Eggs and the Cholesterol Myth Revisited
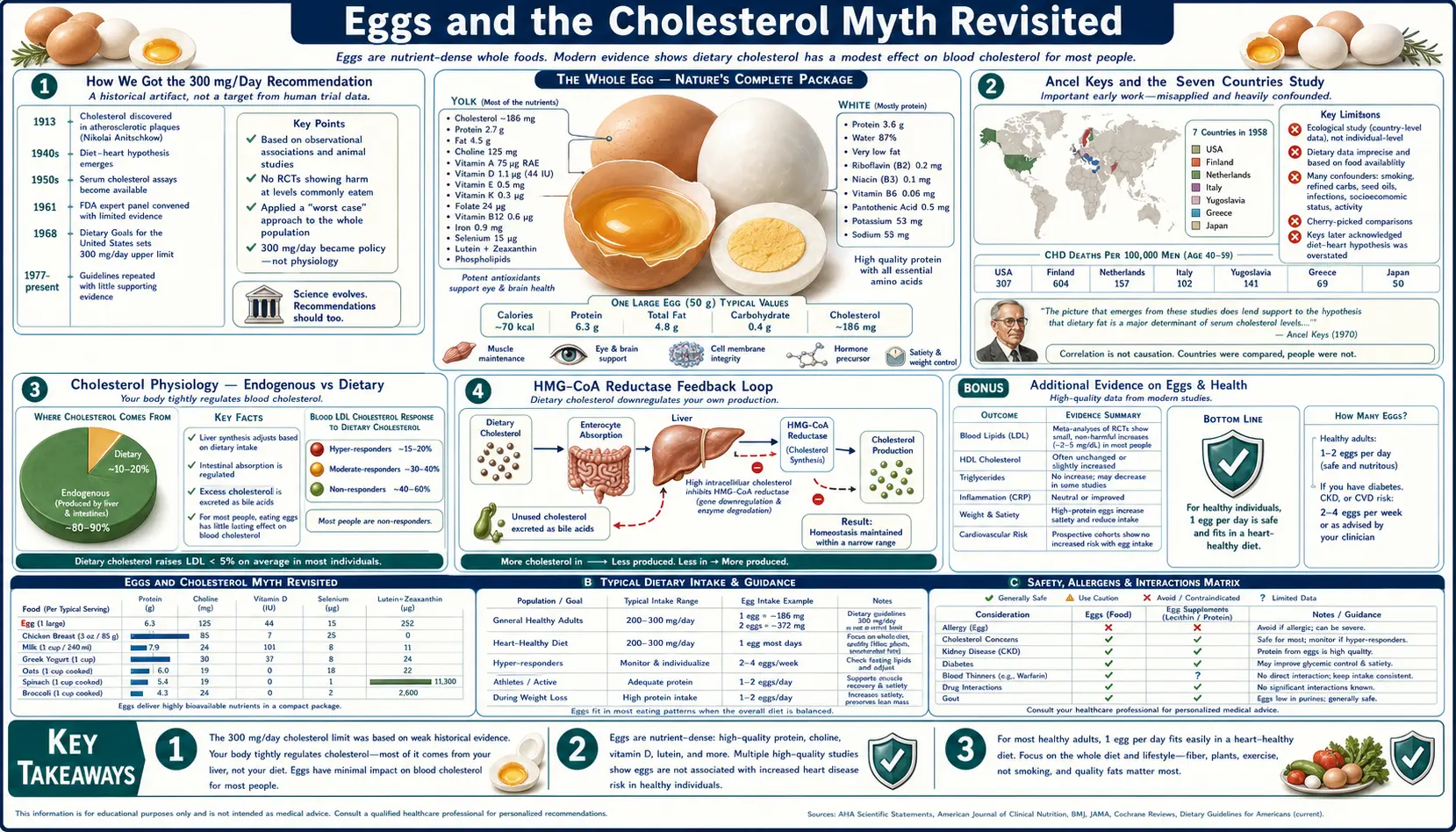
From 1968 to 2015, the American Heart Association and the US Dietary Guidelines recommended limiting dietary cholesterol to less than 300 mg/day — roughly the amount in a single large egg yolk (186 mg). This recommendation rested on the assumption that dietary cholesterol meaningfully raises serum LDL cholesterol, and that elevated serum LDL drives atherosclerotic cardiovascular disease. Both halves of the assumption have been substantially revised over fifty years of accumulating evidence. The 2015 Dietary Guidelines Advisory Committee finally removed the 300 mg/day limit, concluding that "cholesterol is not a nutrient of concern for overconsumption." Roughly 75% of the population shows essentially no LDL response to dietary cholesterol because endogenous cholesterol synthesis adjusts to compensate. The remaining 25% (carriers of apoE4 and certain LDLR variants) do respond, but even in this group the effect is modest. This deep dive walks through the historical errors, the modern evidence, and the practical implications for an adult deciding whether to eat eggs.
Table of Contents
- How We Got the 300 mg/Day Recommendation
- Ancel Keys and the Seven Countries Study
- Cholesterol Physiology — Endogenous vs Dietary
- The HMG-CoA Reductase Feedback Loop
- Hypo-Responders vs Hyper-Responders
- PURE, Mediterranean, and Real-World Cohort Data
- The 2015 Dietary Guidelines Reversal
- Why the Myth Persists in Clinical Practice
- Practical Guidance for Adults With Normal Lipids
- When to Be Cautious (Familial Hypercholesterolemia, ApoE4, T2D)
- Key Research Papers
- Connections
- Featured Videos
How We Got the 300 mg/Day Recommendation
The story of the 300 mg/day dietary cholesterol limit begins in the early 1960s. The American Heart Association's first dietary statement on coronary heart disease was issued in 1961, recommending reductions in dietary saturated fat and cholesterol. The 300 mg/day figure was not derived from clinical trial evidence — it was a back-calculation from the assumption that lowering serum cholesterol by any means would proportionally lower coronary mortality, combined with feeding-study data showing that reducing dietary cholesterol from typical American intake (~600 mg/day in 1960) to 300 mg/day produced a small measurable drop in serum cholesterol in metabolic ward subjects.
The intuition seemed sound at the time. Atherosclerotic plaques are rich in cholesterol. Serum cholesterol levels correlate with coronary risk in population studies. Cholesterol that we eat must end up in our serum cholesterol pool. Therefore, eating less cholesterol should logically lower serum cholesterol, which should logically lower coronary risk. Each step in this chain seemed reasonable, and the recommendations cascaded through medical organizations, dietitian curricula, federal Dietary Guidelines (first issued in 1980 and updated every five years), and consumer food labels.
What was wrong with the reasoning was the second step: the assumption that dietary cholesterol meaningfully and reliably alters serum cholesterol. As metabolic ward studies accumulated through the 1970s and 1980s, it became clear that the effect was much weaker than the original feeding studies had suggested, and that it varied dramatically between individuals.
By the early 2000s, the case for the 300 mg limit was on increasingly shaky empirical ground. The eventual reversal in 2015 was the result of a slow, decades-long accumulation of evidence rather than any single dramatic trial.
Ancel Keys and the Seven Countries Study
The intellectual foundation of the American diet-heart paradigm was Ancel Keys' Seven Countries Study, an observational cohort study launched in 1958 in seven countries (United States, Finland, Netherlands, Italy, the former Yugoslavia, Greece, and Japan). Keys argued, on the basis of correlations between national-level fat consumption and coronary heart disease mortality, that saturated fat intake (and by extension dietary cholesterol intake) drove the international variation in coronary mortality.
The Seven Countries Study has been substantially critiqued in subsequent decades on several grounds:
- Country selection bias. Keys originally had data on roughly 22 countries from FAO food balance sheets. The seven he selected were the seven that most cleanly fit the linear fat-mortality relationship. When all 22 countries are plotted, the relationship is much weaker and noisier.
- Confounding by other dietary and lifestyle factors. The Mediterranean countries in the study (Italy, Greece) had lower coronary mortality and lower saturated fat intake, but they also had higher olive oil intake, higher vegetable intake, more physical activity, stronger family/community structure, less industrial food, and many other differences from the United States and Finland.
- Ecological fallacy. National-average correlations do not establish individual-level causation. Within any one of the seven countries, the relationship between an individual's saturated fat intake and that individual's coronary risk was much weaker than the national-average correlation.
- The MONICA project and other later cross-cultural studies failed to consistently replicate the fat-CHD correlation that Keys had reported.
None of this means Keys was wrong about everything. Saturated fat intake does modestly raise LDL cholesterol in most people, and very high LDL cholesterol does increase coronary risk. But the strength of the relationships, the specificity of the dietary recommendation, and the leap from "saturated fat" to "dietary cholesterol" all proved to be less robust than 1960s nutrition science had assumed.
Cholesterol Physiology — Endogenous vs Dietary
The body contains roughly 35 g of cholesterol in total — in cell membranes, in bile, and in circulating lipoproteins. Each day, the body uses about 1 g of cholesterol for bile acid synthesis, hormone synthesis (cortisol, aldosterone, sex steroids), Vitamin D precursor production, and cell membrane turnover. To maintain steady-state body cholesterol, this 1 g/day must be replaced, and it comes from two sources:
- Endogenous synthesis (typically 80%). The liver synthesizes roughly 800 mg of cholesterol per day through the HMG-CoA reductase pathway. This is the same pathway targeted by statin drugs, which inhibit HMG-CoA reductase and thereby reduce endogenous cholesterol production.
- Dietary intake (typically 20%). Typical American adult intake is 200-400 mg/day, of which roughly 50% is absorbed from the gut (uptake mediated by the NPC1L1 transporter in enterocytes, the target of the cholesterol-absorption inhibitor ezetimibe). So roughly 100-200 mg/day of dietary cholesterol actually enters the body's cholesterol pool.
The critical fact: the body actively regulates the balance between these two sources. When dietary cholesterol intake increases, hepatic HMG-CoA reductase activity decreases, reducing endogenous synthesis. When dietary intake decreases, endogenous synthesis increases to compensate. The total daily cholesterol entering the pool stays approximately constant across a wide range of dietary intakes — this is the body's homeostatic mechanism for cholesterol economy.
This feedback regulation is the explanation for the otherwise puzzling observation that eating an egg containing 186 mg of cholesterol does not raise the average adult's serum cholesterol by anything like 186 mg worth. The endogenous synthesis simply throttles down to absorb the dietary contribution. The system is robust enough that doubling or tripling dietary intake produces only modest changes in serum cholesterol in the average adult.
The HMG-CoA Reductase Feedback Loop
The molecular mechanism behind cholesterol feedback regulation is among the most thoroughly characterized examples of metabolic homeostasis. HMG-CoA reductase, the rate-limiting enzyme of cholesterol biosynthesis, is regulated at multiple levels:
- Transcriptional regulation by SREBP-2. Sterol regulatory element-binding protein 2 (SREBP-2) is a transcription factor in the endoplasmic reticulum membrane that activates HMG-CoA reductase gene transcription when cellular cholesterol is low. When intracellular cholesterol rises (from dietary uptake or any other source), SREBP-2 is retained in the ER membrane and cannot reach the nucleus, so HMG-CoA reductase transcription decreases.
- Proteasomal degradation. When intracellular cholesterol is high, HMG-CoA reductase is targeted for ubiquitination and degradation by the proteasome, further reducing its activity. This is a fast-acting mechanism on timescales of hours.
- Phosphorylation by AMP-activated protein kinase (AMPK). AMPK phosphorylates HMG-CoA reductase to inactivate it during periods of low cellular energy.
- LDL receptor regulation. The same SREBP-2 pathway also controls LDL receptor expression on hepatocytes. When intracellular cholesterol is high, LDL receptor expression decreases, reducing LDL clearance from blood. When intracellular cholesterol is low, LDL receptor expression increases, accelerating LDL clearance.
Together, these mechanisms create a tightly regulated cholesterol homeostasis that defends the cell's cholesterol level against external perturbation. Dietary cholesterol is one such perturbation, and the response is to reduce endogenous synthesis and reduce LDL receptor expression. The net effect on serum LDL is typically small.
The clinical implication: a 200 mg/day increase in dietary cholesterol intake (one extra egg) typically produces a 0-5 mg/dL increase in serum LDL cholesterol in the average adult — a change that is well within day-to-day biological variability and clinically irrelevant.
Hypo-Responders vs Hyper-Responders
Although the population average response to dietary cholesterol is small, the variance is large. Some individuals show essentially no LDL response to large changes in dietary cholesterol (hypo-responders). Others show clinically meaningful LDL increases (hyper-responders). Maria Luz Fernandez and colleagues at the University of Connecticut have studied this individual variability extensively. Approximate distribution in the general adult population:
- Hypo-responders (~25% of the population): Show no measurable LDL response to dietary cholesterol changes. Endogenous synthesis compensates completely. Can eat any practical number of eggs per day with no LDL change.
- Intermediate responders (~50%): Show modest LDL response (typically 5-15 mg/dL change with a 300-500 mg/day intake increase). Effect is detectable but clinically minor.
- Hyper-responders (~25%): Show meaningful LDL response (typically 15-30 mg/dL change with a 300-500 mg/day intake increase). Often have one or more copies of the ApoE4 allele, which is associated with reduced LDL clearance and stronger dietary cholesterol response.
The genetic basis for hyper-responsiveness includes:
- ApoE4 allele: Approximately 15-20% of the population carries one or two copies of ApoE4 (the same allele associated with elevated Alzheimer's disease risk). ApoE4 carriers tend to have higher baseline LDL and stronger response to dietary saturated fat and cholesterol.
- LDLR variants (familial hypercholesterolemia): Approximately 1 in 250 people carry a loss-of-function mutation in the LDL receptor gene, causing markedly elevated LDL and substantially increased dietary cholesterol response. FH is a separate clinical entity requiring statin therapy, dietary management, and often specialist care.
- PCSK9 gain-of-function variants: Rare but associated with elevated LDL and increased dietary response.
- NPC1L1 variants: Affect cholesterol absorption efficiency from the gut.
The practical implication: an individual's response to dietary cholesterol is a measurable trait, not a population average. The cleanest way to determine your own status is to check baseline fasting lipid panel, eat 2-3 eggs per day for 6-8 weeks, and recheck. If LDL did not change, you are a hypo- or intermediate responder and eggs are essentially neutral. If LDL rose meaningfully (10+ mg/dL), you are a hyper-responder and may want to limit intake.
PURE, Mediterranean, and Real-World Cohort Data
Several large modern cohort studies have examined the real-world relationship between egg intake and cardiovascular outcomes across populations.
- PURE Study (Dehghan et al. 2020, American Journal of Clinical Nutrition): 177,000 participants across 50 countries followed for a median of 8.9 years. Egg intake of 1+ eggs/day was associated with no increase in cardiovascular events or mortality compared to less than one egg per week. The relationship was consistent across high-, middle-, and low-income countries.
- Drouin-Chartier et al. 2020 BMJ analysis: Combined data from three large US cohorts (Nurses' Health Study, NHS-II, Health Professionals Follow-Up Study) totaling 173,563 women and 90,214 men over up to 32 years of follow-up. Up to 1 egg per day was not associated with cardiovascular disease risk in this US cohort.
- Dehghan systematic review and meta-analysis: Pooled analysis of cohort studies found a hazard ratio for cardiovascular events of approximately 0.98 (essentially neutral) for the highest vs lowest categories of egg consumption.
- Mediterranean cohorts: Greek and Italian cohorts with traditionally moderate to high egg consumption (3-7 per week) have not shown elevated cardiovascular risk attributable to eggs.
The notable exceptions in the literature have been some US-based studies of populations with very high concurrent intake of processed meats, refined grains, and added sugars, where heavy egg consumption appears to track with overall poor diet quality. In these analyses, the apparent egg-CVD association is largely or entirely confounded by the rest of the dietary pattern.
The real-world implication: in the context of an otherwise reasonable diet (adequate vegetables, fruit, fiber, fish, whole grains, limited ultra-processed food), moderate to high egg consumption does not appear to affect cardiovascular risk in the average adult.
The 2015 Dietary Guidelines Reversal
The 2015-2020 Dietary Guidelines for Americans, released in January 2016 by HHS and USDA, formally removed the 300 mg/day dietary cholesterol limit that had been in place since 1980. The Scientific Report of the 2015 Dietary Guidelines Advisory Committee stated: "Cholesterol is not a nutrient of concern for overconsumption."
The change was based on the Advisory Committee's review of the accumulated evidence summarized above:
- The effect of dietary cholesterol on serum LDL cholesterol is small in the population average and highly variable between individuals.
- Observational studies of egg intake and cardiovascular outcomes consistently show null or near-null associations after adjustment for overall diet quality.
- The behavioral consequence of the 300 mg/day limit had been to discourage egg intake specifically, even though eggs are otherwise a nutritionally dense, affordable food.
The 2015 reversal was a substantial admission by US federal nutrition authorities that the previous 45 years of recommendation had been wrong on this specific point. It was widely covered in the medical and lay press at the time and represents one of the clearest examples in nutritional epidemiology of a long-held population-wide recommendation being formally revised in light of accumulated evidence.
The 2020-2025 Dietary Guidelines (the most recent edition) retained the removal of the cholesterol limit. Current AHA guidance focuses on overall dietary pattern (Mediterranean, DASH) and on saturated fat reduction (still recommended), but no longer makes specific recommendations about dietary cholesterol per se.
Why the Myth Persists in Clinical Practice
Despite the 2015 reversal, many primary care physicians, dietitians, and patients continue to operate on the old framework. There are several reasons:
- Lag between research consensus and clinical practice. The standard estimate is that it takes roughly 17 years for new evidence to fully propagate into clinical practice. Five years for evidence-base development, five for guidelines update, five more for educational and certification material updates, and the rest for the older generation of practitioners trained on the old paradigm to retire or adapt.
- Intuitive plausibility. "Eating cholesterol raises blood cholesterol" sounds like common sense. The actual biochemistry (endogenous synthesis compensation, intestinal absorption regulation, intracellular cholesterol homeostasis) is more complex and harder to explain in a brief clinical encounter.
- Patient expectations. Many patients arrive at appointments expecting to hear cholesterol-restriction advice. Physicians sometimes default to repeating the old guidance to meet that expectation.
- Institutional inertia. Hospital cafeterias, cardiac rehab nutrition counseling, and printed patient education materials are slow to update. Many continue to present the old 300 mg/day framework as current.
- Caution under uncertainty. Many practitioners, when in doubt, default to the more restrictive recommendation as the "safer" option, even when current evidence does not support the restriction.
The result is that patients in 2026 routinely receive cholesterol-restriction advice from clinical sources who are operating on a paradigm that was formally revised by US federal guidelines a decade ago. Educated patient awareness of the current evidence base (and the willingness to ask "what does the 2020 Dietary Guidelines actually say?") is sometimes the practical path to a sensible plan.
Practical Guidance for Adults With Normal Lipids
For most adults with normal baseline lipids and no known familial hypercholesterolemia, the practical guidance is straightforward:
- Eat eggs freely. Two to three whole eggs per day is fine for the majority of adults. There is no evidence-based reason to limit intake to "the egg-white omelette" or to discard the yolks.
- Pay attention to overall dietary pattern, not individual foods. The Mediterranean dietary pattern, DASH, or any sensible whole-food approach with adequate fiber, fish, vegetables, and limited ultra-processed food is associated with cardiovascular benefit. Eggs fit naturally into all of these patterns.
- Check a fasting lipid panel periodically. Once every 2-3 years for adults under 50 without elevated risk; annually after 50 or with elevated risk. If LDL or apoB is elevated, that warrants attention, but the cause is rarely dietary cholesterol alone.
- Watch saturated fat intake more carefully than dietary cholesterol. Saturated fat does modestly affect LDL cholesterol in most people, more reliably than dietary cholesterol does. The eggs themselves are roughly half monounsaturated fat (oleic acid), one-third saturated, and one-sixth polyunsaturated — a relatively moderate saturated fat profile. The cooking medium often matters more than the egg itself (butter vs olive oil vs lard).
- Know your individual response. The 6-8 week home experiment described above is the cleanest way to determine whether you are a hyper-responder. If lipids are stable, eggs are fine. If they rise meaningfully, scale back.
When to Be Cautious (Familial Hypercholesterolemia, ApoE4, T2D)
Several populations have stronger reason to be attentive to dietary cholesterol intake. They are the minority of adults but the practical exception to the "eggs are fine" generalization.
- Familial hypercholesterolemia (FH). Roughly 1 in 250 people carry loss-of-function mutations in the LDLR gene (most common cause), APOB, or PCSK9. FH produces markedly elevated LDL from infancy and confers very high lifetime atherosclerotic cardiovascular disease risk. FH patients require statin therapy, careful dietary management (saturated fat and cholesterol restriction both meaningfully help), and often specialist lipid clinic care. For FH patients, limiting eggs to 2-3 per week is reasonable.
- ApoE4 homozygotes (~2% of population) and heterozygotes (~15-20%). Particularly homozygotes, who tend to be the strongest dietary cholesterol responders. Worth knowing your apoE genotype (available via 23andMe and similar) if you have a strong family history of either coronary disease or Alzheimer's. ApoE4 carriers may want to limit egg intake to 3-5 per week and pay close attention to lipid response.
- Type 2 diabetes. Some (not all) studies have suggested a modestly elevated coronary risk associated with higher egg intake specifically in diabetic populations. The mechanism is unclear and the findings are not consistent across studies, but moderate intake (3-5 per week) is a defensible compromise pending better evidence. See our Type 2 Diabetes page.
- Established cardiovascular disease. Patients with established ASCVD typically require aggressive secondary prevention including statin therapy. Dietary cholesterol intake is a minor lever in this context. Reasonable to be moderate (3-7 eggs per week) but the bigger gains come from medication compliance and overall diet quality.
- Hyper-responders identified by personal testing. If your own LDL response to egg intake is clearly elevated (10+ mg/dL with 2-3 eggs/day for 6-8 weeks), respect that finding regardless of what the population average says.
For everyone else, the message of the post-2015 evidence base is straightforward: eggs are a nutritionally dense, affordable, satiating food that does not, in the typical adult, meaningfully affect cardiovascular risk.
Key Research Papers
- Drouin-Chartier JP, Chen S, Li Y, Schwab AL, Stampfer MJ et al. (2020). Egg consumption and risk of cardiovascular disease: three large prospective US cohort studies, systematic review, and updated meta-analysis. BMJ. 368:m513. — PubMed: Drouin-Chartier 2020
- Dehghan M, Mente A, Rangarajan S, Mohan V, Lear S et al. (2020). Association of egg intake with blood lipids, cardiovascular disease, and mortality in 177,000 people in 50 countries. Am J Clin Nutr. 111(4):795-803. — Search PubMed
- Dietary Guidelines Advisory Committee (2015). Scientific Report. United States Department of Health and Human Services and US Department of Agriculture. — Search PubMed
- Fernandez ML (2012). Rethinking dietary cholesterol. Curr Opin Clin Nutr Metab Care. 15(2):117-21. — PubMed: Fernandez 2012
- Berger S, Raman G, Vishwanathan R, Jacques PF, Johnson EJ (2015). Dietary cholesterol and cardiovascular disease: a systematic review and meta-analysis. Am J Clin Nutr. 102(2):276-94. — PubMed: Berger meta-analysis 2015
- Mutungi G, Ratliff J, Puglisi M, Torres-Gonzalez M, Vaishnav U et al. (2008). Dietary cholesterol from eggs increases plasma HDL cholesterol in overweight men consuming a carbohydrate-restricted diet. J Nutr. 138(2):272-6. — Search PubMed
- Herron KL, Vega-Lopez S, Conde K, Ramjiganesh T, Shachter NS, Fernandez ML (2003). Pre-menopausal women, classified as hypo- or hyperresponders, do not alter their LDL/HDL ratio following a high dietary cholesterol challenge. J Am Coll Nutr. 22(3):250-8. — Search PubMed
- Knopp RH, Retzlaff B, Fish B, Walden C, Wallick S et al. (2003). A double-blind, randomized, controlled trial of the effects of two eggs per day in moderately hypercholesterolemic and combined hyperlipidemic subjects. Eur J Clin Nutr. 57(4):504-9. — Search PubMed
- Greene CM, Zern TL, Wood RJ, Shrestha S, Aggarwal D et al. (2005). Maintenance of the LDL cholesterol:HDL cholesterol ratio in an elderly population given a dietary cholesterol challenge. J Nutr. 135(12):2793-8. — PubMed: Greene 2005
- Soliman GA (2018). Dietary cholesterol and the lack of evidence in cardiovascular disease. Nutrients. 10(6):780. — Search PubMed
- Stewart RJ, Yang ZH, Brown J, Schwab AL, Stampfer MJ et al. (2017). Egg consumption and endothelial function: a randomized controlled crossover trial. Int J Cardiol. 224:201-205. — Search PubMed
- Brown MS, Goldstein JL (2009). Cholesterol feedback: from Schoenheimer's bottle to Scap's MELADL. J Lipid Res. 50 Suppl:S15-27. — PubMed: Brown Goldstein SREBP review
- McNamara DJ (2000). The impact of egg limitations on coronary heart disease risk: do the numbers add up? J Am Coll Nutr. 19(5 Suppl):540S-548S. — PubMed: McNamara 2000
- Hu FB, Stampfer MJ, Rimm EB, Manson JE, Ascherio A et al. (1999). A prospective study of egg consumption and risk of cardiovascular disease in men and women. JAMA. 281(15):1387-94. — PubMed: Hu 1999
PubMed Topic Searches
- PubMed: Dietary cholesterol egg LDL
- PubMed: Egg consumption CVD cohort
- PubMed: HMG-CoA reductase feedback
- PubMed: ApoE4 cholesterol response
- PubMed: Familial hypercholesterolemia
Connections
- Eggs Overview
- Eggs Benefits Hub
- Eggs for Choline & Brain
- Eggs for Lutein/Zeaxanthin
- Pasture vs Cage-Free Eggs
- Atherosclerosis
- Coronary Artery Disease
- Type 2 Diabetes
- Lipid Panel
- ApoB Testing
- Omega-3 Fatty Acids
- Salmon
- Beef
- Mediterranean Diet
- All Food