Sweet Potato Glycemic Index
The widely repeated assumption that sweet potato and white potato are metabolically interchangeable is wrong by a wide margin. Boiled sweet potato has a measured glycemic index of approximately 44 (low category, <55), while baked white potato registers 78 (high category, >70) — a 34-point gap on a 100-point scale that translates to a substantially smaller and slower postprandial glucose excursion after equivalent carbohydrate portions. The mechanistic difference is not just sweetness or fiber: sweet potato contains more resistant starch, a higher amylose-to-amylopectin ratio, intact plant-cell-wall structure that physically slows starch hydrolysis, and polyphenols that inhibit alpha-amylase and alpha-glucosidase. Cooking method matters even more than cultivar — the same tuber can shift 30 points on the glycemic index scale depending on whether it is boiled, baked, roasted, or fried. This page is the practical metabolic deep-dive for diabetic and insulin-resistant readers who have heard sweet potato is "good for you" but want the actual numbers, the cooking-method tradeoffs, and the comparative tables to make day-to-day food decisions.
Table of Contents
- Glycemic Index vs Glycemic Load: The Distinction That Matters
- Measured Glycemic Index Values for Sweet Potato
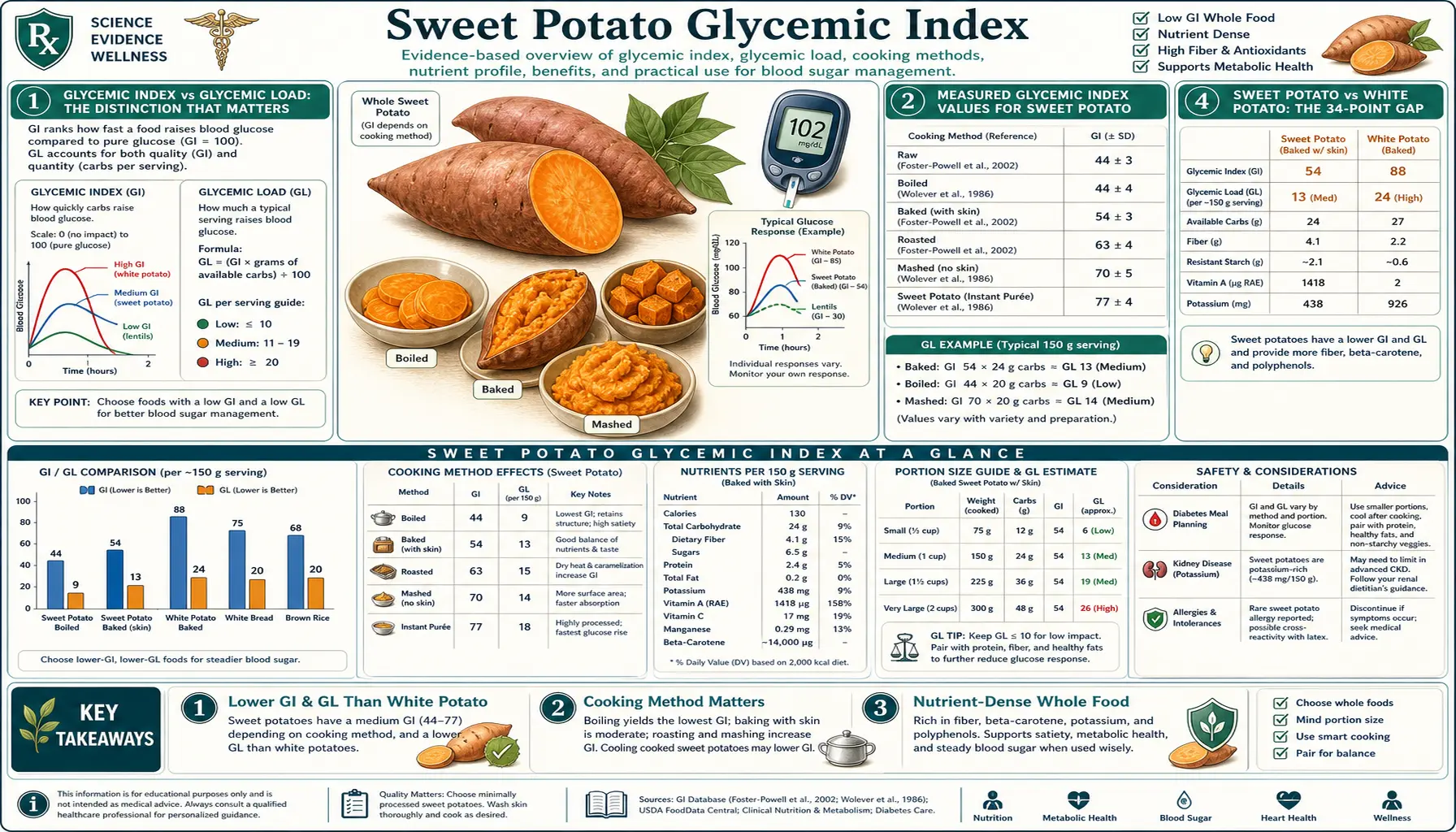
- Sweet Potato vs White Potato: The 34-Point Gap
- How Cooking Method Changes the GI
- The Cool-and-Reheat Resistant Starch Effect
- Mechanisms: Why Sweet Potato Is Slower
- The Caiapo White Sweet Potato Diabetes Trial
- Practical Portions for Diabetics and Insulin-Resistant Eaters
- Combining with Fat, Protein, and Vinegar
- Key Research Papers
- Connections
- Featured Videos
Glycemic Index vs Glycemic Load: The Distinction That Matters
Before walking through the numbers, the distinction between glycemic index (GI) and glycemic load (GL) matters because they answer different questions and are easy to confuse.
Glycemic index is a property of a food itself: when you feed a standardized 50 g portion of available carbohydrate from a specific food to a human subject, how much does their blood glucose rise relative to a reference (usually pure glucose at GI 100)? The reference question is "per gram of carbohydrate, how fast does this food spike my blood sugar?" GI is independent of portion size.
Glycemic load is a property of a serving: GL = (GI × grams of carbohydrate per serving) / 100. The reference question is "how much will this actual portion I am about to eat raise my blood sugar?" GL combines the food's intrinsic glycemic property with the realistic portion size.
Sweet potato is in the low-GI category (under 55) and in the low-to-moderate GL category (under 10 to 15 per serving). A 200 g cooked sweet potato contains approximately 28 g of available carbohydrate, so the glycemic load of one medium boiled sweet potato is approximately (44 × 28) / 100 = 12 — a moderate-to-low load that is well-tolerated by most people with diabetes when paired with protein and fat.
For comparison, a 200 g baked white potato (also ~28 g carbohydrate) has a glycemic load of (78 × 28) / 100 = 22 — nearly twice the postprandial glucose impact for the identical portion.
Measured Glycemic Index Values for Sweet Potato
The published GI values for sweet potato vary by cultivar, ripeness, cooking method, country of origin, and measurement protocol. The Atkinson, Foster-Powell, and Brand-Miller 2008/2021 international GI tables list the following representative values:
- Boiled sweet potato (peeled, 30 min): GI 44 (Australia)
- Boiled sweet potato (peeled, 25 min): GI 46 (USA)
- Baked sweet potato (skin on, 45 min at 180°C): GI 64 (Australia)
- Roasted sweet potato (60 min at 200°C): GI 82 (USA, one study)
- Sweet potato chips/fries: GI 76 (variable)
- Sweet potato pureé: GI 54 (UK)
- Sweet potato Beauregard variety: GI 62 (USA)
- Sweet potato Hayman White variety: GI 39 (USA)
Three practical takeaways from these numbers:
- Boiling produces the lowest GI. The water-immersion cooking limits starch gelatinization, preserves some resistant starch, and avoids the Maillard browning that occurs with dry-heat cooking.
- Baking and roasting roughly double the GI compared to boiling, because the higher dry-heat temperatures more fully gelatinize the starch, making it more accessible to amylase digestion.
- Cultivar effects are real but smaller than cooking effects. Hayman White at GI 39 versus Beauregard at GI 62 is a notable difference, but the boiled-versus-baked difference within a single cultivar is larger.
Sweet Potato vs White Potato: The 34-Point Gap
The most asked question about sweet potato is "is it really better than regular potato for blood sugar?" The answer is yes, by a substantial margin, with the magnitude depending on which cooking method you compare.
| Food | GI | Category |
|---|---|---|
| Boiled sweet potato | 44 | Low |
| Boiled white potato (red-skinned) | 62 | Medium |
| Boiled white potato (Russet) | 70 | Medium-high |
| Baked sweet potato | 64 | Medium |
| Baked white potato (Russet) | 78 | High |
| French fries (white potato) | 75 | High |
| Mashed white potato (instant) | 87 | Very high |
| Mashed white potato (fresh) | 73 | High |
The cleanest head-to-head is boiled-versus-boiled. Boiled sweet potato (GI 44) versus boiled Russet potato (GI 70) is a 26-point gap. For baked-versus-baked, baked sweet potato (GI 64) versus baked Russet (GI 78) is a 14-point gap. The general pattern: sweet potato is metabolically gentler than white potato across every cooking method, but the absolute gap shrinks as cooking method moves from boiling toward baking.
What does this mean clinically? For a person with type 2 diabetes consuming 30 g of available carbohydrate from a starchy side dish, the swap from baked Russet to boiled sweet potato will reduce their two-hour postprandial glucose peak by roughly 15–30 mg/dL on average — not a dramatic effect, but a meaningful one that compounds across daily meals over months and years.
How Cooking Method Changes the GI
The same tuber prepared by different methods produces dramatically different glycemic responses. Starting from highest GI and working down:
- Roasted at high temperature (200°C+) for 60+ minutes — GI 75–85. Maximum starch gelatinization, Maillard browning of surface starches, complete cell-wall breakdown. Almost as glycemic as baked white potato.
- Microwave-baked, whole, skin on — GI ~70. Comparable to oven-baked but slightly less surface caramelization.
- Oven-baked, skin on, 45 min at 180°C — GI ~64. The classic American preparation.
- Sweet potato fries (oven, with olive oil) — GI ~62 with fat slowing absorption; fat does not change the food's intrinsic GI but does slow gastric emptying.
- Mashed (boiled then crushed) — GI ~55. The mashing increases surface area for amylase but the underlying boiled-starch profile remains.
- Boiled, peeled, in chunks, 30 minutes — GI ~46. The reference low-GI preparation.
- Boiled, then cooled and reheated — GI ~40 (see next section on resistant starch).
- Steamed, skin on — GI ~44. Comparable to boiled, slightly more nutrient retention.
The biggest single change is the boiling-versus-roasting spread of roughly 30 GI points on the same tuber. For a person managing blood sugar, that is more impact than switching from sweet potato to a different food. The implication is that if you have a high-GI meal context (e.g. Thanksgiving roasted sweet potatoes), pair them with substantial protein, fat, and acid to flatten the curve, or shift the cooking method to boiling or steaming when feasible.
The Cool-and-Reheat Resistant Starch Effect
One of the most underappreciated metabolic interventions is starch retrogradation. When cooked starch is cooled below approximately 5°C, the gelatinized starch chains begin to re-crystallize into a structure that human amylase cannot digest — functionally, it becomes fiber. This fraction is called type 3 resistant starch (RS3).
The relevant practical sequence:
- Boil or bake the sweet potato as you normally would.
- Refrigerate the cooked sweet potato for at least 12 hours (overnight works perfectly).
- Eat it cold (in a salad, for example), or reheat gently.
The reheated sweet potato now contains substantially more resistant starch than the freshly cooked tuber. Estimates suggest 5–10 percentage points of the total starch is converted to RS3 by overnight refrigeration. The metabolic consequences:
- Lower glycemic response — some of the carbohydrate is no longer rapidly absorbed
- Lower effective calorie content — resistant starch provides ~2 kcal/g (fermentation byproducts) versus 4 kcal/g for digested starch
- Increased colonic short-chain fatty acid production — resistant starch is the favored substrate for butyrate-producing colonic bacteria
- Improved insulin sensitivity at the next meal (the "second-meal effect")
This is the same trick that works for white rice, pasta, and potato. It is one of the few free-lunch interventions in nutrition — the same food, the same total calorie intake, but a measurably better metabolic profile achieved entirely by a refrigeration step.
Mechanisms: Why Sweet Potato Is Slower
Several mechanisms combine to produce the lower glycemic index of sweet potato relative to white potato.
1. Higher amylose-to-amylopectin ratio. Plant starches consist of two glucose polymers: linear amylose and branched amylopectin. Amylose is digested more slowly because its long unbranched chains are more difficult for amylase to access. White potato starch is roughly 80% amylopectin and 20% amylose — weighted toward fast digestion. Sweet potato starch is closer to 70% amylopectin and 30% amylose, shifting the balance toward slower digestion.
2. Dietary fiber content. Sweet potato contains 3–4 g of dietary fiber per 100 g (cooked), compared to 1.5–2.5 g for white potato. Fiber slows gastric emptying, slows enzymatic access to starch granules, and contributes some non-digestible carbohydrate that does not raise blood glucose.
3. Intact cell wall structure. The sweet potato's tuber tissue has thicker, more lignified cell walls than the white potato. Even after cooking, some of the starch granules remain encapsulated within partially intact cell walls, physically delaying amylase access. White potato cell walls largely disintegrate under cooking heat.
4. Polyphenol alpha-amylase inhibition. Sweet potato contains chlorogenic acid, caffeic acid, and other phenolic compounds that competitively inhibit pancreatic alpha-amylase and intestinal brush-border alpha-glucosidase. The effect is small but measurable — comparable in magnitude to a low dose of the diabetic drug acarbose. White potato has substantially less polyphenol content (its polyphenols are concentrated in the skin, which is often discarded).
5. Resistant starch baseline. Even freshly cooked, sweet potato contains 2–4% resistant starch versus 1–2% for white potato. The retrogradation effect described in the previous section adds to this baseline.
These mechanisms are additive, not redundant. Each contributes a few GI points, and the combined effect of all five mechanisms produces the observed 20–30-point gap between sweet potato and white potato at equivalent cooking methods.
The Caiapo White Sweet Potato Diabetes Trial
An interesting but often-overlooked clinical trial used an extract of Caiapo, a white-skinned cultivar of sweet potato grown in Japan and traditionally used for diabetes management. The Ludvik et al. studies (2002, 2003, 2004, 2008) randomized type 2 diabetic patients to either 4 g/day of Caiapo extract or placebo, with the following findings:
- HbA1c decreased from 7.21% to 6.68% in the Caiapo group over twelve weeks, with no change in placebo (statistically significant)
- Fasting plasma glucose decreased in the Caiapo group
- Cholesterol decreased modestly
- No significant adverse effects were reported
The mechanism for Caiapo's glycemic effect is not fully established. Hypotheses include enhanced insulin sensitivity at the muscle level, alpha-glucosidase inhibition, anti-inflammatory effects, and possibly direct insulin-mimetic activity from the storage protein sporamin.
The clinical reach of this finding is limited — Caiapo is a specific cultivar, not the orange sweet potato readily available in U.S. grocery stores, and the trials used a concentrated extract rather than whole food. But the result is suggestive that the metabolic benefits of sweet potato consumption go beyond the passive low-GI property to include some active insulin-sensitizing effect at the tissue level. This is consistent with epidemiologic data showing that populations with high sweet-potato consumption (e.g. traditional Okinawan diet) have very low diabetes prevalence.
Practical Portions for Diabetics and Insulin-Resistant Eaters
For people with type 2 diabetes, pre-diabetes, insulin resistance, or PCOS-related glucose dysregulation, sweet potato is one of the better starchy carbohydrate options, but portion control still matters.
Standard reasonable serving: 150–200 g cooked (one medium-small tuber), which is ~22–28 g of available carbohydrate. For a diabetic eating a 30–45 g carbohydrate target per meal, this is a substantial single carbohydrate source and should not be combined with a second starchy carbohydrate (bread, rice, pasta) at the same meal.
Larger serving for active or non-diabetic eaters: 250–300 g cooked (one large tuber or two small), ~35–42 g carbohydrate. Reasonable for the post-workout meal or for non-diabetic readers who tolerate carbohydrate well.
Frequency: Most days of the week is fine. The fiber, micronutrient density, and low glycemic load make sweet potato one of the carbohydrate sources that does not require restriction even on diabetes-focused diets.
Timing: Many readers report better postprandial response when sweet potato is consumed at lunch or dinner with substantial protein and fat, rather than as a stand-alone breakfast or snack carbohydrate. The mixed meal pattern flattens the glucose curve.
Avoid: Sweet potato pie (added sugar), candied sweet potatoes with marshmallow topping (added sugar plus high-glycemic refined sugar), sweet potato chips (deep-fried in seed oils, high glycemic and inflammatory), commercial sweet potato fries (typically deep-fried in vegetable oil with added starch coatings).
Combining with Fat, Protein, and Vinegar
Three meal-construction principles flatten the glycemic response to any starchy carbohydrate, including sweet potato:
Add fat. Fat slows gastric emptying. Sweet potato eaten with butter, olive oil, coconut oil, avocado, tahini, or alongside a fatty protein (salmon, eggs, beef) produces a slower glucose rise than sweet potato eaten alone. This is also the recommended preparation for maximizing fat-soluble carotenoid absorption (see the Beta-Carotene deep-dive).
Add protein. Protein co-ingestion stimulates a small insulin response that helps clear circulating glucose, and also slows gastric emptying. Sweet potato paired with eggs, fish, meat, beans, or Greek yogurt is metabolically gentler than sweet potato as a stand-alone starch.
Add acid. Vinegar (acetic acid) is the best-studied acid for blunting postprandial glucose. A few teaspoons of apple cider vinegar or balsamic vinegar in a dressing on sweet-potato salad, or a squeeze of lemon, reduces the glycemic peak by 20–30% in repeated clinical trials. The mechanism involves delayed gastric emptying and possibly direct inhibition of disaccharidase activity in the small intestine.
A practical example: 200 g boiled sweet potato cubes, 100 g grilled chicken, two tablespoons olive oil, one tablespoon apple cider vinegar, one cup of mixed greens. This produces a meaningfully smaller postprandial glucose excursion than 200 g baked Russet potato, butter, and a similar protein portion.
Key Research Papers
- Atkinson FS, Foster-Powell K, Brand-Miller JC — International tables of glycemic index and glycemic load values: 2008. PMID 18835944
- Allen JC et al. — Storage stability of cultivar-specific beta-carotene and other carotenoids in pureed and frozen sweet potato. — Search PubMed
- Ludvik B et al. — Improved metabolic control by Ipomoea batatas (Caiapo) is associated with increased adiponectin and decreased fibrinogen levels in type 2 diabetic subjects. — Search PubMed
- Ludvik B et al. — Mode of action of Ipomoea batatas (Caiapo) in type 2 diabetic patients. — Search PubMed
- Allen JC et al. — Glycemic responses to fresh and processed sweet potato (Ipomoea batatas) varieties. — Search PubMed
- Bahado-Singh PS et al. — Relationship between processing method and the glycemic indices of ten sweet potato (Ipomoea batatas) cultivars commonly consumed in Jamaica. — Search PubMed
- Englyst HN et al. — Resistant starch — a 'new' food component: a classification of starch for nutritional purposes. — Search PubMed
- Sajilata MG, Singhal RS, Kulkarni PR — Resistant starch — a review. — Search PubMed
- Johnston KL, Thomas EL, Bell JD — Resistant starch improves insulin sensitivity in metabolic syndrome. — Search PubMed
- Robertson MD et al. — Insulin-sensitizing effects on muscle and adipose tissue after dietary fiber intake in men and women with metabolic syndrome. — Search PubMed
- Liljeberg HG, Björck IM — Delayed gastric emptying rate may explain improved glycaemia in healthy subjects to a starchy meal with added vinegar. — Search PubMed
- Johnston CS et al. — Vinegar improves insulin sensitivity to a high-carbohydrate meal in subjects with insulin resistance or type 2 diabetes. PMID 14694010
Connections
- Sweet Potato Benefits (Hub)
- Sweet Potatoes (Main Page)
- Beta-Carotene and Vision
- Purple vs Orange Cultivars
- Skin Nutrient Density
- Type 2 Diabetes
- Insulin Resistance
- Metabolic Syndrome
- HbA1c
- Fasting Glucose
- Lentils (Low-GI Carbohydrate)
- Apple Cider Vinegar
- All Food Pages