Chanca Piedra for Kidney Stones
Chanca Piedra's English name is a literal translation of the Spanish — "stone breaker." Centuries of Amazonian and Andean folk use anticipated what modern pharmacology has refined: the herb does not literally dissolve mature stones, but it does measurably reduce crystal formation, change crystal shape so fragments pass more easily, and assist clearance after shock-wave lithotripsy (SWL). This page covers the patient-facing protocol — the evidence, the dosing, when it works, and where it doesn't.
Table of Contents
- The "Stone Breaker" Name
- What Chanca Piedra Actually Does
- Calcium Oxalate Stones (~80% of cases)
- Uric Acid Stones
- Cystine and Struvite Stones
- The Nishiura 2004 Trial
- Micali 2006: Post-SWL Fragment Passage
- Urinary Chemistry Effects
- Dosing Protocols
- Chanca Piedra vs Standard Prevention
- Evidence Quality
- Key Research Papers
- Connections
- Featured Videos
The "Stone Breaker" Name
Two languages, same translation. Quebra pedra in Portuguese (Brazilian Amazon) and chanca piedra in Spanish (Andean and Peruvian) both literally mean "stone breaker." The name is centuries old in indigenous Amazonian and Andean traditional medicine, where Phyllanthus niruri was prepared as a tea or decoction for "kidney pain" and the passage of stones in the urine. Modern pharmacological investigation began in the 1980s and 1990s at the Federal University of São Paulo (UNIFESP) under Nicolaos Barros and Ita Pfeferman Heilberg, who built the experimental framework that explained how a folk remedy actually worked.
What Chanca Piedra Actually Does
The traditional name oversells the mechanism. Chanca Piedra is not literally a stone-dissolving solvent. The substantiated effects are subtler and arguably more useful as a long-term strategy:
- Anti-crystallization — reduces the rate at which calcium oxalate ions cluster into stone-forming crystals in supersaturated urine
- Anti-aggregation — prevents small crystals from sticking together into larger, harder-to-pass stones
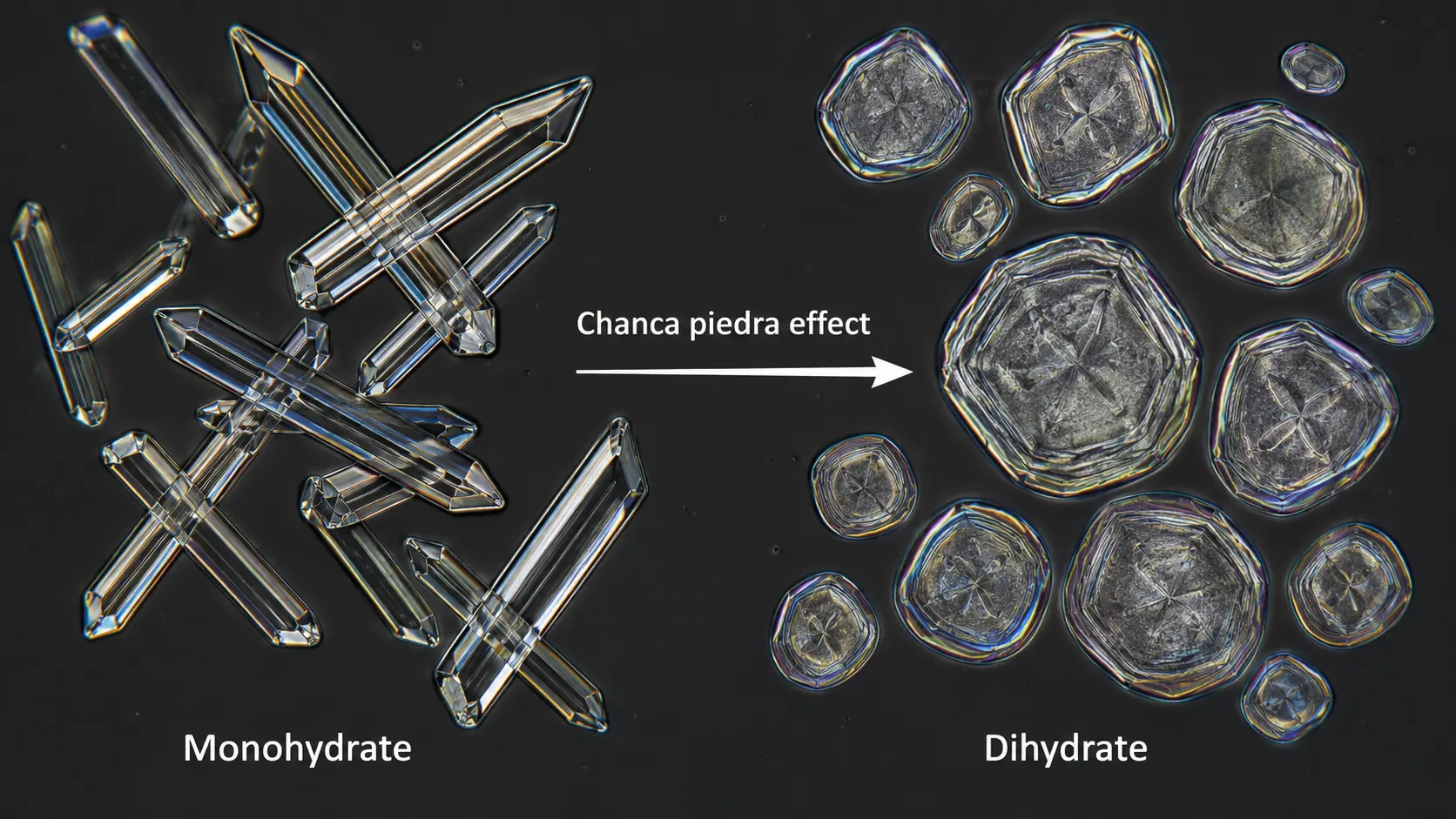
- Crystal-shape modification — shifts the crystal habit from sharp-edged calcium oxalate monohydrate (COM) toward rounder calcium oxalate dihydrate (COD), which slides through the ureter more easily
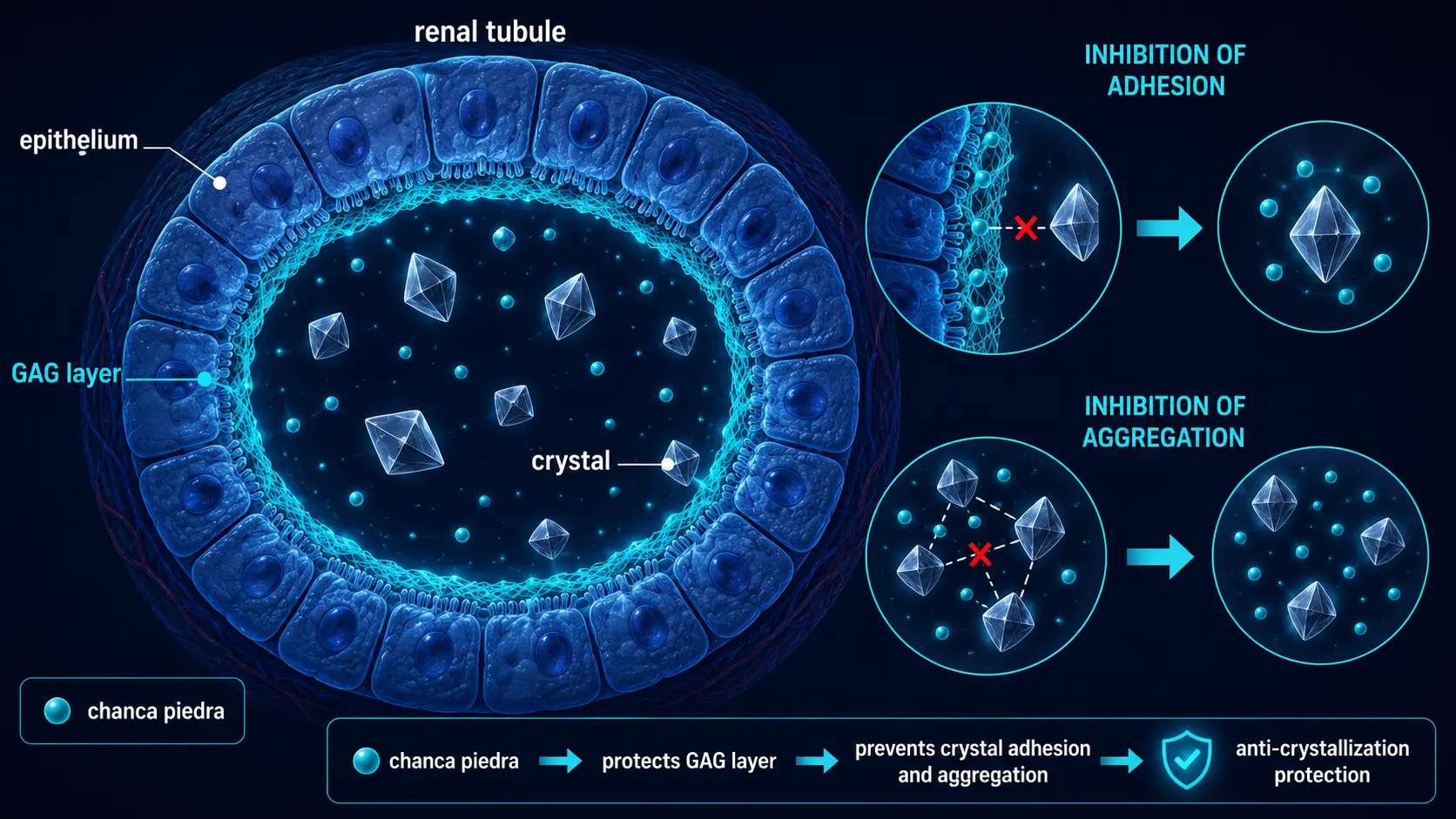
- Reduced epithelial adhesion — disrupts the glycosaminoglycan binding that lets crystals stick to renal tubular cells (the first step in stone growth)
- Reduced internal calcification — existing stones become more friable (less dense, more crumble-prone), improving fragment passage after SWL
The Barros 2003 rat experiments at UNIFESP established the anti-adherence mechanism by showing that Chanca Piedra-treated tubular cells had significantly less calcium oxalate crystal binding. That single mechanism explains most of the downstream clinical observations.
Calcium Oxalate Stones (~80% of cases)
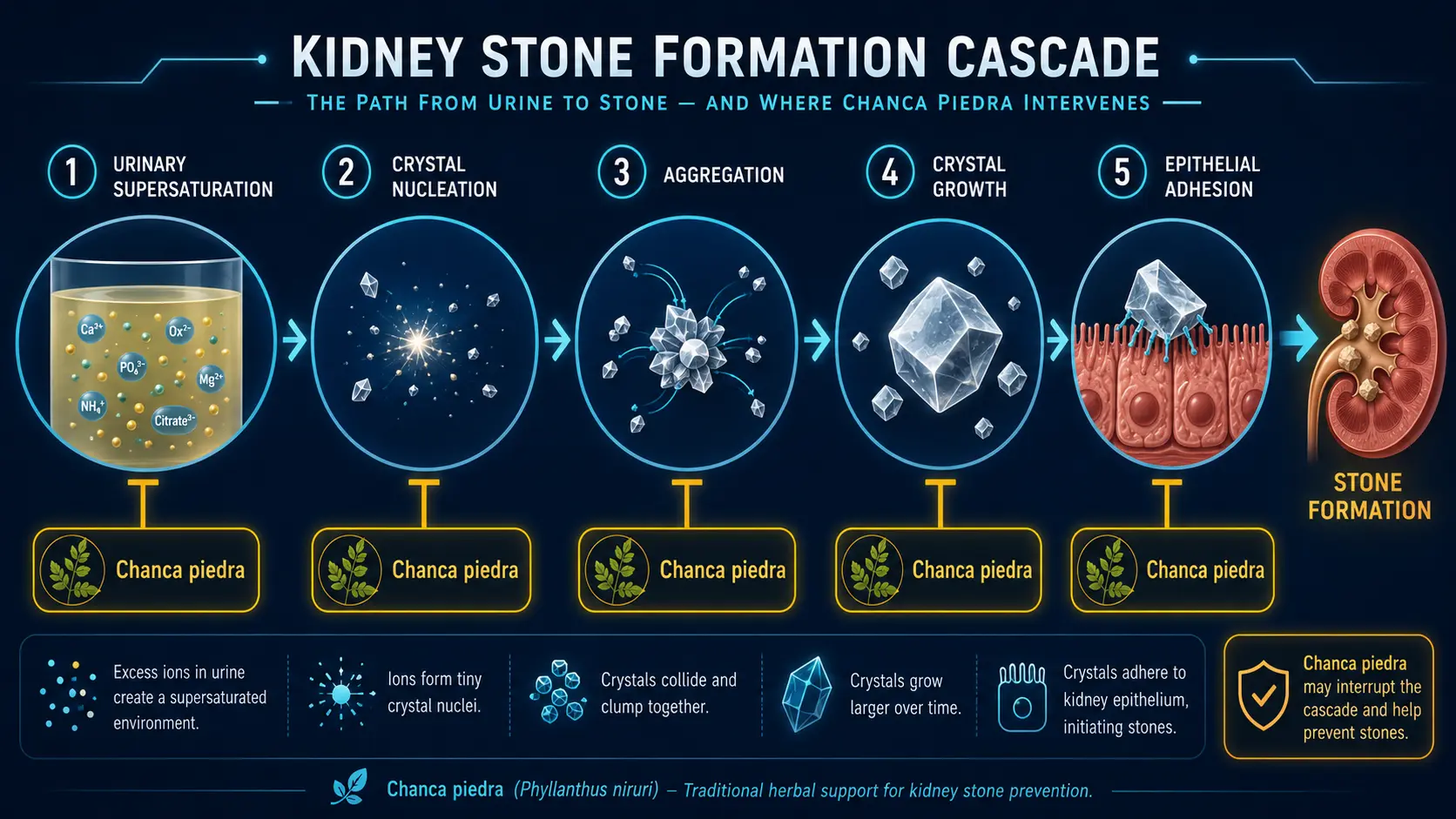
Calcium oxalate stones are by far the most common — about 80% of all kidney stones in the US. They form when urine becomes supersaturated with calcium and oxalate, when crystals nucleate in the renal collecting system, when those crystals stick to the tubular epithelium, and when more crystals layer onto the seed.
Chanca Piedra interrupts this cascade at multiple points. The Nishiura 2004 trial measured urinary chemistry changes in 56 idiopathic calcium oxalate stone formers given 450 mg of dried Phyllanthus niruri extract three times daily for three months. The hypercalciuric subgroup (those whose urine carried excess calcium) showed significant reduction in urinary calcium — the principal driver of new stone formation. The overall stone-promoting profile of the urine improved without any reported adverse effects.
For a calcium oxalate stone-former, the practical implication is that Chanca Piedra is a reasonable adjunct to mainstream prevention (high fluid intake, dietary moderation of oxalate-rich foods like spinach and almonds, dietary calcium kept normal rather than restricted, salt and animal-protein moderation) for slowing or preventing new stone growth. It is not a replacement for these foundations.
Uric Acid Stones
Uric acid stones account for about 10% of all kidney stones and are particularly common in patients with gout, metabolic syndrome, persistent low urine pH, or chronic diarrhea (which can produce acidic urine through bicarbonate loss). Uric acid is much more soluble at urinary pH above 6.5; below pH 5.5 it crystallizes.
Animal data and small human studies suggest Chanca Piedra has modest uricosuric (urate-excreting) and alkalinizing effects, lowering serum uric acid while raising urinary pH toward the soluble range. The mechanism is less well-characterized than the calcium oxalate effects, but is consistent with the xanthine oxidase inhibition documented in pharmacology studies (see Uric Acid & Gout).
For uric acid stone formers, Chanca Piedra is a reasonable adjunct to potassium citrate or sodium bicarbonate, which remain the primary alkalinizing therapies, and to allopurinol or febuxostat, which directly lower serum urate.
Cystine and Struvite Stones
The honest answer for these less-common stone types: there is essentially no high-quality human data supporting Chanca Piedra. A few in-vitro studies suggest reduced struvite crystal nucleation in urinary-tract-infection models (struvite stones form in alkaline urine in the presence of urease-producing bacteria like Proteus). Cystinuria response to Chanca Piedra is anecdotal and absent from any randomized trial literature.
If you have cystine or struvite stones, the standard treatments — tiopronin or D-penicillamine for cystine, plus aggressive hydration and pH control; antibiotics plus surgical clearance for struvite — are not optional. Chanca Piedra at most plays an adjunctive role and should not delay definitive management.
The Nishiura 2004 Trial
The single most-cited human study. Nishiura et al. (UNIFESP, São Paulo), published in Urological Research:
- Design: Open-label, 56 idiopathic calcium oxalate stone formers
- Intervention: 450 mg dried Phyllanthus niruri extract, three times daily, for three months
- Outcomes: 24-hour urine calcium, oxalate, citrate, magnesium, pH
- Findings: Hypercalciuric subgroup (n=22 with baseline urinary calcium > 200 mg/24h) showed significant reduction in urinary calcium. Overall stone-promoting urinary profile improved. No adverse effects reported.
Nishiura is the cleanest human study of Chanca Piedra for stone prevention. Its limits: open-label, no placebo arm, single center, modest sample size, three-month duration only. The mechanism it confirms (hypercalciuria reduction) is biologically plausible and consistent with the rat-model data from Barros.
Micali 2006: Post-SWL Fragment Passage
The strongest evidence for Chanca Piedra in actual stone-passage clinical practice. Micali et al. (Italy), published in The Journal of Urology:
- Design: 150 patients undergoing extracorporeal shock-wave lithotripsy (ESWL) for lower-pole renal stones
- Intervention: 2 g/day Phyllanthus niruri for three months post-ESWL vs no adjuvant
- Outcomes: Stone-free rates at three months
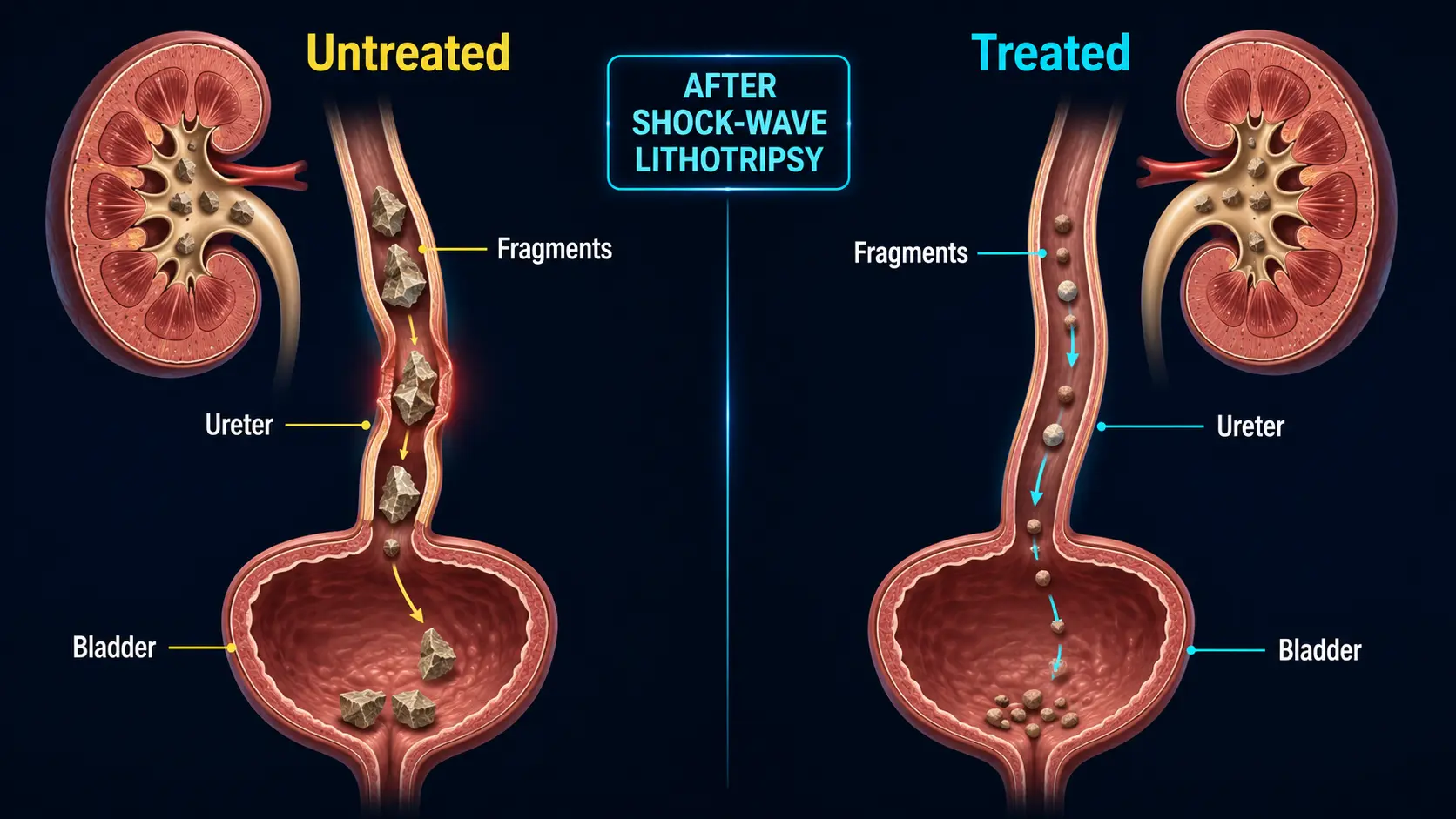
- Findings: Stone-free rates improved from approximately 70% to approximately 94% in the lower calyx (the part of the kidney where fragments often get stuck because of unfavorable anatomy)
This is the use case with the strongest evidence: after a urologist has fragmented your stones with shock waves, Chanca Piedra at 2 g/day for three months helps the fragments make their way out. The 24-percentage-point improvement in stone-free rate is clinically meaningful.
The Pucci 2018 review/meta-analysis (International Brazilian Journal of Urology) confirmed the post-SWL adjuvant signal across multiple smaller trials, while flagging the heterogeneity and small sample sizes that limit strong conclusions.
Urinary Chemistry Effects
From the Nishiura trial and supporting studies, the documented urinary chemistry effects:
- Calcium: reduced in hypercalciuric patients (significant); no change in normocalciuric patients
- Oxalate: no consistent change
- Citrate: variable; some studies show modest increase, which is favorable for stone prevention
- Magnesium: minimal change
- pH: mild alkalinization in some cohorts — favorable for uric acid stone prevention, neutral or mildly favorable for calcium oxalate
None of these are dramatic. Chanca Piedra is a tilt-the-scales intervention, not a transformation. For perspective: a thiazide diuretic typically reduces 24-hour urinary calcium by 25–50%; Chanca Piedra's effect in the hypercalciuric subgroup of Nishiura was in the 10–20% range.
Dosing Protocols
Three patient-facing protocols supported by the trial data:
Post-SWL fragment-passage adjuvant
- Dose: 2 g/day of dried herb (typically as standardized extract capsules)
- Duration: 12 weeks after the procedure
- Pair with: high fluid intake (2.5+ L/day), follow-up imaging at 3 months, urology follow-up
Hypercalciuria prevention
- Dose: 450 mg three times daily of standardized extract (the Nishiura protocol)
- Duration: 3 months on, then re-check 24-hour urine calcium
- Pair with: dietary salt moderation, animal-protein moderation, normal-not-low dietary calcium, high fluid intake
General "stone history" maintenance
- Dose: 1–2 g/day of standardized extract (some practitioners use a 4-week-on / 1-week-off cycle)
- Duration: ongoing as part of long-term prevention
- Pair with: 2.5–3 L/day fluid (the single most important intervention), dietary moderation, periodic urology follow-up
For details on standardization, extract types, and quality criteria, see Forms, Dosing & Standardization.
Chanca Piedra vs Standard Prevention
Standard medical stone prevention has decades of Level-1 randomized-trial evidence:
- Potassium citrate 10–20 mEq three times daily — the most-studied prevention drug, particularly effective in hypocitraturic and uric acid stone formers
- Thiazide diuretics — hydrochlorothiazide 25–50 mg/day or chlorthalidone 25–50 mg/day; reduce hypercalciuria by 25–50%
- Allopurinol — for uric acid stones and hyperuricosuric calcium oxalate stones
- Hydration — 2.5+ L/day urine output is the single most effective non-pharmacologic intervention
Chanca Piedra fits as a complement to these, not a replacement. Reasonable scenarios:
- You're already on potassium citrate but want additional anti-crystallization support
- You can't tolerate potassium citrate's GI effects (stomach upset, diarrhea, hyperkalemia in CKD)
- You can't tolerate thiazide's metabolic effects (hyperuricemia, hyperglycemia, hypokalemia)
- You've just had SWL and want to maximize fragment-clearance odds
- You've had multiple episodes and want a long-term anti-crystallization adjunct
It is not a reasonable substitute for evidence-based therapy in patients with significant stone disease, recurrent stones, or genetic stone-formation syndromes (cystinuria, primary hyperoxaluria).
Evidence Quality
Well-supported:
- Anti-crystallization mechanism in vitro and in animal models
- Post-SWL fragment-passage benefit (Micali 2006 and follow-up trials)
- Reduction of hypercalciuria in idiopathic stone formers (Nishiura 2004)
- Excellent short-to-medium-term safety profile at studied doses
Plausible but preliminary:
- Uric acid stone prevention via mild alkalinization and uricosuric effects
- Citrate-promoting and pH-modifying effects
- Long-term recurrence reduction (most trials only ran 3 months)
Unsupported by evidence:
- Literal dissolution of mature kidney stones (despite the name)
- Cystine or struvite stone treatment as a primary or sole therapy
- Replacement of potassium citrate, thiazides, or allopurinol in indicated patients
- Treatment of acute renal colic (Chanca Piedra is for prevention/passage, not pain control)
Key Research Papers
- Nishiura JL, Campos AH, Boim MA, Heilberg IP, Schor N. Phyllanthus niruri normalizes elevated urinary calcium levels in calcium stone forming (CSF) patients. Urological Research, 2004 Oct;32(5):362-6. — PubMed
- Micali S, Sighinolfi MC, Celia A, et al. Can Phyllanthus niruri affect the efficacy of extracorporeal shock wave lithotripsy for renal stones? A randomized, prospective, long-term study. The Journal of Urology, 2006 Sep;176(3):1020-2. — PubMed
- Barros ME, Schor N, Boim MA. Effects of an aqueous extract from Phyllanthus niruri on calcium oxalate crystallization in vitro. Urological Research, 2003 Feb;31(1):26-31. — PubMed
- Pucci ND, Marchini GS, Mazzucchi E, et al. Effect of Phyllanthus niruri on metabolic parameters of patients with kidney stone: a perspective for disease prevention. International Brazilian Journal of Urology, 2018. — PubMed
- Freitas AM et al. The effect of Phyllanthus niruri on urinary inhibitors of calcium oxalate crystallization. BJU International. — PubMed
- Campos AH, Schor N. Phyllanthus niruri inhibits calcium oxalate endocytosis by renal tubular cells. Nephron. — PubMed
PubMed Topic Searches
- PubMed: Phyllanthus and calcium oxalate
- PubMed: Phyllanthus post-SWL adjuvant
- PubMed: Stone-prevention RCTs
- PubMed: Phyllanthus hypercalciuria
- PubMed: Uric acid stones
- PubMed: Urinary citrate & pH
Connections
- Chanca Piedra Benefits Hub
- Chanca Piedra Overview
- Liver Protection
- Uric Acid and Gout
- Blood Sugar
- Forms, Dosing and Standardization
- Active Compounds
- Safety and Drug Interactions
- Phyllanthus Species Comparison
- Kidney Stones
- Kidney Function
- Urinalysis
- Comprehensive Metabolic Panel
- Uric Acid
- Magnesium
- Potassium
- Calcium
- Gout