Yogurt — Bone Density and Calcium
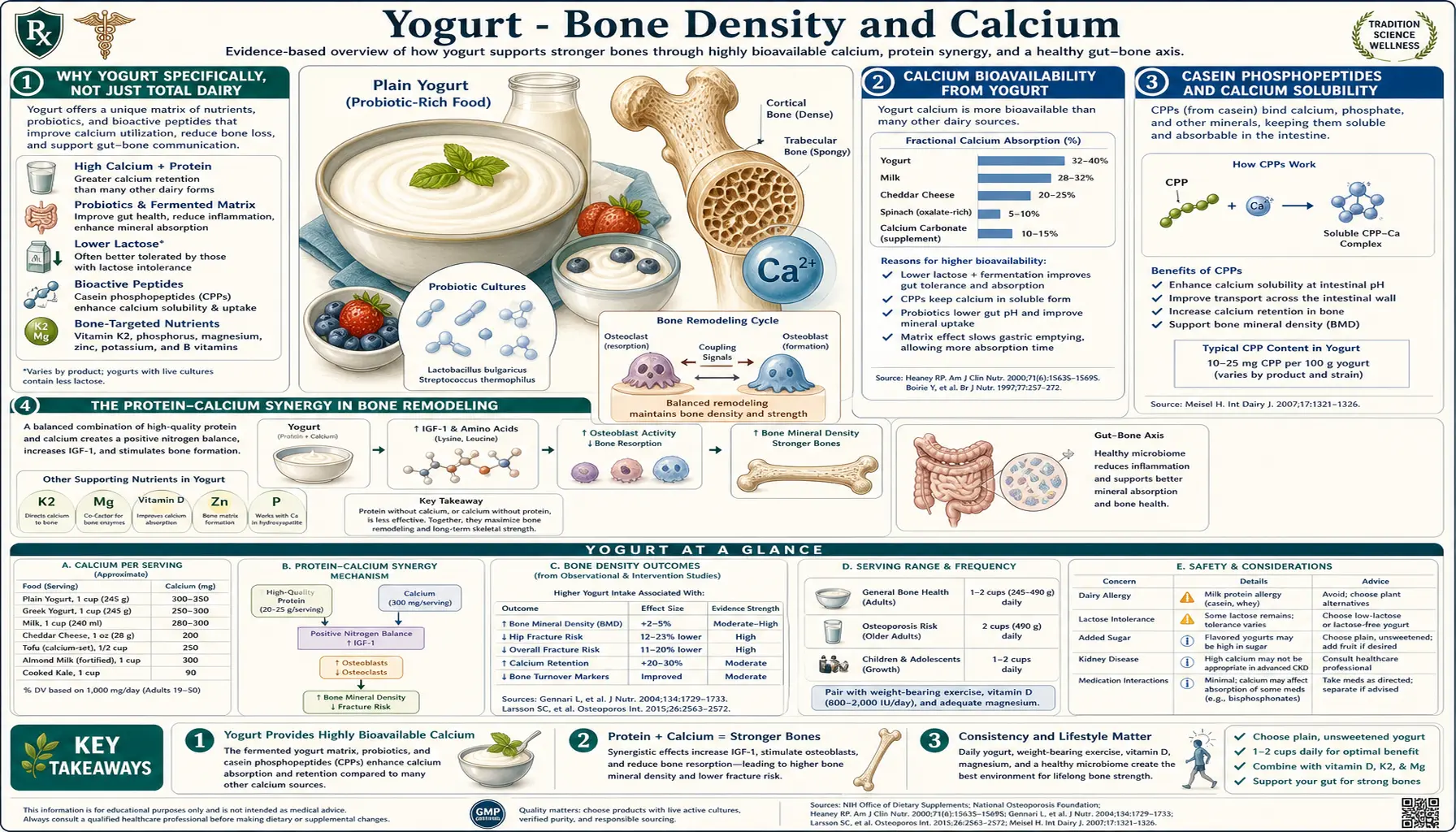
Yogurt is one of the few foods where every gram supports bone health through multiple converging mechanisms: highly bioavailable calcium bound to casein phosphopeptides, high-quality protein providing the amino acid substrate for the bone matrix, bacterially produced vitamin K2 (predominantly MK-9), live cultures that may improve gut absorption of calcium and other minerals, and (in fortified versions) vitamin D for active calcium absorption. The Framingham Offspring cohort and other prospective studies show that yogurt consumption — uniquely among dairy products — is associated with reduced hip-fracture risk in older adults, even after adjustment for total dairy intake. This deep dive walks through each mechanism and the practical guidance for using yogurt as part of a bone-protective dietary pattern.
Table of Contents
- Why Yogurt Specifically, Not Just Total Dairy
- Calcium Bioavailability from Yogurt
- Casein Phosphopeptides and Calcium Solubility
- The Protein-Calcium Synergy in Bone Remodeling
- Bacterial Vitamin K2 (MK-9) Production
- Vitamin D Fortification
- The Framingham Offspring Hip-Fracture Data
- Adolescent Peak Bone Mass
- Practical Application in Older Adults and Postmenopausal Women
- Cautions (Acid Whey, Excess Protein, Magnesium Balance)
- Key Research Papers
- Connections
- Featured Videos
Why Yogurt Specifically, Not Just Total Dairy
Cohort studies of dairy consumption and bone outcomes have produced inconsistent results — some show benefit, some show no effect, and a few have shown signals of increased fracture risk with very high total milk intake. The picture clarifies when individual dairy products are separated. The Framingham Offspring cohort (Sahni et al. 2013, Archives of Osteoporosis) found that yogurt and cheese consumption were associated with higher hip bone mineral density and lower hip fracture risk in older adults, while fluid milk consumption alone showed weaker or absent associations.
Several explanations have been proposed for this pattern:
- Fermented dairy provides bacterially produced vitamin K2 (menaquinones, especially MK-7 to MK-9), which fluid milk lacks. K2 activates osteocalcin to bind calcium into the bone matrix — without K2, calcium can be absorbed but is not optimally deposited into bone.
- The casein-bound calcium in fermented dairy may be more bioavailable than the soluble calcium in fluid milk for individuals with subclinical gastric hypochlorhydria or lactase non-persistence-related gut inflammation.
- Yogurt is consumed in different contexts than fluid milk — often alongside fruit (vitamin C, magnesium), as a substitute for less-nutrient-dense snacks, and at meals where total dietary calcium retention may be higher.
- Probiotic effect on calcium absorption — some clinical trials of probiotic supplementation (without yogurt) have shown modest improvement in calcium absorption, possibly through increased short-chain fatty acid production and consequent reduction in cecal pH.
- Lower added-sugar exposure — flavored fluid milks and milk drinks often have added sugar; plain yogurt purchasers typically have a slightly healthier overall diet pattern (confounding rather than causation).
The implication is that recommending "more dairy" for bone health is less useful than recommending "more fermented dairy" — yogurt and cheese specifically — alongside attention to vitamin D, vitamin K2, protein adequacy, and weight-bearing exercise. For more on the broader bone-protection framework, see Osteoporosis.
Calcium Bioavailability from Yogurt
Calcium absorption from food is governed by chemical form, gastric acidity, vitamin D status, the food matrix, and competing or facilitating dietary components. Yogurt is a particularly absorption-friendly matrix for calcium for several reasons:
- Lactose enhances calcium absorption — the residual lactose in yogurt acts as a mild enhancer of calcium uptake in the small intestine, possibly through promotion of paracellular transport. This effect is largely absent in lactose-intolerant adults but contributes in lactase-persistent individuals.
- Casein phosphopeptides — partial digestion of casein in the stomach and proximal small intestine releases phosphopeptide fragments that bind calcium and keep it in soluble form as the chyme moves into the alkaline jejunum, where free calcium would otherwise precipitate as insoluble salts. (Detailed in next section.)
- The fermentation pH — the acidic pH of yogurt (approximately 4.5) keeps calcium in solution during gastric residence and into the early small intestine, improving absorption window compared with neutral or alkaline calcium-containing foods.
- Adequate vitamin D in fortified versions — many commercial yogurts now add vitamin D, which is required for the active calcium transport pathway through enterocytes. Without adequate D status, only the passive (paracellular) absorption pathway operates and total calcium absorption is reduced.
- Co-presence of magnesium and phosphorus — both required for proper calcium handling in bone tissue, and both naturally present in dairy in appropriate proportions to calcium.
Quantitatively, calcium absorption from yogurt is in the range of 30-35% under normal conditions — comparable to milk and better than most plant sources (kale is about 50%, spinach is about 5% due to oxalate binding, fortified plant milks vary widely based on what calcium salt is used and whether settling occurs).
For comparison, calcium absorption from common supplements: calcium carbonate is about 25-30% (and requires gastric acid for solubilization, so should be taken with food); calcium citrate is about 35% (does not require gastric acid); calcium phosphate is about 25%. Yogurt-source calcium compares favorably with all of these.
Casein Phosphopeptides and Calcium Solubility
Casein contains clusters of phosphoserine residues that bind divalent cations including calcium, magnesium, iron, and zinc. When casein is partially digested by gastric pepsin and pancreatic enzymes, fragments containing these phosphoserine clusters are released as "casein phosphopeptides" (CPPs). The most studied CPP is the beta-CN(1-25) fragment from beta-casein and the alpha-S1-CN(43-79) fragment from alpha-S1-casein.
The functional role of CPPs in calcium handling:
- Solubilization in the alkaline small intestine — as gastric chyme enters the duodenum and is neutralized to pH 6.5-7.5 by pancreatic bicarbonate, free ionic calcium would normally precipitate as calcium phosphate, calcium carbonate, or calcium oxalate. CPPs chelate calcium in a soluble complex that remains available for absorption.
- Maintenance of absorbable concentration along the small intestinal length — without CPPs, most calcium absorption is concentrated in the duodenum where pH is still low enough to keep ionic calcium in solution. With CPPs present, soluble calcium remains available throughout the jejunum and proximal ileum, extending the absorption window.
- Reduced calcium loss in feces — in studies with stable calcium isotopes, CPP-containing meals show higher fractional absorption and lower fecal calcium loss compared with calcium meals without CPP.
The clinical importance of CPPs is partially debated — their effect is most pronounced in scenarios of low gastric acid (older adults on PPI therapy, autoimmune atrophic gastritis), where the alkaline intestinal precipitation problem is most acute. In adults with normal gastric acid, the CPP effect adds to but does not dominate calcium absorption.
CPPs are also added as an isolated ingredient in some functional foods marketed for bone health and dental remineralization (CPP-ACP, sold as Recaldent and incorporated into some chewing gums and toothpastes, has documented enamel-remineralizing effect in cavities research).
The Protein-Calcium Synergy in Bone Remodeling
For decades the conventional wisdom held that dietary protein "leaches" calcium from bone because metabolism of sulfur-containing amino acids produces sulfate that requires urinary excretion as an obligate anion, and the cation balance is maintained partly by urinary calcium excretion. This led to concern that high-protein diets — like the high-protein Greek yogurt patterns — would accelerate bone loss.
Modern research has largely overturned this view. The work of Jane Kerstetter and colleagues (Yale, then UConn) over the 2000s and 2010s clarified that:
- Increased urinary calcium excretion with higher protein intake is partially explained by increased intestinal calcium absorption, not by withdrawal from bone. The net effect on calcium balance is neutral or slightly positive.
- Protein is required for IGF-1 production, which directly stimulates osteoblast activity and bone matrix formation. Low-protein diets in older adults are associated with lower IGF-1, lower bone mineral density, and higher fracture risk.
- The Framingham, Iowa Women's Health Study, and Health Professionals Follow-Up cohorts all show that higher protein intake (within physiologic range) is associated with better bone outcomes, not worse, when calcium intake is adequate.
- The negative effect of protein on bone is observed only in the context of inadequate calcium intake. With calcium adequacy, the protein effect on bone is positive.
Greek yogurt is therefore close to an ideal "bone food" — high in both protein and calcium, with the dietary combination that maximizes IGF-1 stimulation, osteoblast activity, and matrix synthesis while providing the calcium substrate. Older adults at risk of sarcopenia and osteoporosis — the two conditions tend to track together — benefit doubly from a high-protein, calcium-containing yogurt-rich diet pattern.
For more on the muscle-protein-synthesis aspect of this, see the Leucine page — leucine is the key amino acid trigger for muscle protein synthesis, and yogurt is a convenient leucine-rich whole food.
Bacterial Vitamin K2 (MK-9) Production
Vitamin K2 (menaquinones) is the form of vitamin K that activates osteocalcin and matrix Gla protein (MGP) in bone and vascular tissue. Without adequate K2, osteocalcin remains in its inactive (undercarboxylated) form and cannot bind calcium for incorporation into the bone matrix — calcium can be absorbed and circulated but does not optimally deposit into hydroxyapatite. The clinical consequences include both lower bone mineral density and (potentially) increased vascular calcification, since MGP normally prevents calcium deposition in arterial walls.
K2 exists in multiple subtypes named by the length of their isoprenoid side chain (MK-4 through MK-13). Major dietary sources:
- MK-4 — primarily from animal foods (egg yolks, liver, butter, meat). Endogenously converted from dietary K1 (phylloquinone) in some tissues.
- MK-7 — the famous Japanese natto vitamin (from Bacillus subtilis natto). Long half-life (3 days) makes it the most clinically active form per milligram. Niche supplement category.
- MK-8 and MK-9 — produced by various lactic acid bacteria including those in cheese and yogurt fermentation. Aged hard cheeses (Gouda, Edam, Jarlsberg) are particularly rich in MK-8 and MK-9. Yogurt cultures produce smaller amounts.
- MK-10 to MK-13 — produced by some gut bacteria; absorbed in unclear quantities.
The contribution of yogurt to total dietary K2 is modest compared with aged cheeses or natto, but it is non-zero and adds to the cumulative K2 exposure of a yogurt-and-cheese-rich diet. The Rotterdam Study (Gast et al. 2009, Nutrition, Metabolism & Cardiovascular Diseases) found that higher dietary K2 (predominantly from fermented dairy in that population) was associated with reduced coronary calcification and reduced cardiovascular mortality — an effect not seen with vitamin K1 from leafy greens.
For individuals targeting bone health specifically, the practical implication is that a daily yogurt-plus-aged-cheese pattern provides better K2 exposure than yogurt alone or any non-fermented dairy pattern. For osteoporosis-specific recommendations, see Vitamin K2.
Vitamin D Fortification
Vitamin D is required for active calcium absorption from the small intestine — without adequate D status, only the passive (paracellular) absorption pathway operates and overall calcium absorption is reduced to approximately 10-15% rather than the 30-35% achievable with adequate D.
The classic public health intervention for vitamin D inadequacy in the US has been fluid milk fortification (since 1933). Yogurt is typically not fortified as universally, but a growing fraction of US-market yogurts are now D-fortified, typically to provide approximately 20% of the DV (100 IU) per 6-oz serving.
For individuals using yogurt as a primary calcium source, choosing a D-fortified version provides incremental benefit. Alternatively, taking a separate vitamin D supplement (1000-2000 IU/day for most adults, more for those who are deficient or have minimal sun exposure) addresses the same issue independently of food source.
For more on optimal vitamin D dosing and serum 25-hydroxyvitamin D testing, see Vitamin D3 and Vitamin D Test.
The Framingham Offspring Hip-Fracture Data
The Framingham Offspring Study, a prospective cohort initiated in 1971 as the second generation of the original Framingham Heart Study, has produced some of the cleanest available data on individual food categories and bone outcomes. The Sahni et al. analyses (Archives of Osteoporosis 2013; American Journal of Clinical Nutrition 2014) followed 3,212 adults (mean age 60) for up to 16 years and analyzed hip fracture incidence by food intake patterns assessed by food frequency questionnaire.
Key findings:
- Each additional serving per week of yogurt was associated with approximately 6% reduction in hip fracture risk over follow-up.
- Cheese consumption similarly was associated with hip-fracture protection.
- Fluid milk showed weaker association after adjustment for other dairy.
- The yogurt-and-cheese pattern was associated with higher femoral neck and total hip bone mineral density at baseline.
- The effect persisted after adjustment for total calcium intake, vitamin D status, physical activity, BMI, smoking, and other lifestyle factors, suggesting an independent fermented-dairy effect beyond what total calcium alone would predict.
The Framingham finding has been corroborated in the Tucker et al. 2002 cohort analysis (Tufts), in the Iowa Women's Health Study cohort, and in several European prospective studies. The effect is most consistently observed in older adults, where baseline bone-mass loss is highest and the protective contribution of a single dietary change is most measurable. In younger adults with adequate baseline diets, yogurt is not associated with major incremental benefit beyond what a calcium-and-protein-adequate baseline diet would already provide.
Adolescent Peak Bone Mass
Peak bone mass — the maximum bone mineral content achieved across the lifespan — is reached in most individuals between ages 18 and 30 (varies by skeletal site). The bone density attained at peak strongly predicts lifetime fracture risk decades later: an individual who reaches a higher peak bone mass enters middle age with more reserve, so the inevitable post-menopausal or age-related bone loss results in a less catastrophic final density.
Adolescence is the highest-leverage period for dietary calcium intake. The peer-reviewed evidence supports a target of approximately 1,300 mg calcium per day during ages 9-18 — substantially above the adult target of 1,000-1,200 mg. Yogurt is one of the most practical vehicles for hitting this target: a 6-oz serving provides 200-300 mg of highly bioavailable calcium with simultaneous protein and other nutrients required for bone matrix synthesis.
Cavadini et al. (2000, American Journal of Clinical Nutrition) and other adolescent intervention trials have shown that adding 1-2 servings of dairy per day during adolescence can produce 1-3% greater peak bone mineral density compared with no intervention — an effect that, if maintained, may translate to approximately 10-20% reduction in lifetime hip fracture risk decades later.
For families of adolescents, the practical message: a daily plain or lightly-sweetened yogurt as a snack or breakfast component is one of the highest-yield single dietary habits for lifetime bone health. The benefit accrues over decades and is not visible at the time of consumption — making it a parental rather than adolescent priority, but worth emphasizing.
Practical Application in Older Adults and Postmenopausal Women
For older adults — particularly postmenopausal women, who face the rapid 2-3%/year bone density loss during the perimenopausal window — daily yogurt consumption is one of the higher-leverage non-pharmacologic interventions:
- Target intake — 1-2 servings (6-12 oz) of plain, unsweetened yogurt per day. Either Greek or traditional based on lactose tolerance and protein preference. Calcium-fortified or naturally calcium-rich varieties preferred.
- Combine with adequate vitamin D — 1000-2000 IU/day supplemental D3 or sun exposure, with periodic 25-hydroxyvitamin D testing (target 30-50 ng/mL).
- Combine with vitamin K2 — either from daily aged-cheese consumption (Gouda, Jarlsberg, hard parmesan), natto, or a supplemental MK-7 (90-180 mcg/day).
- Adequate total protein intake — 1.0-1.2 g/kg/day for older adults, distributed across meals. A Greek yogurt snack between meals helps achieve this target without forcing oversized main meals.
- Weight-bearing and resistance exercise — the strongest non-dietary intervention for bone density preservation. Diet provides substrate; mechanical loading provides the stimulus to use it.
- Monitor with DEXA scanning at intervals appropriate to risk (typically every 1-2 years for high-risk individuals, 2-5 years for average-risk).
- Avoid excessive sodium and caffeine, both of which increase urinary calcium loss.
For individuals on bisphosphonates, denosumab, or other pharmacologic osteoporosis therapy, yogurt-based calcium intake works synergistically with the medication — the medication slows resorption while diet provides substrate for ongoing formation. Calcium-rich foods (including yogurt) should be taken at least 1 hour separated from oral bisphosphonates to avoid binding interference with absorption.
For more on the broader osteoporosis management framework, see Osteoporosis.
Cautions (Acid Whey, Excess Protein, Magnesium Balance)
- Excessive protein intake without proportional calcium — while the modern view is that protein is not bone-harmful when calcium is adequate, the converse remains true: very high protein intake (>2 g/kg/day) without adequate calcium can produce negative calcium balance. Yogurt provides both, but for individuals supplementing additional protein (whey shakes, etc.), ensure calcium intake scales proportionally.
- Calcium-magnesium ratio — dairy is calcium-dominant and relatively magnesium-poor (yogurt provides approximately 15% of the DV of magnesium per serving versus 25-30% of DV calcium). High dairy intake without magnesium attention can produce a high Ca:Mg ratio that some research suggests may be cardiovascularly unfavorable. Include magnesium-rich foods (nuts, dark leafy greens, whole grains, dark chocolate) alongside dairy.
- Added sugar in flavored yogurts — commercial fruit-on-the-bottom yogurts often contain 18-24 g added sugar per serving, which contributes to insulin resistance and the inflammatory pattern that long-term may worsen bone outcomes. Always prefer plain unsweetened yogurt and add fresh fruit at home.
- Calcium supplementation versus food calcium — some 2010s research raised concern that high-dose calcium supplements (especially >1000 mg/day) might be associated with increased cardiovascular events. The signal has been inconsistent and recent meta-analyses largely do not confirm the effect, but the conservative interpretation is to prefer food-source calcium (yogurt, cheese, leafy greens) over supplements when possible.
- Acid whey environmental concerns — not a direct health caution but a sustainability consideration. Greek yogurt production generates 2-3x volumes of acid whey waste. The industry is largely managing this through livestock feed and biogas recovery, but consumers concerned about supply-chain sustainability may consider rotating between Greek and traditional yogurt.
- Lactose intolerance — mostly addressed by the live-culture effect (see Lactose Tolerance), but severely intolerant individuals may need lactose-free yogurt or smaller serving sizes.
- Cow's milk protein allergy (CMPA) — distinct from lactose intolerance. CMPA patients should avoid yogurt entirely; alternative calcium sources include calcium-fortified plant milks, leafy greens, almonds, and sardines/canned salmon with bones.
Key Research Papers
- Sahni S et al. (2013). Milk and yogurt consumption are linked with higher bone mineral density but not with hip fracture: the Framingham Offspring Study. Archives of Osteoporosis. — Search PubMed
- Sahni S, Mangano KM, Tucker KL, Kiel DP, Casey VA, Hannan MT (2014). Protective association of milk intake on the risk of hip fracture: results from the Framingham Original Cohort. Journal of Bone and Mineral Research. — Search PubMed
- Kerstetter JE et al. (2003). The impact of dietary protein on calcium absorption and kinetic measures of bone turnover in women. Journal of Clinical Endocrinology & Metabolism. — Search PubMed
- Heaney RP (2000). Calcium, dairy products and osteoporosis. Journal of the American College of Nutrition. — Search PubMed
- Weaver CM (2014). Calcium supplementation: is protecting against osteoporosis counter to protecting against cardiovascular disease? Current Osteoporosis Reports. — Search PubMed
- Gast GCM et al. (2009). A high menaquinone intake reduces the incidence of coronary heart disease. Nutrition, Metabolism & Cardiovascular Diseases. — PMID 19179058
- Cavadini C, Siega-Riz AM, Popkin BM (2000). US adolescent food intake trends from 1965 to 1996. Archives of Disease in Childhood. PubMed: Adolescent calcium trends
- Schurch MA et al. (1998). Protein supplements increase serum insulin-like growth factor-I levels and attenuate proximal femur bone loss in patients with recent hip fracture. Annals of Internal Medicine. — Search PubMed
- Pribila BA et al. (2000). Improved lactose digestion and intolerance among African-American adolescent girls fed a dairy-rich diet. Journal of the American Dietetic Association. — PMID 10812376
- Rizzoli R et al. (2014). Benefits and safety of dietary protein for bone health — an expert consensus paper endorsed by the European Society for Clinical and Economical Aspects of Osteoporosis. Osteoporosis International. — Search PubMed
- Iuliano S et al. (2021). Effect of dietary sources of calcium and protein on hip fractures and falls in older adults in residential care: cluster randomised controlled trial. BMJ. — PMID 34670754
- FitzGerald RJ, Murray BA, Walsh DJ (2004). Hypotensive peptides from milk proteins. Journal of Nutrition. — Search PubMed
PubMed Topic Searches
- PubMed: Yogurt and BMD/fracture
- PubMed: CPPs and calcium absorption
- PubMed: K2 in fermented dairy
- PubMed: Kerstetter protein/calcium
- PubMed: Adolescent peak bone mass
Connections
- Yogurt Overview
- Yogurt Benefits Hub
- Probiotic Strains
- Greek vs Regular
- Lactose Tolerance
- Calcium
- Magnesium
- Vitamin D3
- Vitamin K2
- Osteoporosis
- Vitamin D Test
- Leucine
- Milk
- Kale (Calcium)
- Sardines (Calcium and Vitamin D)