Dandelion as a Digestive Aid
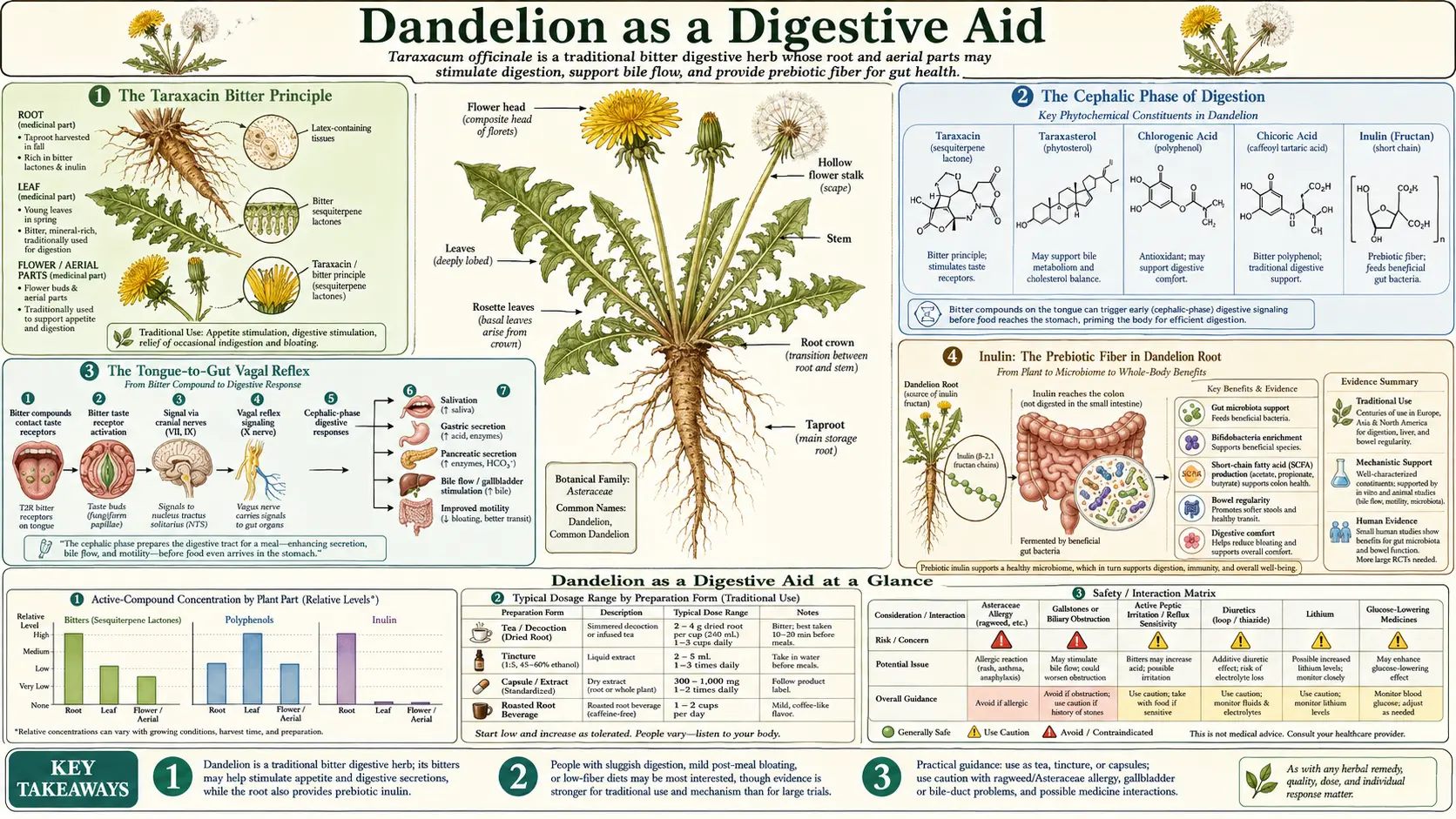
Dandelion is one of the classical "digestive bitters" of European traditional medicine, a category of herbs that work primarily through gustatory stimulation: the bitter principle (taraxacin, a sesquiterpene lactone) binds to bitter taste receptors on the tongue and triggers a vagal reflex that pre-stimulates the entire upstream digestive cascade — saliva, gastric acid, pancreatic enzymes, and bile — before food even reaches the gut. This is the "cephalic phase" of digestion, which the modern American diet has progressively stripped through plant breeding for sweetness and bitterness-suppressing food technology. The root of the plant also contains substantial inulin, a prebiotic fructan that selectively feeds bifidobacteria and produces short-chain fatty acids, supporting downstream gut barrier and microbiome health. This deep-dive walks through the bitter mechanism, the inulin prebiotic effect, the traditional aperitif use, the roasted-root dandelion coffee tradition, the adjunctive role in IBS and functional dyspepsia, and the practical "bitter before meals" protocol that produces noticeable improvement in digestion within days.
Table of Contents
- The Taraxacin Bitter Principle
- The Cephalic Phase of Digestion
- The Tongue-to-Gut Vagal Reflex
- Inulin: The Prebiotic Fiber in Dandelion Root
- Short-Chain Fatty Acids and Gut Barrier
- The Traditional European Bitter Aperitif
- Roasted Dandelion-Root Coffee
- Dandelion Wine and Flower Fermentation
- Functional Dyspepsia and Bloating
- Irritable Bowel Syndrome Adjunct
- Hypochlorhydria and Low Stomach Acid
- Dosage and "Bitter Before Meals" Protocol
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Taraxacin Bitter Principle
The primary bitter principle of dandelion is taraxacin (also called taraxinic acid 1'-O-beta-D-glucopyranoside), a sesquiterpene lactone concentrated in the latex (milky sap) of the plant. Sesquiterpene lactones are a chemical class of plant defense compounds known for intense bitterness, found in many of the medicinally bitter Asteraceae (daisy family) herbs — including chamomile, feverfew, artichoke, chicory, wormwood, and yarrow.
Other related bitter compounds in dandelion include taraxacerin, lactucin, lactucopicrin, and 11β,13-dihydrolactucin. The bitterness intensity varies with the plant part: the latex of the broken stem is the most intensely bitter, the leaf is moderately bitter (more so before the plant flowers), and the root is the least bitter but still distinctly so when prepared as a tincture or strong tea. Roasting the root caramelizes some sugars and softens the bitterness considerably — this is why roasted dandelion-root tea has a much more palatable, coffee-like flavor than fresh-root preparations.
The bitterness of taraxacin is "clean" — it activates bitter taste receptors strongly without producing the harsh, lingering, or astringent quality of some other bitters (like quassia or gentian, which can be overwhelmingly bitter). This makes dandelion one of the more clinically usable bitters: bitter enough to produce a real cephalic-phase response, but not so unpleasant that patients refuse to take it.
The Cephalic Phase of Digestion
Digestion is conventionally divided into three phases:
- Cephalic phase — before food enters the gut, triggered by the sight, smell, taste, or even the anticipation of food. Mediated by the vagus nerve, originating in the brain (the "cephalic" part referring to the head).
- Gastric phase — once food is in the stomach, triggered by stomach distention and by the chemical contents of the meal. Mediated by both local nervous reflexes within the stomach wall and by hormones like gastrin.
- Intestinal phase — once chyme enters the small intestine, triggered by chemical and mechanical stimuli in the duodenum. Mediated by hormones including cholecystokinin (CCK), secretin, and gastric inhibitory polypeptide (GIP).
The cephalic phase has historically been underappreciated in medical training. Pavlov's classical experiments with dogs (the salivation in response to a bell predicting food) established the cephalic phase, but the clinical implications were rarely emphasized until the modern interest in mindful eating, vagal tone, and functional digestive disorders revived interest.
Quantitatively, the cephalic phase accounts for approximately 30% of total digestive secretion in a healthy meal eaten under normal conditions (relaxed, attentive to the food, not rushed or stressed). When the cephalic phase is intact, the rest of digestion proceeds smoothly. When the cephalic phase is suppressed (eating while distracted, while stressed, while rushing, or while consuming food with no bitter component to stimulate the reflex), the gastric and intestinal phases must compensate without the upstream preparation, often resulting in the postprandial bloating, sluggish digestion, and "I just ate but I'm still not satisfied" sensation that characterize modern functional digestive complaints.
The clinical relevance of bitter herbs like dandelion: they restore the cephalic phase that the modern diet and eating pattern have weakened. A few drops of dandelion tincture in a small glass of water, taken 15-20 minutes before a meal, produces a noticeable bitter sensation on the tongue, triggers the cephalic reflex, and primes the digestive cascade. The downstream effects — better digestion, less bloating, more sense of satisfaction after meals, improved bowel regularity — are often apparent within 3-7 days of starting the practice.
The Tongue-to-Gut Vagal Reflex
The molecular and neural anatomy of the bitter reflex is now well-mapped. The pathway:
- Bitter compound binds tongue receptors — taraxacin (and other dandelion sesquiterpene lactones) binds to multiple members of the TAS2R bitter taste receptor family expressed on type II taste cells in taste buds across the tongue, with particular concentration in the posterior tongue and back wall of the pharynx. Humans have approximately 25 different TAS2R genes; different bitter compounds bind different combinations of receptors.
- Signal transduction in the taste cell — TAS2R receptors are G-protein-coupled receptors (GPCRs) signaling through the alpha-gustducin / phospholipase C beta 2 / IP3 / calcium release pathway. The calcium signal opens the TRPM5 ion channel, depolarizing the taste cell.
- Neurotransmitter release — the depolarized type II taste cell releases ATP onto type III taste cells and onto the afferent terminals of the chorda tympani nerve (anterior tongue), the glossopharyngeal nerve (posterior tongue), and the vagus nerve (pharynx and laryngeal region).
- Signal to brainstem — the gustatory afferent signal travels via these three cranial nerves to the nucleus of the solitary tract (NTS) in the medulla oblongata. The NTS is the central integration site for taste, visceral, and cardiovascular afferents.
- Efferent vagal output — the NTS triggers parasympathetic efferent output via the dorsal motor nucleus of the vagus nerve, which sends efferent signals back down to the salivary glands, stomach, pancreas, liver, gallbladder, and proximal small intestine.
- Downstream digestive secretion — the parasympathetic signal triggers:
- Salivation from parotid, submandibular, and sublingual glands — rich in alpha-amylase, lingual lipase, lysozyme, and bicarbonate
- Gastric acid secretion from parietal cells via acetylcholine release at the M3 muscarinic receptor
- Pancreatic exocrine secretion via acetylcholine and indirect CCK release — amylase, lipase, and proenzyme proteases
- Gallbladder contraction with bile release via CCK
- Increased gastric motility and stomach emptying
- Activation of intestinal motility and Migrating Motor Complex
Interestingly, TAS2R bitter receptors are not only expressed on the tongue. They are also expressed on enteroendocrine cells lining the gut, on smooth muscle cells in the airways, on sinus epithelium, and on immune cells. Some of the downstream effects of bitter herbs may be mediated through these "ectopic" bitter receptors, particularly in the gut where direct contact of swallowed bitter compounds with TAS2R-expressing enteroendocrine cells can stimulate local hormone release including GLP-1, PYY, and CCK independent of the tongue-mediated reflex.
This is why bitter herbs work somewhat even when delivered in capsules that bypass the tongue (though less powerfully than tinctures, sprays, or fresh herbs that engage the tongue). The capsule route activates the gut TAS2R pathway only; the tincture or fresh-herb route activates both the gut and the tongue pathways and produces the full cephalic-phase response.
Inulin: The Prebiotic Fiber in Dandelion Root
The second major digestive mechanism of dandelion is the inulin content of the root. Inulin is a fructan polysaccharide — a chain of fructose units linked together with a terminal glucose, ranging from 2 to 60 units long. Humans do not produce any enzyme capable of digesting fructans; they pass undigested through the stomach and small intestine to reach the colon, where colonic bacteria selectively ferment them.
Dandelion root is one of the richest natural sources of inulin in the plant kingdom. The inulin content varies with season and the age of the plant:
- First-year root, autumn-harvested: 20-40% inulin by dry weight, the peak storage period
- First-year root, spring-harvested: 10-20% inulin, after the plant has used winter stores
- Second-year root, autumn: 15-25% inulin
- Second-year root, spring: 5-15% inulin
For comparison, chicory root (the most concentrated commercial source of inulin) is approximately 40-60% inulin by dry weight; Jerusalem artichoke tubers are approximately 15-20% inulin; garlic is approximately 11% inulin; onions are approximately 2-6% inulin; bananas are approximately 0.5% inulin. Dandelion root is in the same league as the dedicated inulin-source plants and is far richer than the inulin content of common dietary vegetables.
Inulin is one of the best-characterized "prebiotic" substrates — meaning it selectively feeds beneficial gut bacteria without feeding the less desirable ones. The dominant beneficiaries are members of the genus Bifidobacterium, which express the fructofuranosidase enzymes needed to hydrolyze inulin and use the released fructose for growth. Bifidobacterium species are widely considered beneficial members of the gut microbiome, associated with reduced inflammation, improved bowel regularity, reduced risk of colon cancer, and improved metabolic markers.
The bifidogenic effect of dandelion-root inulin has been demonstrated in both in-vitro fermentation studies and in animal feeding studies. The magnitude of effect is comparable to that of equivalent doses of chicory inulin, the gold-standard prebiotic substrate. The bifidogenic effect is one of the mechanistically best-supported benefits of long-term daily dandelion-root tea consumption.
Short-Chain Fatty Acids and Gut Barrier
When bifidobacteria and other colonic microbes ferment inulin, the primary metabolic products are short-chain fatty acids (SCFAs) — principally acetate, propionate, and butyrate. SCFAs are not waste products; they are biologically active signaling molecules and energy sources with substantial physiological effects on the host:
- Butyrate — the preferred energy source for colonocytes (the epithelial cells lining the colon). A colon adequately supplied with butyrate maintains barrier integrity, low-level local immune activation, and normal cell turnover. Butyrate also has systemic effects on inflammation, insulin sensitivity, and even on the central nervous system through gut-brain axis signaling.
- Propionate — partly metabolized by colonocytes, partly absorbed into the portal circulation. Propionate reaches the liver and modulates hepatic lipid and glucose metabolism, generally favorably. It also has appetite-modulating effects through gut-derived satiety signaling.
- Acetate — the most abundant SCFA produced. Largely absorbed into the systemic circulation where it serves as an energy substrate for peripheral tissues and as a signaling molecule for adipose tissue, muscle, and brain.
The SCFA-driven benefits of inulin fermentation include:
- Improved colonic barrier integrity (reduced "leaky gut" / intestinal permeability)
- Reduced colonic inflammation
- Improved bowel regularity (SCFA stimulate normal peristalsis)
- Reduced systemic inflammatory markers (CRP, TNF-alpha)
- Modest improvement in glucose tolerance and insulin sensitivity
- Modest reduction in total and LDL cholesterol
- Reduced risk of colorectal cancer (epidemiologic association)
The connection from dandelion root tea to these systemic effects is: dandelion root tea provides inulin, inulin is fermented by bifidobacteria, the fermentation produces SCFAs, and SCFAs provide the metabolic and inflammatory benefits. The chain is mechanistically clean; the magnitude of effect from any individual dietary source of inulin depends on the dose and on the individual's baseline microbiome composition.
The Traditional European Bitter Aperitif
The European cultural tradition of taking a small bitter alcoholic beverage before meals — the "aperitif" tradition — is one of the few surviving practical applications of bitter-herb digestive support in everyday Western culture. The tradition crosses national boundaries: Italy has Campari, Aperol, Fernet, Cynar (artichoke-based) and the bitter Amari category; France has Suze, Salers, Lillet, and the various Vermouths; Germany has Underberg and the herbal liqueur category broadly; Hungary has Unicum.
The aperitif tradition originated as a digestive practice. A small (1-2 oz / 30-60 mL) glass of a bitter herbal liqueur, sipped slowly over 10-20 minutes before a meal, would coat the tongue with bitter compounds, trigger the cephalic-phase reflex discussed above, and prepare the digestive system for the meal to come. The dilution in a small amount of carbonated water (the classic Negroni or Aperol Spritz preparation) preserved the bitter exposure while making the drink palatable.
Dandelion-leaf tincture, taken 15-20 minutes before meals in a small glass of water or sparkling water, replicates the same physiologic effect of the traditional aperitif without the alcohol. Some integrative formulations combine dandelion with other digestive bitters (gentian, artichoke leaf, chicory root, orange peel, angelica root) to produce a more complex bitter profile similar to the classical aperitif herbs. The Swedish Bitters formulation (which contains dandelion, gentian, angelica, rhubarb, aloe, myrrh, and several other bitter herbs) is the most widely available commercial bitter tincture in the integrative-medicine tradition.
The practical adoption of the aperitif practice has been one of the most effective single interventions for patients with functional dyspepsia, post-meal bloating, and reduced appetite. The effect typically becomes apparent within 3-7 days of starting daily pre-meal bitters, with continued improvement over several weeks of consistent use.
Roasted Dandelion-Root Coffee
One of the most pleasant whole-food forms of dandelion for daily long-term use is roasted dandelion-root coffee. The preparation has a long tradition in Europe and North America, particularly during periods of coffee scarcity (the Napoleonic Wars, the World Wars, the American Civil War's southern blockade) when roasted root substitutes filled the gap left by unavailable coffee beans.
The preparation: clean autumn-harvested dandelion roots are chopped into small pieces, dried, then roasted in a slow oven (around 200°F / 95°C) until they turn dark brown and develop a rich coffee-like aroma. The roasted root is ground (in a coffee grinder is fine) and brewed in the same way as ground coffee — either by drip, French press, percolator, or simmered briefly in water and then strained.
The flavor: similar to coffee but milder, with a distinct earthy, slightly sweet, slightly bitter quality. Drinkers describe it as a cross between coffee and chicory-and-coffee (the New Orleans-style coffee blend uses roasted chicory root, which is botanically close to dandelion). The roasting process caramelizes the inulin and develops Maillard-reaction products (the same browning reaction that gives roasted coffee its flavor profile), so the final brewed beverage has substantially less raw bitterness than fresh dandelion root preparations.
Benefits relative to coffee:
- No caffeine, suitable for evening drinking or for people who don't tolerate caffeine well
- Retains the prebiotic inulin (though roasting partly depolymerizes it)
- Retains hepatobiliary and bitter-reflex effects, though somewhat reduced by roasting
- No tannin-related interactions with iron absorption (an issue with regular black coffee at meals)
- Generally gentler on the stomach for people with gastritis or reflux
Drawbacks relative to coffee: no caffeine for those who want the stimulant effect; less intense flavor; less widely available commercially than instant coffee or whole-bean coffee.
Commercial pre-roasted dandelion-root coffee is widely available in natural food stores under brands like Teeccino (which combines roasted dandelion root with carob, chicory, and other roasted plant materials), Dandy Blend (instant; combines dandelion, chicory, beet, barley, and rye), and various single-ingredient roasted dandelion root products. Home roasting from foraged or commercial dried dandelion roots is also straightforward.
One cup of roasted dandelion-root coffee daily is a low-effort, pleasant way to incorporate dandelion's hepatobiliary and prebiotic benefits into a daily routine indefinitely.
Dandelion Wine and Flower Fermentation
Dandelion wine is one of the oldest fermented preparations of the plant, with a tradition stretching back centuries in European folk practice and Native American adoption (Ojibwe, Iroquois, and other Eastern Woodlands cultures used dandelion flowers in fermented and unfermented preparations). The wine is made from the bright yellow flower heads, ideally collected at midday on a sunny day when the flowers are fully open.
The basic process: 4-6 quarts of fresh dandelion flowers are stripped from the green calyx (the green base of the flower; if left in, the wine becomes excessively bitter). The yellow petals are steeped in boiling water for 24 hours, then strained. Sugar, lemon, orange, and wine yeast are added to the strained "tea." The mixture ferments for several weeks, is racked off the sediment, and ages for several months to a year. The finished wine is golden, lightly floral, mildly sweet, low to moderate alcohol (8-12%).
The literary fame of dandelion wine comes from Ray Bradbury's 1957 novel Dandelion Wine, which used the family ritual of making dandelion wine each summer as a metaphor for capturing the essence of childhood summers in jars to be opened in winter. The actual home-fermentation tradition is older and far more widespread than the novel's framing suggests — nearly every rural European-descended family in temperate North America had at least one elder who made dandelion wine each spring or summer.
From a strictly medicinal perspective, dandelion wine is the weakest preparation. The fermentation degrades many of the bitter sesquiterpene lactones; the dilution and the sugar content reduce the therapeutic intensity; and the alcohol content limits dosing. The wine's appeal is cultural and culinary rather than primarily medicinal. The most therapeutically active dandelion preparations remain the dried-leaf tea, the dried-root tea, the tinctures of leaf and root separately, and the fresh young leaves in salad.
The aperitif use of dandelion wine — a small glass before dinner — is the closest the wine comes to its medicinal antecedents, providing some of the same cephalic-phase bitter stimulation that the more concentrated bitter tinctures provide.
Functional Dyspepsia and Bloating
Functional dyspepsia — persistent or recurrent upper abdominal discomfort, early satiety, postprandial fullness, or epigastric pain in the absence of an identifiable structural cause — affects approximately 10-15% of adults in developed countries. The Rome IV diagnostic criteria divide it into postprandial distress syndrome (PDS, dominated by fullness and early satiety) and epigastric pain syndrome (EPS, dominated by burning or pain). Both subtypes are commonly comorbid with irritable bowel syndrome and with reflux disease.
Pharmaceutical management options are limited and only modestly effective. Acid-suppression with proton pump inhibitors (omeprazole, esomeprazole) helps the EPS subtype somewhat. Prokinetic agents (metoclopramide, domperidone outside the US) help the PDS subtype somewhat but have side-effect profiles that limit long-term use. The newer cyclic 5-HT4 agonists (prucalopride) have shown modest benefit in some studies.
Dandelion fits well as an adjunctive support for functional dyspepsia, particularly the postprandial distress subtype where the bitter-mediated cephalic phase enhancement directly addresses the underlying functional deficit. Typical regimen: 2-5 mL of dandelion root tincture (or combined dandelion + gentian + artichoke leaf tincture) in a small glass of water, 15-20 minutes before each main meal. Effect typically becomes noticeable within 7-14 days, with continued improvement over 8-12 weeks.
The German Commission E monograph specifically lists "dyspeptic complaints" as an approved indication for dandelion. The European Medicines Agency monograph likewise lists "mild digestive disorders such as feeling of abdominal fullness, flatulence and slow digestion" as an approved indication. The European regulatory acceptance of this indication is well-established.
Irritable Bowel Syndrome Adjunct
Irritable bowel syndrome (IBS) is a related functional gastrointestinal disorder, characterized by recurrent abdominal pain associated with defecation or with change in bowel habit, in the absence of identifiable structural disease. It affects approximately 10-15% of adults globally. Management is largely empirical: low-FODMAP diet, soluble fiber, antispasmodics, probiotics, neuromodulators (low-dose tricyclic antidepressants for IBS-D, SSRIs for IBS-C), and patient education about the functional nature of the condition.
Dandelion's role in IBS management is adjunctive and somewhat nuanced. For constipation-predominant IBS (IBS-C), dandelion root inulin can contribute to improved bowel regularity through the prebiotic and SCFA mechanisms, and dandelion's bile-flow stimulation can help with the sluggish digestion that often accompanies IBS-C. For diarrhea-predominant IBS (IBS-D), however, dandelion inulin can sometimes worsen symptoms — some IBS patients have a small-intestinal bacterial overgrowth (SIBO) component, and rapid fermentation of inulin in the small intestine can produce gas, bloating, and worsening of the IBS symptoms.
The clinical approach for IBS patients considering dandelion:
- Start with a small dose (2-3 g of dried root in a single daily cup of tea, or 1-2 mL of tincture twice daily)
- Monitor for 7-14 days for symptom improvement vs worsening
- If symptoms worsen (particularly bloating, abdominal pain, distension), suspect SIBO and reduce or discontinue the inulin-containing root preparations; the leaf preparations (low inulin) may still be tolerated
- If symptoms improve, continue and titrate up gradually
- If symptoms are mixed (some better, some worse), consider stool testing for SIBO via lactulose or glucose breath testing and address underlying bacterial overgrowth before re-attempting inulin-rich prebiotic therapy
For more on the SIBO consideration, see our SIBO page, which discusses prebiotic tolerance issues at length. For more on the FODMAP framework, dandelion-root inulin would be classified as a high-FODMAP food (specifically an oligosaccharide / fructan) and would be excluded during the elimination phase of a low-FODMAP trial. The dandelion leaf is FODMAP-neutral and would be allowed.
Hypochlorhydria and Low Stomach Acid
Hypochlorhydria (low stomach acid) is more common than is generally recognized, particularly in older adults, in patients on chronic proton pump inhibitor therapy, and in patients with autoimmune atrophic gastritis. Symptoms include postprandial bloating, early satiety, undigested food in stool, low B12 absorption (with associated fatigue, neurologic symptoms, or anemia), and increased susceptibility to enteric infections (low stomach acid is the first defense against swallowed pathogens).
Pharmaceutical "acid replacement" therapy with betaine HCl supplements is one option, but is somewhat awkward in practice and not appropriate for all patients. Bitter herbs that stimulate endogenous gastric acid secretion through the cephalic-phase vagal reflex are a more physiologic alternative for patients with mild hypochlorhydria not severe enough to require betaine HCl replacement.
Dandelion fits this niche. The bitter taraxacin triggers vagal stimulation of parietal cell acetylcholine release, which directly stimulates gastric H+/K+ ATPase activity and increases gastric acid output. The effect is not as powerful as betaine HCl but is more physiologic, simultaneously stimulating other digestive secretions, and is appropriate as first-line support in mild hypochlorhydria before escalation to betaine HCl replacement.
The typical protocol: 2-5 mL of dandelion tincture (root or leaf, both work; root is somewhat more bitter) in a small glass of water, 15-20 minutes before each main meal, for 4-8 weeks with symptom monitoring. If symptoms improve, continue as long-term daily practice. If symptoms do not improve or worsen, consider escalation to betaine HCl (under guidance, as inappropriate use of betaine HCl in normochlorhydric patients can cause symptomatic gastritis).
Dosage and "Bitter Before Meals" Protocol
For digestive aid applications, dandelion can be used as either root or leaf, with somewhat different emphases:
For bitter-mediated digestive stimulation (cephalic phase enhancement):
- Dandelion root tincture (1:5 in 40% alcohol) — 2-5 mL in 1-2 oz of water, 15-20 minutes before each main meal. The most concentrated bitter preparation. The form most likely to produce strong cephalic-phase effects.
- Dandelion leaf tincture (1:3 in 30% alcohol) — 2-5 mL in 1-2 oz of water, 15-20 minutes before each main meal. Somewhat less bitter than the root tincture but more diuretic.
- Fresh dandelion leaves in pre-meal salad — the most traditional whole-food form. A handful of young pre-flowering leaves as part of a salad eaten as the first course of a meal. The bitterness from chewing engages the cephalic-phase reflex.
- Combined bitter tinctures (Swedish Bitters or similar) — 2-5 mL in water before meals. The combined herbs produce a more complex bitter profile and may be more effective than single-herb dandelion tincture.
For inulin prebiotic effects:
- Roasted dandelion-root tea — 1-2 cups daily, brewed from 1-2 teaspoons (2-4 g) of dried roasted root per cup
- Dandelion-root capsules (non-roasted) — 500-1500 mg, twice daily with meals; provides higher per-dose inulin than roasted root tea
- Raw or lightly roasted dandelion root powder in smoothies — 1-2 teaspoons daily; mixes well into smoothies, oatmeal, or kefir
The "bitter before meals" protocol that produces the most reliable improvement in functional digestive complaints:
- Mix 3 mL of dandelion root tincture (or Swedish Bitters) into 2 oz of warm water
- Sip slowly over 1-2 minutes, swishing each sip in the mouth to ensure tongue contact
- Wait 15-20 minutes for the cephalic-phase reflex to peak
- Begin the meal in a relaxed, attentive manner (no phones, no screens, no rushing)
- Chew thoroughly — the mechanical and sensory experience of chewing engages and prolongs the cephalic-phase response
- Continue daily before each main meal for at least 14 days before assessing effect
The effect on functional dyspepsia and post-meal bloating is often noticeable within 7 days and reliably evident within 14 days when the protocol is followed consistently. The protocol can be continued indefinitely as a long-term digestive support practice.
Cautions
- Gallstone disease — relative contraindication. The cholagogue effect can precipitate biliary colic in patients with known gallstones. Avoid in patients with active cholecystitis.
- Active gastric ulcer — bitter herbs that stimulate gastric acid secretion can worsen active gastric or duodenal ulcer. Wait until ulcer has healed before starting bitter herbs.
- SIBO (small intestinal bacterial overgrowth) — inulin-rich root preparations can worsen SIBO symptoms. The leaf preparation is FODMAP-neutral and may be better tolerated.
- FODMAP-sensitive IBS — dandelion root inulin is a high-FODMAP fructan and should be avoided during the elimination phase of a low-FODMAP trial. Leaf preparations are FODMAP-neutral.
- Asteraceae allergy — cross-reactive with ragweed, chamomile, and other daisy-family plants. Test with small dose first.
- Pregnancy and lactation — the bitter principles cross to breast milk and can produce bitter milk that infants may reject. Avoid concentrated bitter tinctures during lactation; modest food-source use of dandelion is generally considered acceptable.
- Drug interactions — modest CYP1A2 and CYP3A4 modulation in vitro; clinical significance is uncertain but generally small. No specific high-magnitude drug interactions consistently reported.
Key Research Papers
- Trojanova I, Rada V, Kokoska L, Vlkova E (2004). The bifidogenic effect of Taraxacum officinale root. Fitoterapia. — PubMed
- Wirngo FE, Lambert MN, Jeppesen PB (2016). The physiological effects of dandelion (Taraxacum officinale) in type 2 diabetes. Review of Diabetic Studies. — PubMed
- McMullen MK, Whitehouse JM, Towell A (2015). Bitters: time for a new paradigm. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Chambers ES, Preston T, Frost G, Morrison DJ (2018). Role of gut microbiota-generated short-chain fatty acids in metabolic and cardiovascular health. Current Nutrition Reports. — PubMed
- Roberfroid M (2007). Prebiotics: the concept revisited. Journal of Nutrition. — PubMed
- Gibson GR, Roberfroid MB (1995). Dietary modulation of the human colonic microbiota: introducing the concept of prebiotics. Journal of Nutrition. — PubMed
- Bischoff-Kont I, Furst R (2021). Benefits of ginger and its constituent 6-shogaol in inhibiting inflammatory processes (parallel review — bitter herbs and digestion). Pharmaceuticals. — PubMed
- Lai PK, Roy J (2004). Antimicrobial and chemopreventive properties of herbs and spices (including dandelion). Current Medicinal Chemistry. — PubMed
- Behrens M, Meyerhof W (2011). Gustatory and extragustatory functions of mammalian taste receptors. Physiology and Behavior. — PubMed
- Schutz K, Carle R, Schieber A (2006). Taraxacum — a review on its phytochemical and pharmacological profile. Journal of Ethnopharmacology. — PubMed
- Janda K, Gutowska I, Geszke-Moritz M, Jakubczyk K (2021). The common cichory (Cichorium intybus L.) as a source of extracts with health-promoting properties. Molecules. — PubMed
- Talley NJ, Ford AC (2015). Functional dyspepsia. New England Journal of Medicine. — PubMed
PubMed Topic Searches
- PubMed: Dandelion bitter / cephalic phase
- PubMed: Dandelion root inulin prebiotic
- PubMed: TAS2R gut enteroendocrine
- PubMed: SCFA colonic fermentation
- PubMed: Functional dyspepsia bitter aperitif
- PubMed: IBS / prebiotic / FODMAP
Connections
- Dandelion Overview
- Dandelion Benefits Hub
- Dandelion Liver & Detox
- Dandelion Diuretic & Kidney
- Dandelion Antioxidant
- Ginger
- Turmeric
- Berberine
- Probiotics
- Gut Healing
- Gut-Brain Axis
- SIBO
- Bloating
- Gastroenterology
- Food
- All Herbs