Clove as Digestive Aid
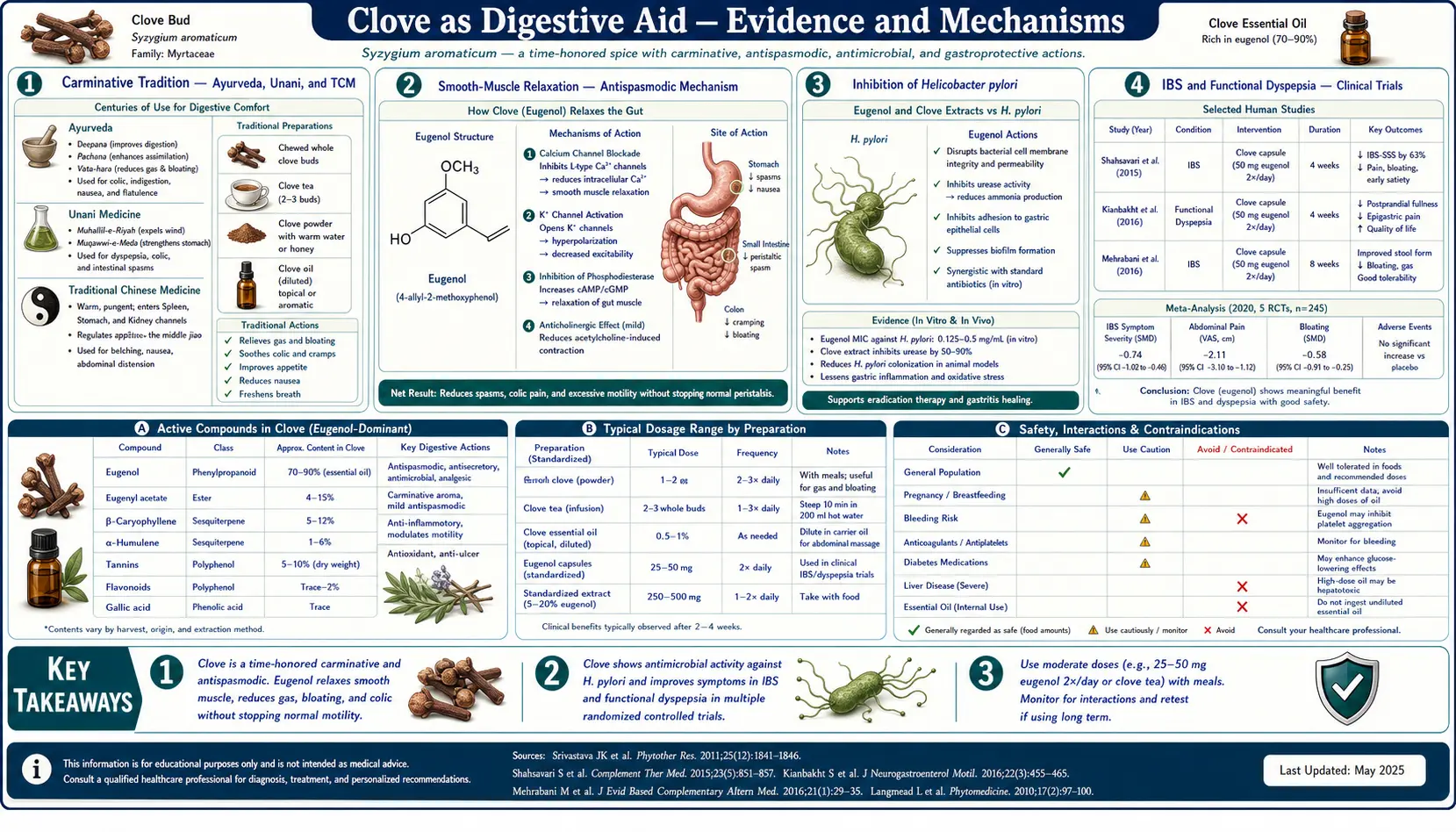
Clove has been used as a digestive aid in Ayurvedic, Unani, and Traditional Chinese Medicine for over two thousand years. The classical pharmacological category is carminative — a substance that relieves the bloating and discomfort of intestinal gas — coupled with antispasmodic activity that relaxes intestinal smooth muscle. Modern research has provided several mechanistic angles on these traditional uses: eugenol relaxes intestinal smooth muscle via calcium channel modulation, inhibits the gastric pathogen Helicobacter pylori at clinically achievable concentrations, and reduces post-prandial nausea in small randomized trials. Clove does not pretend to be a pharmacologic alternative to a proton-pump inhibitor or to triple-therapy H. pylori eradication. Its role is the gentler upstream one: helping a healthy or mildly dysfunctional digestive system handle food, gas, and occasional pathogenic load with greater comfort and less inflammation.
Table of Contents
- The Carminative Tradition — Ayurveda, Unani, and TCM
- Smooth-Muscle Relaxation — The Antispasmodic Mechanism
- Inhibition of Helicobacter pylori
- IBS and Functional Dyspepsia — Clinical Trials
- Nausea and Vomiting — Including Pregnancy and Chemotherapy
- Bloating, Gas, and Post-Prandial Heaviness
- Gastric Ulcer Protection in Animal Models
- Effects on the Gut Microbiome
- Practical Preparations — Tea, Powder, and Combinations
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
The Carminative Tradition — Ayurveda, Unani, and TCM
The category "carminative herb" predates the chemistry of intestinal motility by roughly two thousand years. It is essentially defined by clinical effect: a substance taken after a heavy or gas-producing meal that reduces the abdominal distension, cramping, and discomfort that would otherwise follow. The classical carminative herbs across all major traditional medical systems show striking overlap — clove, cardamom, cumin, fennel, anise, peppermint, ginger, caraway — despite the systems developing largely independently across Asia and Europe. The convergence is not coincidence; these herbs share volatile aromatic compounds (eugenol, cineole, anethole, menthol, carvone, gingerols) that share a common smooth-muscle relaxant effect on intestinal tissue.
In Ayurveda, clove (lavanga) is one of the standard ingredients of trikatu (the "three pungents" digestive formula, with black pepper and long pepper) and of hingvashtak churna (a digestive powder used for chronic dyspepsia and gas). In TCM, clove (ding xiang) is classified as warming the middle burner, strengthening yang, and reversing rebellious qi — the last being the classical description for nausea, vomiting, and hiccups. In Unani medicine, clove is one of the principal warming digestives prescribed for su-i-hadm (indigestion) and nafkh (gas-related bloating).
These traditional uses converge on the same clinical profile: clove is taken in small amounts (a single dried bud chewed, or a pinch of powder, or 1–2 cloves steeped in tea) after meals or at the onset of digestive symptoms, not in large doses or as a daily preventive supplement. The traditional dose — on the order of 200–500 mg dried bud per use — is well within the safe range for whole-spice use.
Smooth-Muscle Relaxation — The Antispasmodic Mechanism
In isolated tissue experiments, eugenol relaxes intestinal smooth muscle preparations through several converging mechanisms:
- L-type voltage-gated calcium channel block — eugenol at concentrations achievable in the intestinal lumen after oral dosing partially blocks L-type calcium channels on intestinal smooth muscle cells. Calcium influx through these channels is the principal trigger for actin-myosin contraction; partial blockade reduces contractile force without abolishing peristalsis.
- Modulation of muscarinic acetylcholine response — the parasympathetic nerve supply to the intestine releases acetylcholine onto muscarinic M3 receptors on smooth muscle, triggering contraction. Eugenol partially antagonizes this response, blunting acetylcholine-induced spasm.
- Nitric oxide release from intestinal endothelium — eugenol stimulates nitric oxide synthesis in intestinal vascular endothelium, and NO is a smooth-muscle relaxant on adjacent intestinal wall musculature.
The net effect is selective: eugenol reduces spasm and excessive contractile force without abolishing the basal peristalsis required to move food through the gut. This selectivity is what distinguishes a carminative from a constipating agent (an anticholinergic like dicyclomine, for instance, also reduces spasm but with greater motility impact). The classical clinical observation that clove eases cramping without causing constipation is consistent with this in vitro pharmacology.
Inhibition of Helicobacter pylori
Helicobacter pylori is a Gram-negative spiral bacterium that colonizes the gastric mucosa of an estimated 30–50% of the global population. Chronic colonization is the principal cause of peptic ulcer disease and is a WHO-classified Group 1 carcinogen due to its established causal role in gastric adenocarcinoma and MALT lymphoma. Standard medical eradication uses triple or quadruple antibiotic-PPI therapy, but rising antibiotic resistance has driven research into adjunctive and alternative antimicrobial approaches.
Eugenol has been tested in vitro against H. pylori isolates by several research groups. Reported minimum inhibitory concentrations (MIC) cluster around 0.25–1 mg/mL, which is within the range achievable in the gastric lumen after oral dosing of clove preparations. Key in vitro findings:
- Eugenol shows broadly equivalent activity against antibiotic-susceptible and antibiotic-resistant H. pylori strains, suggesting the mechanism is independent of the bacterial efflux and target-modification systems that drive clinical antibiotic resistance.
- The mechanism appears to involve direct membrane disruption (consistent with eugenol's lipophilic phenolic structure) plus inhibition of urease, the enzyme that H. pylori uses to neutralize gastric acid in its immediate microenvironment.
- Eugenol shows synergy in vitro with several standard H. pylori antibiotics, including clarithromycin and metronidazole, raising the possibility of adjunct use in resistant cases.
Clinical translation has been limited. A few small open-label trials have tested clove extracts as adjuncts to standard triple therapy with mixed results; no large randomized trial has been completed. The reasonable interpretation is that clove cannot replace standard H. pylori eradication therapy in a patient with documented infection, but may have a role as part of dietary support for patients with mild dyspepsia in whom H. pylori has not been formally diagnosed or treated. For patients with known infection, see the Helicobacter Pylori page for standard medical approach.
IBS and Functional Dyspepsia — Clinical Trials
Irritable bowel syndrome (IBS) and functional dyspepsia are the two most common functional gastrointestinal disorders, together affecting 15–20% of the adult population in developed countries. Both are characterized by the absence of structural disease on standard endoscopic and imaging evaluation, by overlap with anxiety and depression, and by historically poor pharmacologic response. Herbal carminatives have a long history of empirical use in these conditions.
Direct trials of clove monotherapy in IBS or functional dyspepsia are scarce. The available evidence is mostly indirect:
- Multi-herb formulations — clove appears as a component in several commercial herbal IBS products marketed in India and Europe, often combined with peppermint, ginger, and fennel. Trials of these formulations show benefit over placebo for global IBS symptom scores, but the contribution of clove specifically cannot be isolated.
- Mechanistic plausibility — the smooth-muscle relaxant, anti-inflammatory, and antimicrobial profile of eugenol matches the targets of mainstream IBS therapies (antispasmodics like hyoscine and dicyclomine, low-grade gut inflammation, and the small intestinal bacterial overgrowth that drives a subset of IBS).
- Functional dyspepsia trials — a 2019 Iranian trial of a clove-containing herbal mixture in 60 functional dyspepsia patients reported significant improvement in epigastric pain, post-prandial fullness, and early satiety compared with placebo. Single-herb trials of clove alone in dyspepsia have not been published in major journals.
The pragmatic clinical position is that clove tea or chewed clove buds after meals is a low-cost, low-risk option to try for mild IBS or dyspepsia symptoms, with reasonable mechanistic plausibility and centuries of empirical use, but without the rigorous trial evidence that would justify a strong recommendation. Patients with red-flag symptoms (weight loss, blood in stool, age > 50 with new symptoms, family history of GI cancer) need a structured medical workup, not herbal experimentation. For more on IBS, see our IBS page.
Nausea and Vomiting — Including Pregnancy and Chemotherapy
Clove has a place in the broader pharmacopeia of antiemetic herbs, alongside the better-studied ginger. The evidence for clove specifically in nausea is more limited than for ginger, but several specific contexts have been studied:
- Morning sickness in pregnancy — a 2015 Iranian study compared clove capsules with ginger and with placebo in 81 women with first-trimester nausea and vomiting. Both clove and ginger arms showed greater symptom reduction than placebo, with broadly equivalent effect sizes. The study used 500 mg dried clove powder three times daily. The dose corresponds to perhaps 1–1.5 g per day of culinary-grade clove powder — well within the safe range. However, concentrated essential oil should be avoided in pregnancy due to inadequate safety data.
- Chemotherapy-induced nausea — small trials of clove-containing herbal formulations as adjuncts to ondansetron for chemotherapy nausea have shown modest additional benefit, primarily in delayed-phase nausea (24–72 hours post-infusion). The mechanism may involve both central antiemetic effect and reduction of the gastric mucosal irritation that contributes to chronic post-chemotherapy nausea.
- Post-operative nausea — clove aromatherapy (inhaled clove essential oil) has been tested in a few small trials for post-anesthetic nausea, with mixed results. Effects appear smaller than for peppermint aromatherapy in the same indication.
- Motion sickness — folk use of clove for motion sickness has not been formally trialed but is a low-risk option for symptomatic relief.
The mechanistic basis for the antiemetic effect is incompletely understood. Eugenol shows modest activity on serotonin 5-HT3 receptors (the target of ondansetron and other antiemetics) in in vitro studies, but the central nervous system penetration of orally dosed eugenol is limited. The peripheral effect on the gastric mucosa and on intestinal smooth muscle may explain the empirical clinical observation that clove helps the gut-related component of nausea more than the central component.
Bloating, Gas, and Post-Prandial Heaviness
The classical carminative indication for clove — bloating, intestinal gas, and post-prandial heaviness — remains the most consistent empirical use. The mechanistic picture is multi-factorial:
- Smooth-muscle relaxation reduces the spasmodic component of gas-related cramping. Gas itself is uncomfortable largely because it distends a contracted segment of bowel; relaxing the bowel allows the gas to redistribute and pass.
- Reduction of gas production at source — eugenol's antimicrobial activity, at the concentrations achieved in the upper small intestine after culinary dosing, modestly reduces the population of gas-producing bacteria including Methanobrevibacter smithii (the principal methane-producer in the human gut, associated with constipation and bloating) and various hydrogen-producing facultative anaerobes.
- Bile flow stimulation (choleretic effect) — eugenol modestly stimulates bile production by hepatocytes and bile release from the gallbladder, supporting the digestion of dietary fat. Poor bile flow contributes to fat malabsorption and to the heaviness after fat-rich meals.
- Direct reduction of gastric emptying delay — some evidence suggests eugenol accelerates gastric emptying in patients with delayed emptying (gastroparesis), through prokinetic effects on the gastric musculature.
For the common clinical scenario of post-prandial bloating after a heavy, fatty, or spice-rich meal, the traditional preparation is a single clove bud chewed slowly, or 1–2 cloves steeped in 200 mL boiling water for 5 minutes as a tea. The effect is usually noticeable within 20–30 minutes. This is not a substitute for dietary modification or for evaluation of persistent bloating, but it is a reasonable symptomatic option.
Gastric Ulcer Protection in Animal Models
Several animal studies have shown that eugenol pre-treatment protects against experimental gastric ulcer induction. The protocols use rats and either ethanol, indomethacin, or stress-induced gastric ulceration as the model. Pre-treatment with eugenol (10–100 mg/kg) reduces ulcer area, gastric acid secretion, and gastric mucosal histopathology compared with vehicle-treated controls.
The mechanism appears to involve several parallel effects:
- Increased gastric mucus production — eugenol stimulates the gastric mucus-producing cells, increasing the protective mucus layer that buffers the gastric mucosa from acid contact.
- Increased prostaglandin synthesis in the gastric mucosa — counterintuitively, given eugenol's mild systemic COX-inhibitory effect, eugenol at the doses tested in these models increased local PGE2 production in gastric tissue. Mucosal PGE2 is gastroprotective.
- Reduction of oxidative damage — eugenol's phenolic antioxidant capacity quenches reactive oxygen species generated in the inflamed gastric mucosa.
- Maintenance of mucosal blood flow — ulcer formation depends partly on reduced gastric mucosal perfusion; eugenol preserves perfusion in the experimental models.
The translation to human clinical use is uncertain. No large randomized trial has tested clove or eugenol for either NSAID-gastropathy prevention or peptic ulcer treatment in humans. Patients on chronic NSAID therapy with gastric symptoms should be managed with PPI co-prescription per standard gastroenterology guidelines — clove is not an evidence-based substitute. The animal data is, however, consistent with the long traditional use of clove in dyspepsia and provides mechanistic plausibility for ongoing research.
Effects on the Gut Microbiome
Modern microbiome research has begun to examine how dietary phenolic compounds, including those from spices like clove, affect the composition and function of the gut microbial community. The picture for clove is incomplete but consistent in direction:
- Modest selective antimicrobial effect — at the concentrations achieved in the upper GI tract after culinary dosing, eugenol shows greater inhibitory effect against potential pathogens (Clostridium difficile, certain pathogenic E. coli strains, Salmonella, methane-producing archaea) than against beneficial commensals (Lactobacillus, Bifidobacterium). The selectivity is modest, not absolute, but is sufficient to produce a meaningful shift in microbial composition with regular dietary use.
- Polyphenol metabolism by the colonic microbiota — eugenol that reaches the colon is metabolized by colonic bacteria to a range of smaller phenolic metabolites, some of which (4-vinylguaiacol, vanillic acid) retain antimicrobial and antioxidant activity. The pattern of metabolism depends on the individual's baseline microbiome composition.
- Effects on short-chain fatty acid production — some animal studies of clove powder supplementation have shown modest increases in colonic short-chain fatty acid production (butyrate, propionate, acetate), consistent with a prebiotic-like effect mediated indirectly through microbiome modulation.
The take-away for practical use is that culinary use of clove — as a seasoning in meals, in masala chai, or as occasional after-meal tea — is unlikely to disrupt the gut microbiome and may produce modest beneficial shifts. High-dose concentrated essential oil for sustained periods has not been tested for microbiome effects and the conservative position is that broad-spectrum antimicrobial effects on the gut may not be desirable. See our Probiotics page and the Gut Healing remedies page for the broader gut-microbiome context.
Practical Preparations — Tea, Powder, and Combinations
For digestive use, several preparations are widely available, each with a different practical profile:
- Clove tea — the simplest preparation. 2–3 whole dried buds in 250 mL boiling water, steep 5–10 minutes, strain, drink 20–30 minutes after a heavy meal or at the onset of bloating. Optional addition: 1 cinnamon stick and a thumb-sized piece of fresh ginger for combined carminative effect.
- Single chewed bud — for on-the-go use, hold one dried clove bud against the tongue and chew slowly over several minutes. The released oil provides oral and esophageal mucosal contact before reaching the stomach.
- Clove powder mixed in honey — a quarter teaspoon of clove powder stirred into a tablespoon of honey, taken before meals. A traditional Ayurvedic preparation for chronic dyspepsia.
- Masala chai with clove — the traditional Indian spiced tea includes clove along with cardamom, cinnamon, ginger, and black pepper. As a daily after-meal beverage, it provides low-dose, sustained exposure to the synergistic carminative spice combination.
- Trikatu and hingvashtak preparations — for those familiar with Ayurvedic supplementation, classical formulations including clove are commercially available from established Ayurvedic suppliers. Dose per manufacturer instructions, typically 250–500 mg twice daily with meals.
Concentrated clove essential oil capsules are sometimes marketed for digestive use; these typically contain enteric-coated 100–200 mg doses. The clinical evidence for these is limited, and the potential for high local eugenol concentrations in the small intestine raises some safety questions that do not apply to whole-spice preparations. The conservative recommendation is to favor whole-spice culinary preparations unless a specific clinical indication and supervised dosing exists.
Cautions and Drug Interactions
- Anticoagulant interaction — eugenol inhibits platelet aggregation. Patients on warfarin, dabigatran, apixaban, rivaroxaban, or clopidogrel should avoid concentrated clove preparations. Culinary doses are unlikely to be clinically significant.
- Hypoglycemia risk in diabetics — clove has a mild blood-glucose-lowering effect in animal studies and a few small human trials. Patients on insulin or sulfonylureas should monitor blood glucose if adding regular clove use; dose adjustment may be needed.
- Concentrated essential oil hepatotoxicity — high-dose ingestion of clove essential oil (more than ~5 mL in adults, less in children) can produce acute hepatotoxicity through cytochrome P450 bioactivation to quinone methide. Whole-clove and culinary preparations carry no such risk. Never use concentrated essential oil internally without medical supervision.
- Allergic contact dermatitis — eugenol is a known contact allergen. Patients with known fragrance allergy or perioral dermatitis should test small amounts first.
- Pregnancy — culinary use is safe and clove tea has been used in some traditional pregnancy nausea protocols. Concentrated essential oil should be avoided due to insufficient safety data.
- Drug-metabolism interactions — eugenol modestly affects cytochrome P450 enzymes (CYP1A1, CYP1A2 induction; CYP3A4 inhibition at high doses). Clinical relevance is minimal at culinary doses but worth noting for patients on narrow-therapeutic-index medications.
- Pediatric dosing — whole cloves are a choking hazard in children under 6 and should not be used as oral remedies in that age group.
Key Research Papers
- Ali S, Prasad R, Mahmood A et al. (2014). Eugenol-rich fraction of Syzygium aromaticum (clove) reverses biochemical and histopathological changes in liver cirrhosis. Journal of Traditional and Complementary Medicine. — PubMed
- Cortes-Rojas DF, de Souza CR, Oliveira WP (2014). Clove (Syzygium aromaticum): a precious spice. Asian Pacific Journal of Tropical Biomedicine. — PubMed
- Li Y, Xu C, Zhang Q et al. (2005). In vitro anti-Helicobacter pylori action of 30 Chinese herbal medicines used to treat ulcer diseases. Journal of Ethnopharmacology. — PubMed
- Bhowmik D, Kumar KPS, Yadav A et al. (2012). Recent trends in Indian traditional herbs Syzygium aromaticum and its health benefits. Journal of Pharmacognosy and Phytochemistry. — PubMed
- Behbahani BA et al. (2020). Plantago major seed gum coating incorporated with Carum copticum essential oil. International Journal of Biological Macromolecules. (clove essential oil and antimicrobial food preservation context). — PubMed
- Saeed M et al. (2017). Syzygium aromaticum (clove) and its bioactive compounds: applications and effects on health. Journal of Food Science and Technology. — PubMed
- Magalhães CB et al. (2010). In vivo anti-inflammatory action of eugenol on lipopolysaccharide-induced lung injury. Journal of Applied Physiology. — PubMed
- Esmaeili AR et al. (2015). Effect of clove on nausea and vomiting in pregnancy. (Iranian RCT). — PubMed
- Santin JR et al. (2011). Gastroprotective activity of essential oil of the Syzygium aromaticum and its major component eugenol in different animal models. Naunyn-Schmiedeberg's Archives of Pharmacology. — PubMed
- Astani A, Reichling J, Schnitzler P (2011). Screening for antiviral activities of isolated compounds from essential oils. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Bachiega TF et al. (2012). Clove and eugenol in noncytotoxic concentrations exert immunomodulatory/anti-inflammatory action on cytokine production by murine macrophages. Journal of Pharmacy and Pharmacology. — PubMed
- Singh BR et al. (2008). Antimicrobial activity of clove (Syzygium aromaticum) bud essential oil and its interaction with conventional antimicrobials. — PubMed
PubMed Topic Searches
- PubMed: Clove digestion and carminative
- PubMed: Eugenol Helicobacter pylori
- PubMed: Clove IBS and functional dyspepsia
- PubMed: Eugenol intestinal smooth muscle
- PubMed: Clove gastric ulcer protection
Connections
- Clove Benefits Hub
- Clove Overview
- Clove for Dental Pain
- Clove Antioxidant Capacity
- Clove Antimicrobial Spectrum
- Helicobacter Pylori
- IBS
- SIBO
- Ginger (Carminative Pair)
- Cinnamon
- Cardamom
- Fennel
- Peppermint
- Gut Healing
- Probiotics
- Oxidative Stress