Sweet Potato for Skin Nutrient Density
Dietary carotenoids deposit measurably in the dermis within weeks of sustained intake, and the skin's carotenoid concentration is one of the more reliable biomarkers of antioxidant status and habitual vegetable intake. Stahl and Sies' work in Heidelberg over the past two decades demonstrated that beta-carotene supplementation (or beta-carotene-rich diet) raises the minimal erythemal dose — the UV exposure required to produce visible redness — by roughly 30% over 8–12 weeks of consistent intake. Stephen and Whitehead's perception studies showed that carotenoid skin coloration is rated as "healthier looking" than equivalent melanin tan, suggesting an evolved human preference for the dietary-derived skin pigment. Sweet potato, with the highest beta-carotene density of any commonly eaten food, is one of the most efficient dietary vehicles for raising skin carotenoid concentration. This page walks through the carotenoid-to-dermis pathway, the photoprotection mechanism, the measurable skin-yellowness and Raman spectroscopy biomarkers, and the practical guidance for using dietary sweet potato as a complement (not a replacement) for topical sunscreen.
Table of Contents
- The Carotenoid-to-Skin Deposition Pathway
- Stahl and Sies: Carotenoids and Photoprotection
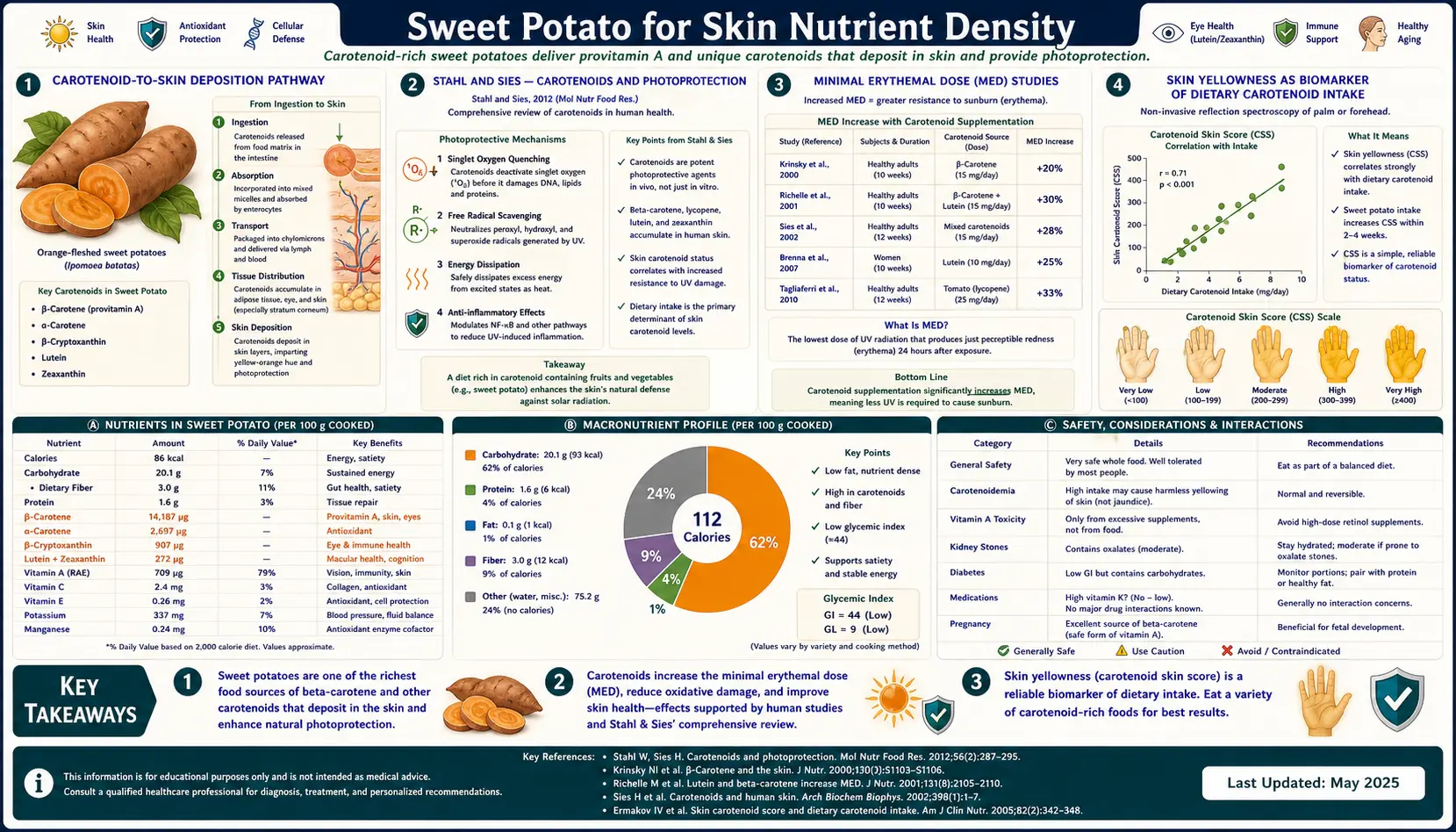
- Minimal Erythemal Dose (MED) Studies
- Skin Yellowness as Biomarker of Dietary Carotenoid Intake
- Resonance Raman Spectroscopy of Skin Carotenoids
- Retinoic Acid and Keratinocyte Differentiation
- Stephen-Whitehead: Carotenoid Coloration and Perceived Health
- Acne and Cellular Turnover
- Wound Healing and Epithelial Repair
- Practical Guidance: Diet vs Topicals vs Sunscreen
- Key Research Papers
- Connections
- Featured Videos
The Carotenoid-to-Skin Deposition Pathway
Dietary beta-carotene from sweet potato (or other orange/green vegetables) is absorbed in the small intestine, packaged into chylomicrons, and exported via lymph to the systemic circulation. Once in circulation, beta-carotene partitions into lipoproteins (LDL and HDL) and is transported to tissues throughout the body. The skin — particularly the stratum corneum and the adipose-rich deeper dermis — is one of the major non-hepatic carotenoid storage sites in the human body.
The deposition is gradual. After increasing dietary carotenoid intake, plasma carotenoid concentration rises within days, but skin carotenoid concentration rises over 4–8 weeks and reaches a new steady state at 8–12 weeks. The skin-to-plasma carotenoid concentration ratio in habitually high-vegetable-intake individuals is roughly 5:1 (skin contains ~5 times the concentration found in plasma) — demonstrating that skin actively accumulates dietary carotenoids over time.
The deposition is bidirectional. When dietary intake decreases, skin carotenoid concentration falls, again with a several-week lag. Skin carotenoid status thus reflects habitual long-term intake rather than the last meal, which makes it a useful biomarker for vegetable consumption in epidemiologic and clinical studies.
Two carotenoid classes deposit preferentially in different skin compartments:
- Beta-carotene, alpha-carotene, gamma-carotene, lycopene — deposit primarily in the deeper dermis and subcutaneous adipose tissue. Beta-carotene from sweet potato falls in this group.
- Lutein and zeaxanthin — deposit preferentially in the stratum corneum and at higher concentrations near the skin surface. These are the xanthophyll carotenoids dominant in dark leafy greens (kale, spinach).
Both classes contribute to skin antioxidant defense, but through different micro-anatomical locations.
Stahl and Sies: Carotenoids and Photoprotection
Wilhelm Stahl and Helmut Sies at Heinrich-Heine University in Düsseldorf published the foundational human work on dietary carotenoids and skin photoprotection beginning in the late 1990s. Their basic experimental paradigm:
- Recruit healthy adult volunteers
- Measure baseline minimal erythemal dose (MED) — the UV exposure that produces visible redness 24 hours after exposure
- Begin supplementation with beta-carotene, lycopene, or a carotenoid-rich food (tomato paste, sweet potato, carrot juice)
- Re-measure MED at 8, 10, and 12 weeks
The consistent finding across multiple trials: sustained carotenoid supplementation raised MED by approximately 25–35% over the intervention period. The carotenoid was acting as an in-skin antioxidant that quenched the reactive oxygen species generated by UV exposure before they could produce the inflammatory cascade leading to visible erythema.
The mechanism involves several layers:
- Direct quenching of singlet oxygen (carotenoids are exceptionally efficient singlet oxygen scavengers)
- Scavenging of peroxyl radicals in lipid membranes
- Reduction of UV-induced lipid peroxidation
- Modulation of UV-induced gene expression (decreased COX-2 induction)
- Some inhibition of UV-induced matrix metalloproteinase (MMP-1) activation, slowing the photoaging cascade
The protection is not absolute — carotenoid-supplemented subjects still burn at sufficiently high UV doses — but the threshold for burning is meaningfully higher, and the same UV exposure produces less visible erythema and less DNA damage in carotenoid-replete versus depleted skin.
Minimal Erythemal Dose (MED) Studies
The MED measurement is the standard quantitative endpoint for skin photoprotection research. It is measured by exposing small patches of skin (typically on the back or buttocks) to a series of UV doses from a calibrated lamp, scoring the patches 24 hours later for visible redness, and identifying the lowest dose that produces minimally perceptible erythema.
MED is usually expressed in mJ/cm² of UV-B equivalent. Typical baseline values for Type II fair-skinned adults are 25–40 mJ/cm². Sustained carotenoid intake raises this to 35–55 mJ/cm² over 8–12 weeks — a meaningful but not dramatic protective effect.
For context, a typical noon-sun exposure on a clear summer day in temperate latitudes delivers 1 MED in roughly 15–25 minutes for unprotected fair skin. A 30% increase in MED extends that exposure time to roughly 20–33 minutes. This is real protection — but it is a fraction of the protection provided by an SPF 30 sunscreen (which extends safe exposure by a factor of 30). Dietary carotenoid is a complement to sunscreen, not a substitute.
The cleanest single trial for sweet potato specifically is limited — most MED studies used isolated beta-carotene supplementation or tomato paste lycopene. By extrapolation from the carotenoid intake achieved (which determines skin deposition), regular sweet potato consumption (3–4 servings per week) is sufficient to produce the photoprotective MED elevation seen in the supplementation trials.
Skin Yellowness as Biomarker of Dietary Carotenoid Intake
Skin coloration can be quantitatively characterized using the CIE L*a*b* color space, which separates lightness (L*), red-green axis (a*), and yellow-blue axis (b*). The b* component — how yellow versus blue the skin appears — correlates strongly with skin carotenoid content. Carotenoids absorb light in the blue-violet region and reflect yellow-orange, so increasing skin carotenoid deposition shifts the b* value upward.
This relationship has been validated in multiple populations:
- People with higher self-reported fruit and vegetable intake have higher skin b* values
- Controlled diet trials that increase carotenoid intake produce measurable b* increases within 4 weeks
- The relationship is most reliable on relatively un-tanned skin areas (inner forearm, palm), since melanin also affects color and confounds the measurement on sun-exposed skin
Tools like the Veggie Meter (a portable resonance Raman spectroscopy device) have been deployed in school nutrition research to objectively measure skin carotenoid status without requiring blood draw. The measurement takes seconds, is non-invasive, and reliably tracks dietary carotenoid intake over the past 4–6 weeks.
For an individual experimenting with sweet potato as a dietary intervention, the practical takeaway is that skin tone change within the first 1–2 months is a reliable indicator that the intervention is "taking." A faint warming of the inner-forearm skin tone, particularly noticeable on the palms and soles, indicates that dietary beta-carotene is reaching circulation and depositing in tissues.
Resonance Raman Spectroscopy of Skin Carotenoids
Resonance Raman spectroscopy provides the most precise non-invasive measurement of skin carotenoid concentration. The technique uses a low-power blue laser (488 nm) to excite the carotenoid molecules in the skin, which then emit a characteristic Raman scattering signal whose intensity is proportional to the carotenoid concentration in the illuminated tissue volume.
Validated against blood carotenoid measurement and skin biopsy, Raman skin carotenoid scores show:
- Strong correlation with habitual fruit and vegetable intake (r = 0.6–0.8 in most studies)
- Modest correlation with single-meal carotenoid intake (the skin pool integrates over weeks, not hours)
- Inverse correlation with smoking status (smokers have lower skin carotenoid concentrations at any given dietary intake, due to oxidative consumption)
- Inverse correlation with body mass index (carotenoids partition into adipose tissue, so total body fat dilutes the skin concentration)
- Positive correlation with the AREDS-type macular pigment optical density (a related measure of carotenoid status in a different tissue)
The technique has been used in nutritional research, in clinical trials evaluating dietary interventions, and increasingly in consumer-facing wellness applications. The takeaway is that dietary carotenoid intake produces measurable, objectively verifiable changes in skin and macular pigment status that integrate over weeks to months — a useful feedback signal for individuals trying to assess the impact of dietary changes.
Retinoic Acid and Keratinocyte Differentiation
Beta-carotene from sweet potato is converted (partially) to retinol, and retinol is in turn oxidized in tissues to all-trans-retinoic acid. Retinoic acid is the active hormone-like ligand of the RAR/RXR nuclear receptor family, which controls expression of hundreds of genes involved in cell proliferation, differentiation, and apoptosis.
In the skin, retinoic acid signaling is essential for normal keratinocyte differentiation — the orderly progression from basal cell to spinous cell to granular cell to fully keratinized stratum corneum that maintains the epidermal barrier. Deficiency of retinoic acid signaling produces:
- Hyperkeratosis (abnormal thickening of the stratum corneum, follicular hyperkeratosis)
- Follicular plugging (the substrate for comedonal acne)
- Phrynoderma (the "toad skin" dermatologic manifestation of severe Vitamin A deficiency)
- Impaired barrier function with increased transepidermal water loss
Adequate dietary Vitamin A (from sweet potato beta-carotene plus the small amount in eggs, dairy, and fish) supports normal keratinocyte differentiation without requiring topical retinoids. For more aggressive dermatologic conditions (severe nodulocystic acne, severe psoriasis), pharmacologic topical or oral retinoids are used at doses far above dietary intake — but the underlying skin biology that those drugs are amplifying is the same biology that adequate dietary Vitamin A supports at a baseline level.
See our Vitamin A for Skin deep-dive for the full discussion of topical and oral retinoid pharmacology.
Stephen-Whitehead: Carotenoid Coloration and Perceived Health
An interesting parallel literature on the social/psychological dimension of skin carotenoid pigmentation has emerged from work led by Ian Stephen, David Perrett, Whitehead, and colleagues. Their studies test the hypothesis that carotenoid-derived skin yellowness is an evolved signal of underlying health and reproductive fitness.
The methodology typically involves presenting raters with facial photographs in which a skin-tone parameter has been digitally manipulated, and asking the raters to choose the image that looks "healthiest" or "most attractive." The repeated finding:
- Raters consistently prefer skin tones shifted in the direction of higher carotenoid coloration over equivalent shifts in the direction of higher melanin tan
- The preference for carotenoid coloration is cross-cultural — observed in samples from Europe, Asia, and Africa
- The effect size is modest but statistically robust across multiple replications
- The preference does not appear to be driven by perceived ethnicity or skin-tone matching with the rater's own appearance
The hypothesis is that the human visual system has evolved sensitivity to skin carotenoid content because it provides reliable real-time information about an individual's habitual diet, antioxidant status, and possibly underlying immune/reproductive fitness. The evolutionary argument is speculative, but the empirical finding — that observers can detect and prefer carotenoid skin coloration — is well-replicated.
The practical relevance for sweet potato consumption: in addition to the photoprotective and dermatologic effects, sustained intake produces a visible cosmetic effect (subtle warming of skin tone) that observers may register positively. This is not a dramatic effect, and it is not a substitute for the bigger cosmetic interventions, but it is real and measurable.
Acne and Cellular Turnover
Acne pathogenesis involves four overlapping processes: follicular hyperkeratosis (the comedone), increased sebum production, Cutibacterium acnes proliferation in the follicle, and inflammation. Vitamin A signaling addresses the first of these directly — retinoic acid normalizes keratinocyte differentiation and prevents the follicular plugging that initiates the comedone.
The most powerful acne therapies in dermatology are retinoid-based: topical tretinoin (Retin-A), topical adapalene (Differin), and oral isotretinoin (Accutane). These work by delivering supraphysiologic concentrations of retinoid activity directly to the skin or systemically. For mild-to-moderate acne not requiring pharmacotherapy, the question of whether dietary Vitamin A status meaningfully affects acne severity has been studied with mixed results.
Observational evidence suggests that people with poor dietary Vitamin A status (rare in developed countries, more common where intake is restricted) have somewhat more comedonal acne. People with adequate dietary Vitamin A do not appear to benefit from supraphysiologic Vitamin A supplementation for acne — once the receptors are saturated, more does not help and at high enough doses produces hypervitaminosis A.
The practical implication is that adequate dietary Vitamin A (from sweet potato and other sources) supports normal skin turnover and may be a small contributor to better skin appearance, but is not a replacement for proven topical or oral acne therapies in patients with significant disease. See our Acne page for the broader management approach.
Wound Healing and Epithelial Repair
Vitamin A is essential for wound healing through its role in epithelial cell proliferation and the inflammatory phase of repair. Patients with Vitamin A deficiency show delayed wound healing, impaired epithelialization, and increased risk of wound infection. Patients on chronic corticosteroids (which suppress wound healing through multiple mechanisms including impaired retinoid signaling) sometimes benefit from supplemental Vitamin A specifically to restore wound-healing capacity.
For the general population, dietary Vitamin A from sweet potato and other sources is adequate to support normal wound healing. Targeted supplementation is reserved for:
- Documented Vitamin A deficiency (rare in developed countries except in malabsorption syndromes)
- Post-surgical patients on chronic corticosteroids
- Patients with chronic non-healing wounds (pressure ulcers, diabetic foot ulcers) where Vitamin A status has been documented as deficient
- Severe burn patients (large protein and micronutrient losses require aggressive supplementation)
For routine post-injury recovery in otherwise well-nourished adults, increased sweet potato consumption (and other beta-carotene-rich vegetables) is a reasonable way to ensure adequate Vitamin A supply without the small risks of pharmacologic supplementation.
Practical Guidance: Diet vs Topicals vs Sunscreen
The relationship between dietary nutrition and skin health is real but is the smallest of the three major skin interventions available to adults. In rough order of impact for prevention of photoaging, skin cancer, and general skin appearance:
- Sunscreen. Daily broad-spectrum SPF 30+ on face, neck, and hands is the highest-impact single intervention. It dwarfs every other modality in measured photoprotection and skin-aging endpoints.
- Topical retinoid. Tretinoin or its derivatives, used long-term, produce documented improvements in fine lines, pigmentation, and skin texture. This is the second-tier skin intervention behind sunscreen.
- Dietary carotenoids and antioxidants. Sweet potato, kale, spinach, tomato, and the broader antioxidant-rich diet provide a measurable additional layer of skin photoprotection and may slow photoaging by a small but real amount.
- Other lifestyle factors. Not smoking, adequate sleep, hydration, omega-3 fatty acids, avoiding excess alcohol.
For sweet potato specifically in this framework: consume orange-flesh sweet potato 3–4 times per week as part of an otherwise varied vegetable-rich diet. Do not expect it to replace sunscreen. Do not expect dramatic skin changes within days — the dermal deposition pathway takes 4–8 weeks. Do expect subtle improvements in skin tone uniformity, slightly increased UV tolerance, and a small but measurable contribution to long-term skin appearance over years.
Combine with topical sunscreen for daytime, a topical retinoid (over the counter or prescription) for nighttime if appropriate for your skin, and the rest of the antioxidant-rich diet (dark leafy greens for lutein/zeaxanthin, fatty fish for omega-3 and Vitamin D, berries for additional polyphenols, green tea for catechins). The total dietary approach is more than the sum of any single food.
Key Research Papers
- Stahl W, Sies H — Carotenoids and protection against solar UV radiation. — Search PubMed
- Stahl W, Sies H — Beta-carotene and other carotenoids in protection from sunlight. — Search PubMed
- Köpcke W, Krutmann J — Protection from sunburn with beta-carotene — a meta-analysis. — Search PubMed
- Stephen ID, Coetzee V, Perrett DI — Carotenoid and melanin pigment coloration affect perceived human health. — Search PubMed
- Whitehead RD et al. — You are what you eat: within-subject increases in fruit and vegetable consumption confer beneficial skin-color changes. — Search PubMed
- Whitehead RD et al. — Appealing to vanity: could potential appearance improvement motivate fruit and vegetable consumption? Search PubMed
- Ermakov IV, Gellermann W — Optical detection methods for carotenoids in human skin. — Search PubMed
- Darvin ME et al. — The role of carotenoids in human skin. — Search PubMed
- Heinrich U, Tronnier H, Stahl W, Bejot M, Maurette JM — Antioxidant supplements improve parameters related to skin structure in humans. — Search PubMed
- Cho S et al. — Differential effects of low-dose and high-dose beta-carotene supplementation on the signs of photoaging and type I procollagen gene expression in human skin in vivo. — Search PubMed
- Schagen SK, Zampeli VA, Makrantonaki E, Zouboulis CC — Discovering the link between nutrition and skin aging. PMID 23467449
- Mukherjee S, Date A, Patravale V, Korting HC, Roeder A, Weindl G — Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. PMID 18046911
Connections
- Sweet Potato Benefits (Hub)
- Sweet Potatoes (Main Page)
- Beta-Carotene and Vision
- Sweet Potato Glycemic Index
- Purple vs Orange Cultivars
- Vitamin A
- Vitamin A Benefits Deep Dive
- Vitamin A for Skin & Cellular Differentiation
- Acne
- Psoriasis
- Antioxidants
- Kale (Lutein, Zeaxanthin)
- Blueberries
- All Food Pages