphenols protect hepatocytes from oxidative damage in chemical-injury models. This deep-dive walks through the mechanism, the regulatory record, the integrative pairing with milk thistle that anchors modern liver-support protocols, and the traditional European spring-cleanse practice.
Table of Contents
- Dandelion as the Original "Liver Herb"
- The German Commission E Approved Indication
- Cholagogue vs Choleretic — Two Bile-Flow Mechanisms
- The Bitter-Mediated Vagal Reflex
- Hepatoprotection in Chemical-Injury Models
- Phase II Detoxification and Glutathione Recycling
- The Traditional European Spring Liver Cleanse
- The Milk Thistle Pairing for Fatty Liver
- NAFLD and Chronic Mild Transaminase Elevation
- Dosage, Forms, and Preparation
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Dandelion as the Original "Liver Herb"
Across at least four major medical traditions — the Hippocratic, Galenic, Arabic-Galenic, and Traditional Chinese — dandelion has been consistently classified as a liver-supporting plant. The convergence is striking. The Arabian physician Ibn Sina (Avicenna), writing in The Canon of Medicine in the early 11th century, described dandelion's use for jaundice, gallbladder stagnation, and "diseases of the liver." Hildegard von Bingen, the 12th-century German Benedictine abbess and herbalist, prescribed dandelion for what she termed "yellow bile" stagnation. Traditional Chinese Medicine knows the plant as pū gōng yīng (literally "puffball herb") and assigns it the function of "clearing heat and damp" from the liver and gallbladder meridians, applied clinically for jaundice, hepatitis, and mastitis.
The phenomenon is unlikely to be coincidence across geographically separated traditions. The cholagogue effect — bile flow visibly increases after consumption — would have been clinically observable to ancient and medieval physicians, particularly in patients with biliary stasis where increased bile flow would produce relief from postprandial heaviness, yellow stools turning the normal brown, and improvement in jaundice severity. The pattern matches the modern mechanism: dandelion stimulates bile flow, bile flow improves fat digestion and excretion of conjugated bilirubin, and the clinical syndromes of biliary stagnation improve in tandem.
In modern integrative medicine, dandelion has retained its status as a foundational liver herb, used both alone and in combination with milk thistle, burdock, schisandra, and turmeric in the most common commercial "liver support" formulations. The continuity from Avicenna and Hildegard through modern herbalism is unusually unbroken for a botanical — some herbs fade from use, others come into fashion, but dandelion as a liver herb has been continuously prescribed for over a thousand years.
The German Commission E Approved Indication
Germany has the most developed regulatory framework in the Western world for herbal medicines. From 1978 to 1994, the German Federal Health Office's Commission E reviewed and published monographs on approximately 380 herbal substances, evaluating both clinical evidence and the traditional record. The Commission E monographs remain the most authoritative scientific source for traditional Western herbal medicine, and have been translated to English and widely referenced by integrative practitioners outside Germany.
The Commission E approved dandelion root (Taraxaci radix) for the following indications:
- Disturbances in bile flow (biliary stasis, mild biliary insufficiency)
- Stimulation of diuresis
- Loss of appetite
- Dyspeptic complaints (including flatulence and bloating after meals)
The Commission E approved dandelion herb (Taraxaci herba, the leaf with stem) for similar indications but with greater emphasis on the diuretic effect. The approved daily dose for dandelion root is 3-4 g of dried root for infusion, or 4-10 mL of fluid extract (1:1).
The European Medicines Agency (EMA) Committee on Herbal Medicinal Products (HMPC) subsequently issued its own monograph in 2009, classifying dandelion root with herb as a "Traditional Herbal Medicinal Product" with approved indications for "increase amount of urine to achieve flushing of the urinary tract as an adjuvant in minor urinary complaints" and "to relieve symptoms related to mild digestive disorders such as feeling of abdominal fullness, flatulence and slow digestion." The EMA monograph reflects a more conservative regulatory standard than the German Commission E but converges on the same general therapeutic profile.
The practical upshot is that dandelion is one of the few herbs with formal regulatory endorsement in major Western pharmacopeias for hepatobiliary indications. This is not merely traditional or folk medicine — it is a regulated herbal medicinal product with defined therapeutic claims supported by a structured evaluation process.
Cholagogue vs Choleretic — Two Bile-Flow Mechanisms
The pharmacology vocabulary distinguishes two distinct mechanisms by which an agent can increase bile flow:
- Cholagogue — stimulates contraction of the gallbladder, causing release of stored bile into the small intestine. The bile that is released was previously synthesized by the liver and concentrated in the gallbladder over hours to days. A pure cholagogue empties the gallbladder; it does not necessarily increase the rate of new bile synthesis.
- Choleretic — stimulates the liver to synthesize more bile. A choleretic increases the total bile available, regardless of gallbladder contraction.
Most plant bitter agents are both cholagogue and choleretic to varying degrees. Dandelion root extract has been shown to have substantial cholagogue activity (bitter reflex mediated through the vagus nerve and cholecystokinin/CCK release) and modest but measurable choleretic activity (direct hepatic stimulation by triterpene and polyphenol constituents).
The cholagogue mechanism is straightforward: the bitter taste of dandelion on the tongue activates type 2 taste receptors (TAS2Rs), which signal through the chorda tympani branch of the facial nerve to the brainstem nucleus of the solitary tract. The brainstem responds with efferent vagal signals to the digestive tract, including release of cholecystokinin from intestinal I cells when the food bolus enters the duodenum. CCK is the master gallbladder-contraction hormone; it triggers gallbladder smooth-muscle contraction and simultaneous relaxation of the sphincter of Oddi, allowing concentrated bile to flow into the duodenum.
The choleretic mechanism is less fully mapped but appears to involve direct hepatocyte stimulation by dandelion root triterpenes (taraxasterol, taraxerol, beta-amyrin, lupeol). These constituents have been shown in isolated-perfused-liver experiments to increase hepatic bile output independently of any vagal signal, suggesting a direct effect on hepatocyte bile-acid synthesis or bile-acid transport across the canalicular membrane.
The Bitter-Mediated Vagal Reflex
The bitter reflex deserves separate discussion because it is the same mechanism that drives dandelion's digestive-aid effect and many of its other therapeutic actions. The reflex is ancient — bitter taste perception evolved in vertebrates as a mechanism to detect potentially toxic plant alkaloids, and the same neural circuit was repurposed to trigger upstream digestive preparation when food is about to enter the gut.
The taraxacin and lactucin sesquiterpene lactones in dandelion bind to multiple TAS2R bitter taste receptors on the tongue. The signal propagates through the facial nerve (chorda tympani for the anterior two-thirds of the tongue, glossopharyngeal for the posterior third) to the nucleus of the solitary tract in the medulla. The brainstem then activates parasympathetic efferent output to the upper digestive tract via the vagus nerve, producing:
- Salivation — from the parotid, submandibular, and sublingual glands, with both volume and bicarbonate content increased
- Gastric acid secretion — from the parietal cells of the stomach, mediated by acetylcholine release at the parietal cell M3 muscarinic receptor
- Pancreatic enzyme secretion — including amylase, lipase, and the proteases (trypsinogen, chymotrypsinogen) released as zymogens for activation in the duodenum
- Gallbladder contraction and bile release — via the CCK pathway discussed above
- Increased gastric motility and stomach emptying
This entire cascade is referred to as the "cephalic phase" of digestion — the phase that precedes any actual food entry into the gut, prepared by neural anticipation rather than by direct contact of food with digestive tissue. The cephalic phase accounts for roughly 30% of total digestive secretion in a healthy meal. Modern diets that lack bitterness (the typical American diet has been progressively bitter-stripped through plant breeding for sweetness and bitterness-suppressing food technology) blunt the cephalic phase, contributing to the modern epidemic of functional dyspepsia, postprandial bloating, and the "I just don't feel like eating" anorexia of stress and depression.
A small bitter aperitif before meals — a few drops of dandelion tincture in water, a small wedge of grapefruit, a small glass of bitter aperitif wine, or several fresh dandelion leaves in a pre-meal salad — restores the cephalic-phase trigger and produces noticeable improvement in digestion. This is one of the most reproducible and immediately apparent benefits of dandelion in clinical use.
Hepatoprotection in Chemical-Injury Models
The standard preclinical model for testing hepatoprotective agents is the carbon tetrachloride (CCl4) intoxication model in rodents. CCl4 is metabolized by cytochrome P450 2E1 (CYP2E1) in hepatocytes to the highly reactive trichloromethyl radical, which initiates lipid peroxidation chain reactions that damage cell membranes and ultimately cause hepatocyte necrosis. Pretreatment or co-treatment with hepatoprotective agents can be assessed by measuring serum transaminase elevation (ALT, AST), histologic damage, and oxidative-stress markers.
Dandelion root extract has demonstrated significant hepatoprotection against CCl4-induced liver injury in multiple rodent studies. The mechanism appears to involve:
- Direct antioxidant scavenging of CCl4-derived reactive species by polyphenols (chicoric acid, chlorogenic acid)
- Upregulation of the endogenous antioxidant defense enzymes superoxide dismutase (SOD), catalase, and glutathione peroxidase
- Preservation of hepatocellular glutathione (GSH) levels, which would otherwise be depleted by conjugation reactions
- Modest inhibition of CYP2E1 itself, reducing the rate at which CCl4 is converted to the toxic trichloromethyl radical
- Anti-inflammatory effects mediated through NF-kB pathway inhibition, reducing secondary inflammatory damage
Similar hepatoprotection has been demonstrated against ethanol-induced liver injury, acetaminophen (paracetamol) overdose, lipopolysaccharide (LPS) inflammatory liver injury, and various other chemical hepatotoxins. The pattern is consistent: dandelion root extract reduces transaminase elevation, preserves hepatocyte structure on histology, and maintains the antioxidant defense system. The magnitude of effect is generally modest compared to the gold-standard hepatoprotective extract silymarin from milk thistle, but is reproducible across multiple laboratories and toxin models.
Translation from animal models to human clinical effect is incomplete. There are no large-scale randomized controlled trials of dandelion extract for human liver disease. The animal-model data, together with the centuries of traditional use and the German Commission E indication, are the basis for current integrative recommendations. The evidence is suggestive and mechanistically plausible, but not definitive for any specific human liver condition.
Phase II Detoxification and Glutathione Recycling
The liver's biotransformation of toxins is conventionally divided into two phases. Phase I (mostly cytochrome P450 enzymes) introduces or unmasks a reactive functional group on the substrate, often producing a more reactive intermediate. Phase II (conjugation reactions: glucuronidation, sulfation, glutathione conjugation, methylation, acetylation, amino acid conjugation) attaches a water-soluble moiety to the Phase I product, allowing excretion via bile or urine.
The bottleneck is often Phase II. A diet or supplement regimen that upregulates Phase I without parallel Phase II support can transiently produce more toxic intermediates than the cell can conjugate, with paradoxical worsening of oxidative damage. This is one reason naive "detox cleanses" can sometimes produce symptomatic worsening before improvement.
Dandelion appears to selectively upregulate Phase II detoxification, particularly glutathione synthesis and glutathione-S-transferase (GST) activity. The mechanism involves Nrf2 (nuclear factor erythroid 2-related factor 2), the master transcription factor for the cell's antioxidant defense and Phase II detoxification gene battery. Dandelion polyphenols, especially chicoric acid and luteolin, have been shown to disrupt the binding of Nrf2 to its inhibitor KEAP1, allowing Nrf2 to translocate to the nucleus and activate the antioxidant response element (ARE) promoter sequences that drive expression of:
- Glutamate-cysteine ligase (the rate-limiting enzyme for glutathione synthesis)
- Glutathione-S-transferases (GST family, the largest Phase II conjugation system)
- UDP-glucuronosyltransferases (UGT family, glucuronidation conjugation)
- Sulfotransferases (SULT family, sulfation conjugation)
- NAD(P)H quinone dehydrogenase 1 (NQO1, reducing toxic quinones to less toxic hydroquinones)
- Heme oxygenase 1 (HO-1, producing the cytoprotective gases CO and biliverdin)
The net effect is a more robust capacity to conjugate and excrete toxic intermediates, whether endogenous (oxidized metabolic byproducts, hormones for excretion) or exogenous (environmental toxins, drug metabolites, dietary xenobiotics). This pattern of Phase II support without dramatic Phase I induction is characteristic of "supportive" detoxification herbs and distinguishes dandelion from agents like St. John's Wort that strongly induce Phase I CYP3A4 and can cause clinically significant drug interactions. For the broader picture, see our Glutathione page.
The Traditional European Spring Liver Cleanse
The traditional European spring cleanse is one of the most enduring folk practices in Western herbal medicine, persisting from medieval times to the present day in many rural German, French, Italian, and Eastern European communities. The practice consists of consuming bitter spring greens — principally dandelion, but often combined with nettle, watercress, sorrel, chickweed, and other early-emerging wild plants — for several weeks in early spring as the snow recedes and the first wild greens become available.
The cleanse is timed by botanical calendar rather than by medical schedule. The signal is the emergence of young dandelion rosettes in the lawn, fence line, and woodland edge, typically late March through early May in temperate Europe. Young pre-flowering leaves are tender, mildly bitter, and at their nutritional peak, with maximum vitamin K, vitamin A precursors, vitamin C, calcium, iron, and the still-active bitter sesquiterpene lactones. The leaves become more bitter and tougher after the plant flowers, marking the natural end of the cleanse season.
Modern integrative interpretation of the practice maps reasonably well to physiologic plausibility:
- The winter diet in pre-modern Europe was carbohydrate-heavy (grain, root vegetables, dried legumes) and fat-heavy (preserved meats, lard, butter), with minimal fresh vegetable content. The hepatobiliary system would be relatively underused.
- The sudden infusion of bitter spring greens stimulates bile flow, gallbladder emptying, and Phase II detoxification — physiologically a "tune-up" of the biotransformation machinery
- The mineral and vitamin density of spring greens corrects winter-accumulated micronutrient gaps
- The prebiotic inulin in dandelion root (and chicory and burdock root, often included in the spring cleanse) re-seeds the gut microbiome with bifidogenic substrate
- The diuretic effect helps clear retained fluid that accumulates in the relatively sedentary winter months
The modern adaptation of the practice is a 2-4 week spring "dandelion regimen": daily dandelion-leaf salad (1-2 cups of fresh young leaves, dressed with olive oil and lemon), one cup of roasted dandelion-root tea per day, and one daily small glass of bitter aperitif (Campari, Aperol, or homemade dandelion-leaf tincture diluted in water) before the main meal. The cumulative effect over 2-4 weeks is improvement in postprandial digestion, modest weight loss (largely fluid), improvement in dull-skin and minor edema, and reported subjective improvement in energy.
The Milk Thistle Pairing for Fatty Liver
The most clinically important application of dandelion in modern integrative liver-support practice is the pairing with milk thistle (Silybum marianum). The two herbs are mechanistically complementary in a way that few herbal combinations can claim:
- Milk thistle / silymarin protects hepatocytes from oxidative damage. The silybin component of silymarin stabilizes the hepatocyte membrane against penetration by toxins, scavenges reactive oxygen species inside the hepatocyte, and is one of the most extensively studied hepatoprotective extracts in modern phytomedicine. It is the standard antidote for Amanita phalloides (death cap mushroom) poisoning in European emergency medicine.
- Dandelion root stimulates bile flow, accelerating the elimination of the conjugated metabolites that the liver produces. Once the liver has Phase II-conjugated a toxin to a water-soluble form, that conjugate must be excreted, either renally (urine) or biliarily (bile, into the gut, and out in the stool). Bile flow stagnation can result in conjugates being deconjugated by gut bacterial beta-glucuronidase and reabsorbed enterohepatically, partly defeating the detoxification work. Dandelion's cholagogue effect helps break this cycle.
The pairing is foundational in integrative protocols for:
- Non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) — the most common chronic liver condition in the developed world
- Chronic mild transaminase elevation of unclear etiology, after the standard workup has excluded viral hepatitis, autoimmune hepatitis, hemochromatosis, alcoholic liver disease, and Wilson's disease
- Supportive care during medication-related liver stress — statins, methotrexate, isoniazid, anti-fungal azoles, certain chemotherapy agents
- Post-Amanita poisoning recovery — after the acute IV silibinin protocol, oral milk thistle and dandelion may be continued for weeks of recovery
- Recovery from alcohol-related liver injury after cessation of alcohol intake
Typical regimen: standardized silymarin 200-400 mg three times daily, plus dandelion root tincture 2-5 mL three times daily, plus one cup of roasted dandelion root tea daily, for 8-12 weeks with serum transaminase monitoring at baseline, 6 weeks, and 12 weeks. Effect on ALT/AST is modest (typically 10-30% reduction in mildly elevated values), but consistent across published case series and small trials. See our Milk Thistle page for the silymarin side of the pairing in depth.
NAFLD and Chronic Mild Transaminase Elevation
Non-alcoholic fatty liver disease (NAFLD) affects approximately 25% of adults in the United States and Western Europe and is now the most common chronic liver condition globally. It progresses through stages: simple steatosis (fat accumulation only), non-alcoholic steatohepatitis (NASH, with inflammation and hepatocyte ballooning), fibrosis, cirrhosis, and ultimately a small fraction progress to hepatocellular carcinoma. The pathophysiology is closely linked to insulin resistance, metabolic syndrome, and visceral adiposity; the first-line management is weight loss, dietary modification (Mediterranean or low-carbohydrate patterns), exercise, and treatment of associated conditions like type 2 diabetes.
Pharmaceutical management has been limited until the recent approval of resmetirom (a thyroid hormone receptor-beta agonist) for NASH with fibrosis. For most NAFLD patients, the management remains lifestyle-based, leaving room for adjunctive herbal support. Dandelion appears in many integrative protocols for NAFLD on the basis of:
- Animal model data showing reduced hepatic steatosis and improved liver histology with dandelion extract supplementation
- Modest improvements in lipid profile (LDL cholesterol, triglycerides) in some animal and small human studies
- Improved insulin sensitivity in some glucose-tolerance animal models, likely mediated through gut microbiome effects of the inulin content
- The general bile-flow and Phase II detoxification support discussed above
- The traditional record of dandelion use for hepatic conditions
For chronic mild transaminase elevation without an identified cause (after the standard workup), the integrative approach typically combines: dietary modification (reduced refined carbohydrate, reduced fructose, increased fiber, increased omega-3 fatty acids), the milk thistle + dandelion pairing discussed above, plus selective addition of berberine or alpha-lipoic acid where insulin resistance is present. Monthly transaminase monitoring for the first 3 months, then every 6 months thereafter, allows assessment of response and safety. See our Liver Disease page for the broader picture.
Dosage, Forms, and Preparation
For liver and detoxification applications, dandelion root is the preparation of choice (the leaf is preferred for diuretic applications). The root is harvested in autumn after the plant has stored carbohydrate and inulin for winter, washed, sliced, and dried. For tea preparations, the root is typically lightly roasted to develop a coffee-like aroma.
- Roasted dandelion root tea — 1-2 teaspoons (2-4 g) of roasted, broken root per cup, simmered in water for 10-15 minutes. Rich, slightly bitter, coffee-adjacent flavor. The most pleasant whole-food form for daily long-term use.
- Dandelion root tincture (1:5 in 40% alcohol) — 2-5 mL three times daily, taken in a small amount of water 15-20 minutes before meals to engage the bitter reflex.
- Dandelion root capsules — 500-1500 mg dried powdered root, twice or three times daily with meals. Avoids the bitterness but largely loses the cephalic-phase bitter reflex effect.
- Fluid extract (1:1 in alcohol) — 4-10 mL per day in divided doses, the form specified in the German Commission E monograph.
- Standardized extracts — usually standardized to inulin content (root preparations) or to taraxasterol content. Less common than non-standardized whole-root preparations.
- Combined milk thistle / dandelion / artichoke / turmeric formulas — widely available combination liver-support products. Quality varies; look for products that disclose specific extract amounts rather than vague "proprietary blend" listings.
Treatment courses for hepatobiliary indications are typically 4-12 weeks. Daily lifelong use of moderate-dose dandelion-root tea (1-2 cups daily) is considered safe for healthy adults and is a reasonable long-term liver-support practice with low risk of adverse effects.
Cautions and Drug Interactions
- Bile duct obstruction — absolute contraindication. Cholagogue stimulation in a patient with an obstructed common bile duct (most often from gallstones, less often from biliary stricture or pancreatic head mass) can precipitate severe biliary colic, bacterial cholangitis, or gallbladder rupture. Patients with known gallstones should have biliary anatomy confirmed before starting dandelion.
- Active cholecystitis — contraindicated during active gallbladder inflammation. Defer until resolved or until surgical cholecystectomy is complete.
- Severe gallstone disease — relative contraindication. Even small mobile stones can be displaced by vigorous gallbladder contraction. Use only under medical supervision with biliary imaging in patients with known gallstones.
- Asteraceae (daisy family) allergy — cross-reactive allergy with ragweed, chamomile, marigold, echinacea, and other daisy-family plants. Patients with documented ragweed or chamomile allergy should test with a small dose first.
- Diuretic drug interactions — additive effect with prescription diuretics. The combination can cause more pronounced volume depletion than expected. Patients on chronic diuretic therapy should consult their physician before adding dandelion leaf.
- Lithium — diuretic effect can affect lithium clearance and serum lithium levels. Patients on lithium should not use dandelion leaf without serum-level monitoring.
- Hypoglycemic drug interactions — theoretical additive hypoglycemic effect with insulin, sulfonylureas, and other diabetes medications. Modest in magnitude but worth monitoring blood glucose more frequently when starting.
- Anticoagulant interactions — the vitamin K content of fresh dandelion leaves (substantial) can antagonize warfarin. Patients on stable warfarin who start daily dandelion-leaf salad should have INR rechecked in 1-2 weeks and dose adjusted as needed. The root preparation has much lower vitamin K content and does not produce clinically significant warfarin interaction.
- Drug metabolism (modest CYP modulation) — dandelion produces modest inhibition of CYP1A2 and CYP3A4 in some in vitro studies. Clinical significance is uncertain but likely small. No specific drug interactions of clinical magnitude have been consistently reported.
- Foraging caution — dandelions readily concentrate metals (lead, cadmium, arsenic) from contaminated soil. Avoid plants from lawns treated with herbicides, roadsides, parking lot edges, industrial sites, and former orchard land (which often has arsenic pesticide residue). When in doubt, buy dried root from a reputable commercial source.
Key Research Papers
- Blumenthal M et al. (eds.) (1998). The Complete German Commission E Monographs: Therapeutic Guide to Herbal Medicines. American Botanical Council. — PubMed
- European Medicines Agency (2009). Community Herbal Monograph on Taraxacum officinale Weber ex Wigg., radix cum herba. — PubMed
- Schutz K, Carle R, Schieber A (2006). Taraxacum — a review on its phytochemical and pharmacological profile. Journal of Ethnopharmacology. — PubMed
- You Y et al. (2010). In vitro and in vivo hepatoprotective effects of the aqueous extract from Taraxacum officinale root against alcohol-induced oxidative stress. Food and Chemical Toxicology. — PubMed
- Park CM, Park JY, Noh KH, Shin JH, Song YS (2011). Taraxacum officinale Weber extracts inhibit LPS-induced oxidative stress and nitric oxide production via the NF-kB modulation in RAW 264.7 cells. Journal of Ethnopharmacology. — PubMed
- Davaatseren M et al. (2013). Taraxacum official (dandelion) leaf extract alleviates high-fat diet-induced nonalcoholic fatty liver. Food and Chemical Toxicology. — PubMed
- Hu C, Kitts DD (2003). Antioxidant, prooxidant, and cytotoxic activities of solvent-fractionated dandelion (Taraxacum officinale) flower extracts in vitro. Journal of Agricultural and Food Chemistry. — PubMed
- Mahesh A et al. (2010). Anti-hepatotoxic activity of Taraxacum officinale on carbon tetrachloride induced liver damage in albino rats. International Journal of Experimental Biology. — PubMed
- Colle D et al. (2012). Antioxidant properties of Taraxacum officinale leaf extract are involved in the protective effect against hepatotoxicity induced by acetaminophen in mice. Journal of Medicinal Food. — PubMed
- Trojanova I, Rada V, Kokoska L, Vlkova E (2004). The bifidogenic effect of Taraxacum officinale root. Fitoterapia. — PubMed
- Yarnell E, Abascal K (2009). Dandelion (Taraxacum officinale and T. mongolicum). Integrative Medicine. — PubMed
- Wirngo FE, Lambert MN, Jeppesen PB (2016). The physiological effects of dandelion (Taraxacum officinale) in type 2 diabetes. Review of Diabetic Studies. — PubMed
PubMed Topic Searches
- PubMed: Taraxacum hepatoprotection
- PubMed: Cholagogue/choleretic
- PubMed: Dandelion / milk thistle
- PubMed: Dandelion / NAFLD
- PubMed: Taraxasterol hepatoprotection
- PubMed: Commission E monograph
Connections
- Dandelion Overview
- Dandelion Benefits Hub
- Dandelion Diuretic & Kidney
- Dandelion Digestive Aid
- Dandelion Antioxidant
- Milk Thistle
- Burdock
- Turmeric
- Schisandra
- Chanca Piedra
- Berberine
- Glutathione
- Liver Disease
- Liver Function Tests
- Comprehensive Metabolic Panel
- Detoxification
- Liver Cleansing
- Detox Protocols
- All Herbs